
Abstract
Abstract
Objective:
To present the primary results of laparoscopic, Burch-type colposuspension (LBC) in children.
Patients and Methods:
LBC was performed in eight children (mean age, 14 years) with urinary incontinence after failed extensive urotherapy program. In all patients, bladder neck (BN) incompetence was proven by clinical observation, perineal ultrasound (US), and video-urodynamic study (V-UDS). The LBC was performed with patients in the lithotomy position by means of three 5-mm ports. The anterior wall of the vagina, lateral to the BN, was mobilized, and the vaginal wall was bilaterally lifted and sutured to Cooper's ligament, resulting in elevation and fixation of the BN. A catheter was left for 4 days. The mean operation time was 101 minutes (range, 56–150 minutes), and the follow-up time was >6 months.
Results:
The postoperative period was uneventful for all patients. Shortly after the procedure, 5 patients (62.5%) were dry, and 1 patient improved (12.5%). After 6 months, 3 patients (37.5%) were dry, and 2 (25%) improved. In 3 wet patients, control US and V-UDS focused on the BN revealed hypermobility and persistent flat vesicourethral angle (VUA) in 1 patient, hypermobility with a good restoration of the VUA in 1 patient, and good fixation with good restoration of the VUA in 1 patient.
Conclusions:
LBC is a challenging procedure in children because of the small operation field. This procedure can be considered to cure refractory stress urinary incontinence in children with BN insufficiency when noninvasive methods have failed.
Introduction
T
Girls with lower urinary tract symptoms and coexisting stress incontinence can mostly be cured by urotherapy and physical therapy. Only a few patients have persistent incontinence based on congenital bladder neck (BN) insufficiency and obtain a tertiary referral for surgery after failed conservative and pharmaceutical treatments. Previously, we published our results of open colposuspension for refractory incontinence. 6
The aim of this study is to present the challenges and primary results of laparoscopic, Burch-type colposuspension (LBC) in pediatric patients.
Subjects and Methods
Between April 2011 and June 2012, eight girls between 10 and 15 years of age (mean, 14 years) had an LBC. All children had stress incontinence; two of them also had urge incontinence. All girls received our standard diagnostic work-up in the outpatient clinic, which includes the following: a bladder and bowel diary, at least two uroflowmetry tests with ultrasound (US) measurement of residual urine, a physical examination with extensive focus on lumbosacral neurological functioning, and standard US of kidneys and bladder. At our department all wet children undergo a perineal US that is focused on the BN position and mobility during straining, pelvic floor command, and measurement of urethral length and position in rest and during coughing and straining. For this purpose the C9-4 probe is put between the labia at the level of the meatus urethrae. The symphysis, bladder, BN, urethra, and pelvic floor muscle complex are identified and examined. This technique has been previously described. 7 There is little known about the normal values of these parameters, but the first normograms have been presented. 8 All individuals had failed a 3-month outpatient urotherapy training. A video-urodynamic study (V-UDS) was performed, followed by 2 weeks of in-hospital training that was focused on the pelvic floor coordination. Those with urge incontinence had been given antimuscarinics without relief of symptoms. Any girls after this treatment who were proven to suffer from therapy-resistant incontinence, based on BN insufficiency, were considered as candidates for surgery. Reevaluation of the patients was performed and showed a continuously open and hypermobile bladder neck with a relatively flat vesicourethral angle (VUA) on perineal US. The V-UDS was repeated with special interest in the BN anatomy and function. The BN was considered incompetent if the following features were seen: an open BN during filling phase; a hypermobile BN, which meant >2 cm descent during straining; a flat VUA; and often, also, a cystocele during straining and voiding (Figs. 1 and 2). When incontinence could not be masked by wearing simple pads and both the urotherapist and the patient considered that the impact on the quality of life was serious, a colposuspension procedure was proposed for those patients. Average duration of failed conservative and pharmaceutical treatment in these girls was 2.5 years.
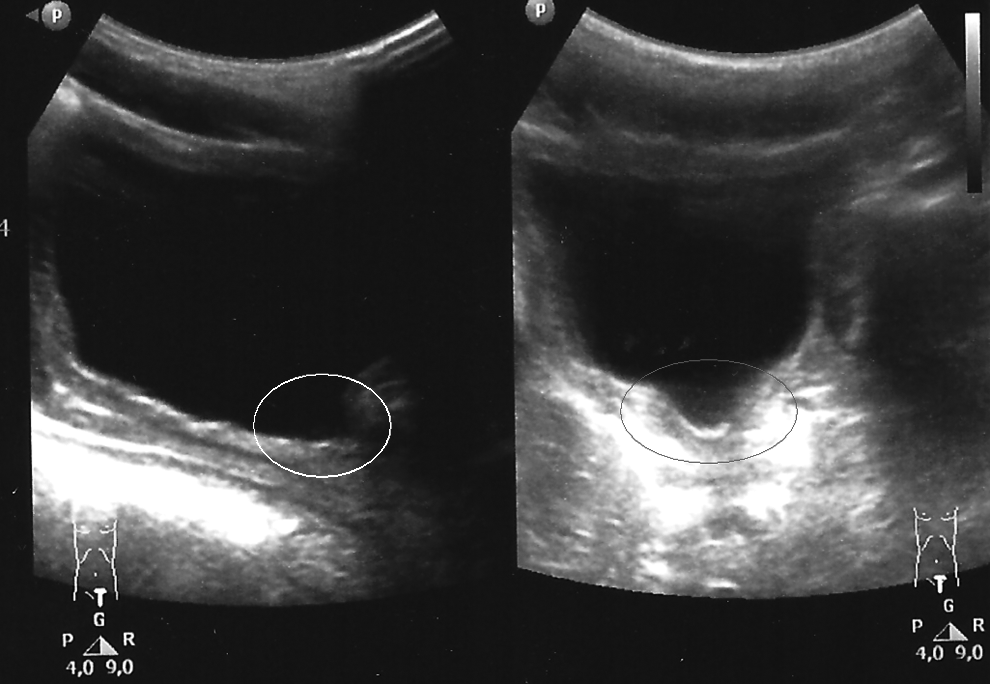
Transabdominal ultrasound: open bladder neck (circle).
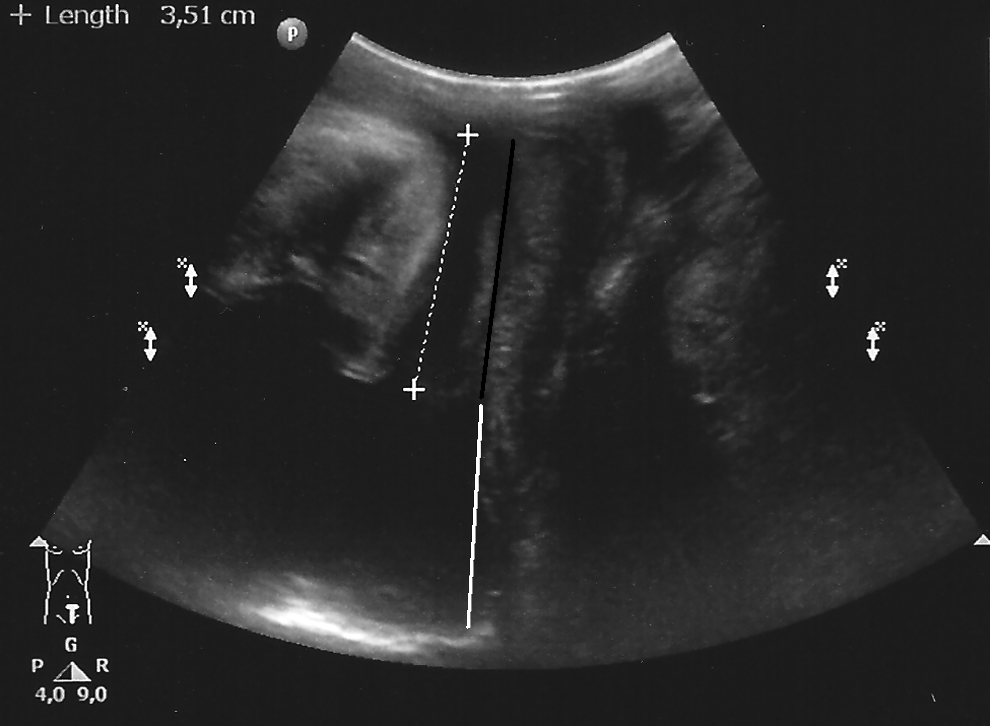
Perineal ultrasound: flat vesicourethral angle (parallel lines).
The technique
Surgery is performed with the patient in the lithotomy position, and urethrocystoscopy is performed to evaluate the anatomy of the lower urinary tract. A balloon catheter is inserted into the bladder. The operating surgeon is on the left side of the patient. The first 5-mm port is introduced below the umbilicus. The 30° telescope is used bluntly to first pass the preperitoneal space and then caudally, in front of the bladder, to enter the prevesical space at the level of the BN. In the first 5 cases, the space between the rectus fascia and the peritoneum was created in the midline. In cases 6–8, the anterior sheath of the rectus fascia was incised right to the midline, and the rectus muscle was spread to reach the posterior sheath of the rectus fascia. In this way, the Retzius space could be easily approached with minimal risk for peritoneal injury. The CO2 insufflator setting are 8 mm Hg pressure and 4 L/minute flow. Two 5-mm ports are inserted left and right of the midline in the suprapubic region. Gentle traction of the catheter enables identification of the level of the BN during the laparoscopic surgery. The endopelvic fascia is opened. The BN and the anterolateral wall of the vagina are identified and freed by monopolar cautery. The vaginal wall is pushed up left and right of the BN using an intravaginal clamp to determine the optimal area for the suspending stitches. Polyglactin sutures (2-0) are passed through the vaginal wall and through Cooper's ligament, and they are knotted while the anterior vaginal wall is pushed upward from inside the vagina (Fig. 3). In the first 3 cases, the stitches were placed first on both sides, and the knots were completed afterward. In the later 5 cases, the stitches were inserted singly, beginning on the left side. In 4 patients, one stitch on the left and one on the right side were enough to achieve an appropriate elevation of the BN (Table 1). Finally, cystoscopy is performed to assess the correct level of suspension and the restoration of a normal VUA and to ensure that no sutures have entered the bladder. The mean operative time was 101 minutes (range, 56–150 minutes).
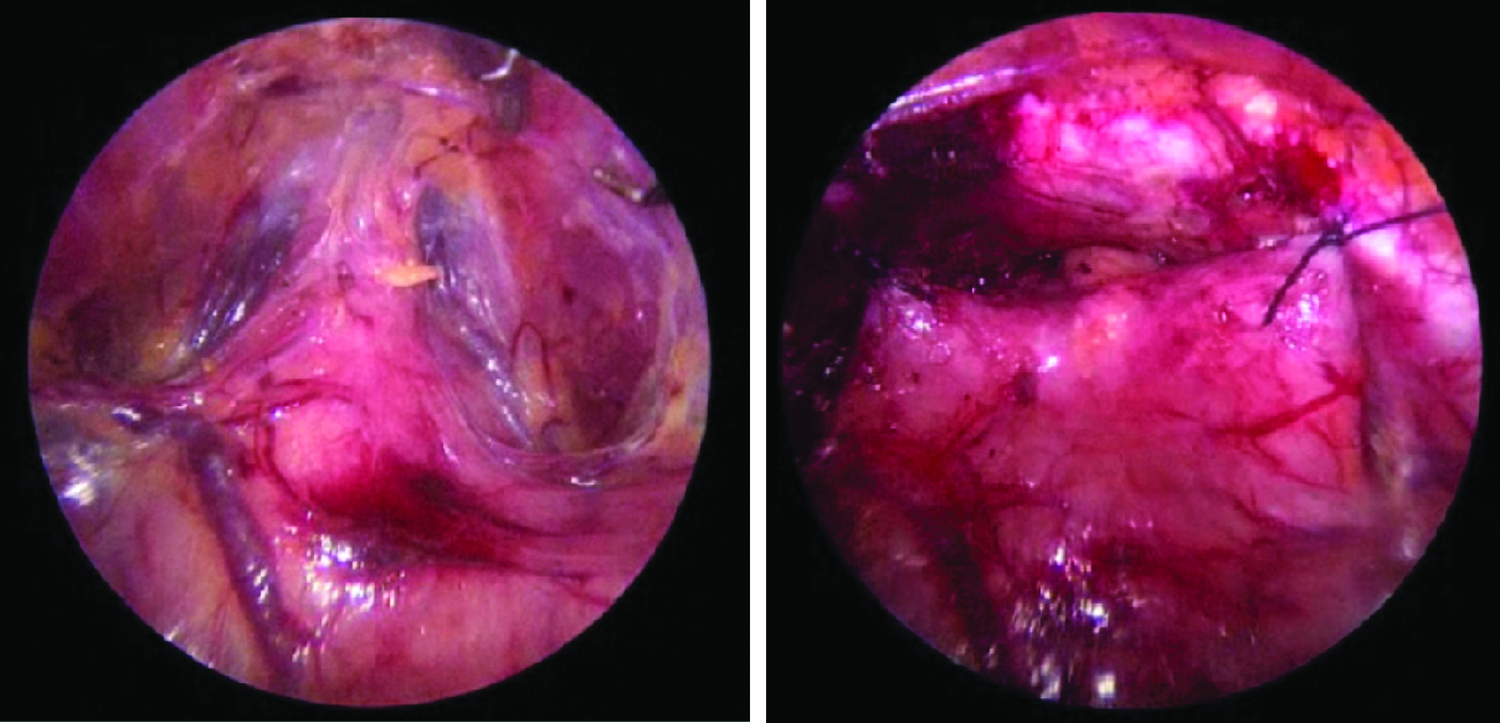
Intraoperative views:
BC, bladder capacity; BN, bladder neck; DOA, detrusor overactivity; DV, dysfunctional voiding; L, left side; PVR, post-void residual; R, right side; rUTI, recurrent urinary tract infections; SUI, stress urinary incontinence; UI, urge incontinence; VUA, vesicourethral angle.
A transurethral catheter is left in position for 4 days. The patient is asked not to perform any sport exercises for a period of 6 weeks and not to lift objects of more than 7.5 kg for a period of 3 months. The results were assessed 3 and 6 months after surgery. Definition of success was as follows: dryness when no incontinence was present or improvement when the number of wet episodes was diminished.
Results
The postoperative course was uneventful in all patients. No urinary retention was observed. In 1 patient, injury of the peritoneum occurred during the port introduction. An intravenous cannula was inserted percutaneously to decompress the intraperitoneal space without the need for conversion.
Shortly after the procedure 5 patients (62.5%) were dry, and 1 improved (12.5%). At the 6-month follow-up, 3 patients (37.5%) were dry, and 2 (25%) had fewer than 50% of wet incidents compared with preoperatively. In 3 patients who were wet, a control US as well as V-UDS was performed. The BN was still hypermobile with a flat VUA in 1 patient, was hypermobile with a good angle in 1 patient, and was well fixed to the symphysis with a good VUA in 1 patient.
One patient who improved is scheduled for a V-UDS. One patient was dry after surgery but relapsed after a motorbike accident a few weeks after surgery. Detailed results are presented in Table 2.
BN, bladder neck; DOA, detrusor overactivity; SUI, stress urinary incontinence; VUA, vesicourethral angle; V-UDS, video-urodynamic study.
Discussion
Urinary incontinence in girls is predominantly a functional problem based on abnormal detrusor or/and sphincter functions. In rare cases, incontinence is based on congenital insufficiency of the BN. Conventional urotherapy is used in children with functional disorders. Pharmacological treatment and additional physical therapy can help in some patients. 4 Careful reevaluation of the patient with refractory incontinence should be done by history and stress tests. Neuropathic disorders must be excluded. Anatomical anomalies of the lower urinary tract must be reconsidered. US of the pelvic floor and V-UDS can provide useful information regarding the anatomy and the function of the lower urinary tract. 9 In a few girls, BN insufficiency can be detected. The signs of this phenomenon include the following: continuously open BN during filling phase, hypermobility of the BN, a cystocele during straining, and absence of a VUA. An open BN identified by US can be observed frequently in girls with dysfunctional voiding, even after successful urotherapy.
SUI based on BN insufficiency is very common in adult women. BN suspension by means of fixation of the anterolateral vaginal wall to Cooper's ligament was proposed by Burch in 1961. 10 The success rate of this procedure is between 85% and 90% in the first year, with a relapse rate up to 20% after a longer follow-up. The results of the open colposuspension and LBC are similar, where the latter has a lower complication rate and shorter hospital stay (level of evidence 1A). During recent years the midurethral slings have become the first-line treatment in the adult population, but the Burch procedure still has a “grade A” recommendation and should be offered to patients when a midurethral sling cannot be used. The open colposuspension is also a recommended option after a failed midurethral sling operation.11,12
A general rule in our department is not to use artificial slings in children because of the lack of space in the prepubertal vagina and insufficient data on the possibility of having a vaginal birth after an artificial sling procedure. In neurogenic lower urinary tract dysfunction, a rectus fascia sling procedure is our first choice. A colposuspension can be performed on children with SUI and mixed urinary incontinence based on BN insufficiency.
We previously published our results of using the open Burch colposuspension in a pediatric population. 6 The overall success rate was 54% for dry and 15% for symptom improvement. The laparoscopic technique provides dryness and improvement in 62.5% of patients, which is similar to the results of the open approach. However, SUI disappeared completely in 5 patients and was improved in 1 patient (75%). A similar success rate, defined as “no SUI on control urodynamics,” has been published for an adult population. 13 To our knowledge, there is no literature on LBC in children; hence, there is no study with which to compare our results. In 1 case that had a failed endoscopic procedure, a re-do open colposuspension was performed but unfortunately was also unsuccessful. Because of the small number of patients, no conclusion can be drawn on how to improve the results. SUI is an uncommon problem in the pediatric population, and the criteria of BN incompetence are not well established yet. The inclusion criteria as well as the other pre- and postoperative factors can have an influence on the outcome.
Technical challenges of the endoscopic technique are related to the limited operating space in children. In addition, the short distance between the suprapubic ports can be challenging. Small needles must be used (we used polyglactin 2-0 RB), and sliding knots can be advantageous. Blunt insertion of the first port increases the risk for peritoneum injury and gas leakage. To prevent this, we began to insert the port through the rectus muscle. By spreading this muscle in the caudal direction, the linea arcuata is approached, and the prevesical space can be reached. After introduction of these improvements, the operating time decreased from 130–140 minutes in the first patients to approximately 80 minutes in the later patients. We have chosen for the preperitoneal approach to get direct access to the BN and the vaginal walls and to avoid intraperitoneal surgery, but we do not claim that this approach is superior to the transperitoneal one.
The success rate in our series was lower than the literature reports for adults. Several factors might be responsible for this: (1) These individuals are complicated cases of refractory incontinence with many additional problems (chronic constipation in 1 case, lack of patient's compliance in 1 case, and small bladder volume in 1 case). (2) The indications for this procedure in children are not well established. Colposuspension can be offered to girls with refractory incontinence based on BN insufficiency, but careful urodynamic evaluation (US of the pelvic floor and V-UDS) is mandatory. However, significant discrepancy between the clinical outcome (wet) and urodynamic findings can be found. (3) This is our first series, our experience with this technique is limited, and there may be a learning curve. Obviously, the laparoscopic technique provides a very good cosmetic outcome and superior view in the operation field, resulting in improved precision.
Conclusions
LBC is a challenging procedure in children because of the small operation field. This procedure can be considered to cure refractory SUI in children with BN insufficiency when noninvasive methods have failed.
Footnotes
Disclosure Statement
No competing financial interests exist.