
Abstract
Abstract
Objective:
To describe a novel practical technique for trocar placement in extraperitoneal laparoscopic radical prostatectomy (eLRP) and robotic-assisted laparoscopic radical prostatectomy (eRALP) in patients who had lower midline abdominal incisions.
Subjects and Methods:
Between March 1999 and November 2013, 3080 LRPs were performed in our department. In total, 1745 eLRPs and 416 eRALPs were enrolled in the study. Group 1 consisted of 57 cases (45 eLRPs and 12 eRALPs) with median lower incision scars after previous abdominal surgery. Group 2 consisted of the same numbers of patients without previous surgeries after matched-pair analyses was performed according to body mass index, age, and operation style. Demographic, perioperative, and postoperative data were recorded. Additionally, we described our novel practical trocar replacement technique for extraperitoneal approach. Statistical analyses were performed.
Results:
Mean age was 65.6±6.2 years. Mean follow-up was 102.9±24.5 months. There were 12 eRALPs and 45 eLRPs in each group. Demographic, perioperative, and postoperative data were similar in the two groups except for trocar placement time. The trocar placement time was longer in Group 1 than in Group 2 (P<.001). In all patients with previous abdominal surgery with lower abdominal incision scars, we were able to establish trocar placement and correct access to the extraperitoneal space. Moreover, we had no conversions or complications in any patient.
Conclusions:
Our technique seems safe and practical for trocar placements for eLRP and eRALP in patients with lower abdominal incision scars.
Introduction
R
Patient selection criteria have come into question because of increased numbers of cases, and the increasing experience, for these surgical options. However, there are limited contraindications such as an uncorrected hemostasis deficit, active peritoneal inflammatory processes, and severe cardiopulmonary diseases; there are also extraperitoneal LRP (eLRP)- and/or extraperitoneal RALP (eRALP)-specific contraindications such as morbid obesity, high prostate volume, and a narrow and deep pelvis.3,4 In addition, previous abdominal and pelvic surgeries can be another relative contraindication. Although they are relative contraindications for LRP and RALP, they may interfere with the safety and efficacy of the operation.
The first step of these procedures is trocar placement. Thus, most of the surgeons prefer the transperitoneal laparoscopic approach, which allows a wide area for both tissue handling and instrument manipulations. 5
Previous abdominal surgery may produce possible risks such as potential presence of intraabdominal adhesions, and these may be related with increased risk of organ injuries. 6 Laparoscopic transperitoneal entry into the previously operated-on abdomens may usually be associated with injuries to the gastrointestinal tract and major blood vessels. The reported complication rates in the literature vary between 0.12% and 1.38%. 7 Moreover, intraabdominal adhesions require more effort, and the risk of visceral organ injuries increase. 7 On the other hand, the extraperitoneal approach can provide some advantages such as rapid access to the Retzius space and decreased risk of intraabdominal organ injuries.8,9 The eLRP is feasible as it can overcome the possible complications and limitation of the transperitoneal approach.10,11
One of the major and important steps of the eLRP is to enter accurately and to create the extraperitoneal space in a safe way, as well as in the eRALP. Despite the well-known advantages of eLRP and eRALP, there are limited published data on the access technique for challenging cases.
Herein, we aimed to describe a novel practical technique for trocar placement in eLRP and eRALP in patients who had lower midline abdominal incisions. According to our knowledge, our study is unique in the literature in that extraperitoneal approaches were described in patients with lower midline incision scars.
Subjects and Methods
All patients fully understood the treatment and aim of this study, and written informed consents were obtained. All data were recorded prospectively using a Microsoft® (Redmond, WA) Office Excel® spreadsheet.
This study is a part of ongoing LRP and RALP studies in our department. Between March 1999 and November 2013, 3080 LRPs were performed in our department. In total, 1745 eLRPs and 416 eRALPs were enrolled in the study.
Patient selection
Patient selection was nonrandomized. There were 57 patients in whom eLRPs (n=45) and eRALPs (n=12) were performed who had lower abdominal incision scars due to previous major abdominal surgeries. The previous surgeries of these patients are listed in Table 1. Group 1 consisted of these patients. Group 2 consisted of the same numbers of patients who had not any previous abdominal or pelvic surgery who met matched-pair criteria. We used the following matched-pair criteria: body mass index (BMI) (in kg/m2), age (years), and operation type (eLRP/eRALP). In particular, BMI is related with obesity, and these two factors are important factors for matched-pair analyses with abdominal anatomy, which can affect directly the laparoscopic entry.
Exclusion criteria were lacking follow-up data, patients needed extended lympadenectomies, and not complying with the matched-pair criteria. In total, 114 patients were enrolled in the study.
Collected data
Demographic data including age, BMI, and prostate-specific antigen (in ng/dL), operative data including operation type, time period for trocar replacements, and estimated blood loss during trocar placement, and postoperative data including pathological reports were recorded.
Operation technique
The patient is placed in a lithotomy position with both arms parallel to the body, and the legs are abducted. The operation table is placed in the 15°–20° Trendelenburg position, and a shoulder support is used for better fixation of the patient.
The first step of the procedure is to create a preperitoneal space and to place the first trocar. The extraperitoneal approach starts with a 12–15-mm median periumbilical incision at the inferior border of the umbilicus (the Hasson technique) (Fig. 1B). 10 A blunt dissection is performed until the anterior rectus sheath is reached. Then, the anterior rectus sheath is incised horizontally, on both sides of the median scar. Then, the longitudinal muscle filaments of the rectus muscle are seen. Then, the space between the rectus muscle and posterior rectus sheath and midline incision scar is created by finger dissections, bluntly, in both sides to the direction of the preperitoneal space (Fig. 1C). The median scar is not incised and/or bluntly dissected by the fingers, so as not to cause an injury to the peritoneum. A10-mm balloon dilating trocar (Herloon; Aesculap, B. Braun Melsungen AG, Tuttlingen, Germany) is introduced gently through this incision, and the extraperitoneal space is then extended carefully up to the pelvis (Fig. 1D and E). Afterward, the extraperitoneal area is seen under direct optic vision through the balloon using the 10-mm scope. The epigastric vessels, which are behind the anterior abdominal wall, compressed ventrally through the balloon, and the median scar line are visualized. The epigastric vessels and the pubic arch are the main landmarks during dilation with the balloon. The lateral part of the pubic arch becomes visible toward the end of the dissection. Subsequently the anterior abdominal wall is elevated ventrally through the facial incisions, by using long blunt hooks. The midline scar is sharply dissected very close to the abdominal wall first, in an open fashion with scissors. The scope is introduced directly through the opening of the extraperitoneal space to permit better visualization of the distal part of the scar tissue. The dissection of the midline scar is then extended caudally under direct endoscopic vision, as distal as possible, by using endoscopic scissors in order to create adequate space (Fig. 1F). The remaining scar tissue is coagulated and cut until the space for proper optical port placement is created.
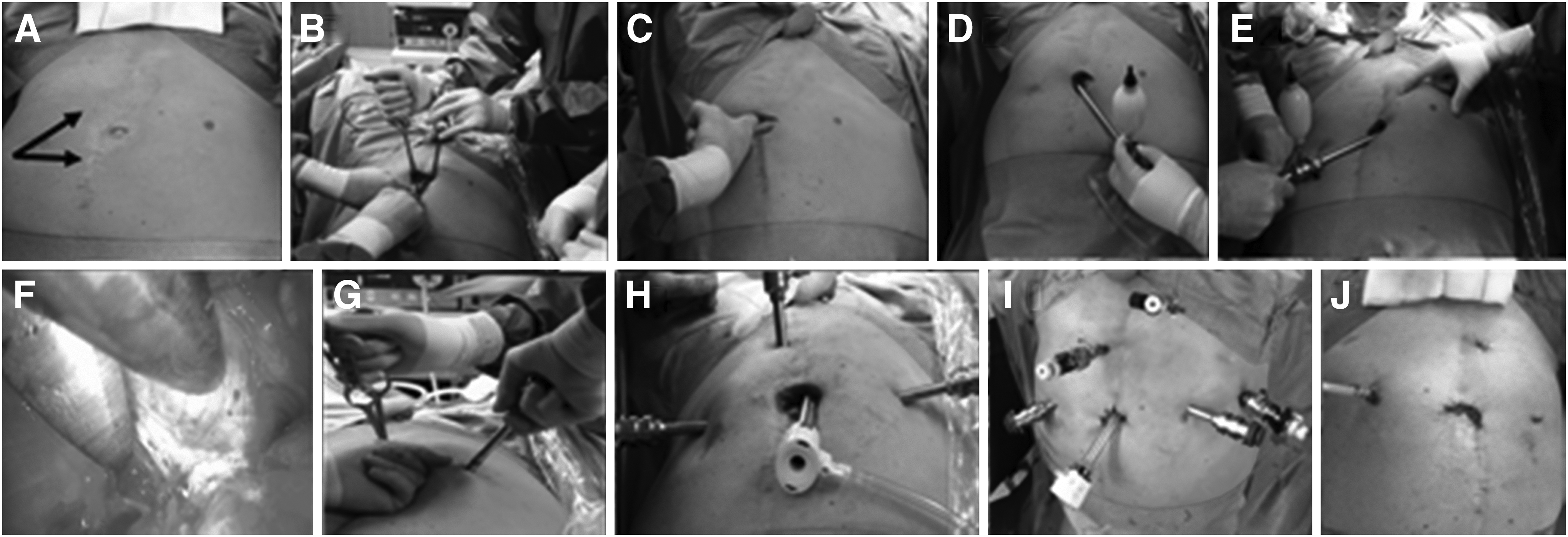
Port arrangements during extraperitoneal laparoscopic/robot-assisted laparoscopic radical prostatectomy.
After the scar is incised until the pubis and a sufficient extraperitoneal space is created, the first three trocars, including two 11-mm working trocars (for robotic cases two 8-mm da Vinci® Surgical System [Intuitive Surgical, Sunnyvale, CA] trocars) and the medial assistant trocars, are placed under digital control (Fig. 1G).
Thereafter, a 12-mm optic port is placed on the midline, and the anterior rectus fascia is closed in an airtight fashion (2/0 polyglactin 910 [Vicryl®; Ethicon, a Johnson & Johnson Company, Cincinnati, OH] sutures).
The extraperitoneal area is explored under optic vision, after establishing the pneumo-extraperitoneum by CO2 gas insufflation (maximum pressure, 15–20 mm Hg; maximum gas flow, 30 mL/second) (Fig. 1H). The remaining adhesions on peritoneum are dissected bluntly and gently. Additionally, these are swept cranially for preparing the area to replace other trocars. The remaining lateral trocars are placed under endoscopic view, and the port placement is arranged in a W-shaped manner (Fig. 1I).
Afterward, an extra 6-mm port is placed on the suprapubic area for retracting and manipulating the prostate during the surgery.
Statistical analyses
Statistical Package for the Social Sciences (SPSS) for Windows software (version 16.0; SPSS Inc., Chicago, IL) was used for statistical analysis. The independent-samples t test was used to compare measurable values, and the Mann–Whitney U test was used for comparisons between the groups. Statistical significance was accepted at P<.05.
Results
Mean age was 65.6±6.2 years. Mean follow-up was 102.9±24.5 months. There were 12 eRALPs and 45 eLRPs in each group. Mean age and prostate-specific antigen level were similar in the two groups (P=.1 and P=.15, respectively; Table 2).
NA, not assessed; PSA, prostate-specific antigen.
There was no need for conversion in any case. Also, there were no complications during the intra- and postoperative periods. However, mean trocar replacement time was longer in Group 1 than in Group 2 (P<.001). Pathological Gleason score and prostate volume were comparable in the two groups. The results are summarized in Table 3. Moreover, there was no bleeding to be taken into account during trocar placements in the two groups.
Statistically significant P value.
EBL, estimated blood loss.
Additionally, there were eight (13.6%) iatrogenic peritoneal injuries during the preparation of the extraperitoneal space and trocar placement in Group 1 and five (8.7%) iatrogenic peritoneal injuries in Group 2 (P=.08). These did not affect the course of the operations.
Discussion
Trocar placement is an important step at the beginning of eLRP and eRALP. Thus, it may affect the continuum of the surgical procedure. In particular, if the patient has had previous abdominal surgeries with lower abdominal incision scars, this step may be challenging for the surgeons. Previous abdominal surgery has traditionally been considered as a relative contraindication to laparoscopy and has been found to increase the operative times and complication rates. 12 Controversially, there are published data on feasibility and safety of LRP13,14 and RALP 15 in patients with previous abdominal surgeries. To overcome these, herein we describe a practical and safe technique for creating the extraperitoneal space and for trocar placement in patients with lower abdominal scars. The trocar placement step is similar for eLRP and eRALP; thus we included and assessed their data together in this series. According to our best knowledge, this is the first study in which such a kind of technique was described for eLRP and eRALP in cases with previous major abdominal surgeries.
We used BMI and age for matched-pair analyses. These may have an effect on patients' body shape and thereby may affect directly the trocar placement step. 16 According to our study, operative and postoperative data were comparable between the two groups except the mean trocar placement time. Developing the extraperitoneal space during laparoscopic surgery is more difficult in patients with previous abdominopelvic surgeries. This step can be time-consuming and occasionally a hazardous procedure because previous abdominal surgeries usually lead to adhesions on the peritoneum and also fascias. 17 Therefore, access into the extraperitoneal cavity may be difficult. In our Group 1, with previous abdominal surgeries and lower abdominal scars, careful preperitoneal dissections by the fingers and the balloon on both sides were performed. Then, the median scars were dissected, and peritoneal adhesiolysis was necessary. Thus, the trocar placement time was longer in Group 1 than in Group 2. Additionally, the first three trocars were placed under digital guidance, and the last three trocars were placed under direct vision, after placement of the optic trocar. We took maximum care not to injure the peritoneum in order to keep the advantages of a close cavity operation. Moreover, flexibility of trocar sites is necessary when dealing with such kinds of difficult cases. 18 We have arranged our trocars according to our cases for providing maximum space without changing our main concept.
We described the safety of eLRP in patients with previous abdominal surgeries in our previous series. 10 In the present series, we aimed to exhibit the safety and feasibility of our trocar placement technique for eLRP and eRALP in patients with previous abdominal surgeries. Stolzenburg et al. 18 reported about the feasibility of eLRP in patients with previous abdominal surgeries. However, our series had similar results; additionally, we described a standard surgical technique. We have included both eLRP and eRALP cases in our study because creating the extraperitoneal space and trocar placement steps were the same in these procedures. Boylu et al. 19 presented their adhesiolysis technique with 18 RALP patients with previous abdominal surgeries in the transabdominal approach, and they noted that eLRP could be an alternative approach for these patients. Our results support their opinion; moreover, we do not need any bowel or omentum dissection according our extraperitoneal technique.
We performed standard open placement of the first trocar in eLRPs and eRALPs. 20 The balloon trocar was used for creating the extraperitoneal space, and optical vision was used for the initial access. Hajdinjak and Oakley 21 reported a similar technique as fast, easy, and safe in eLRP. On the other hand, Tinelli et al. 22 suggested that direct optical entry has some advantages when compared with open laparoscopy in terms of saving time, enabling a safe and expeditious, visually guided entry for laparoscopy. We have also preferred a balloon trocar dissection under optical vision successfully as a part of our technique. Nevertheless, using the dilating trocar may be superior to direct optical entry. There may be somewhat less bleeding and more space with the dilating trocar; thus rapid placements of trocars can be obtained. In addition, there may be desufflation of the extraperitoneal and/or peritoneal space, by using direct optical entry. However, it should be kept in the mind that the best way is the known and experienced way in trocar replacements. Therefore, these reported techniques above are just offered for trocar replacement during eLRP and eRALP.
Nazemi et al. 23 reported no difference in estimated blood loss and complication rate in their transperitoneal RALP series, when comparing those who had had previous abdominal surgery versus no surgery. Results of our study were parallel to theirs. The mean estimated blood loss during trocar placement was similar in both groups. We had also iatrogenic peritoneal injuries despite our careful dissection; however, these did not affect the course of the operations. We were able to establish trocar placement and correct access to the extraperitoneal space in all patients. In addition, all procedures could be completed without any complication and conversion. We believe that the extraperitoneal route of access with our technique contributed significantly to our findings in which previous abdominal surgery did not complicate the extraperitoneal approach.
There were some limitations in our study. First is the nonrandomized characteristic of the study. The second is the limited numbers of patients. These may be related with patient selection bias.
The main goals of the study are evaluating the safety and efficacy of trocar placement by our novel practical technique during eLRP and eRALP in patients with previous abdominal surgeries and lower abdominal incision scars. According to our best knowledge this has been the first series in the literature on this issue.
Conclusions
Creating the extraperitoneal space with our novel trocar placement technique can be performed safely and effectively in eLRP and eRALP patients with lower midline abdominal incision scars. Nevertheless, endoscopic surgeons should keep in mind that the best trocar placement technique should be selected by themselves.
Footnotes
Disclosure Statement
No competing financial interests exist.