
Abstract
Abstract
Objective:
To discuss the learning curve of laparoscopy-assisted distal gastrectomy (LADG) with lymph node dissection and the oncological results and long-term outcomes of different periods in the learning stage.
Patients and Methods:
One hundred twenty-four patients with gastric cancer who received LADG with lymph node dissection from January 2004 to December 2009 were retrospectively reviewed and analyzed. They were divided into three groups (A–C) according to different operative date: 41 were in Group A (early), 41 in Group B (middle), and 42 in Group C (laer). There were no significant statistical differences among the three groups with respect to age, gender, early/advanced gastric cancer, Union for International Cancer Control stage, and lymph node dissection. Then the following items were compared in these groups: operative time, blood loss, number of lymph nodes harvested, postoperative complications, postoperative hospital stay, and long-term survival.
Results:
The operative time in Group A (235.0±50.3 minutes) was significantly longer than in Groups B (201.7±39.6 minutes) and C (199.0±44.7 minutes), but there was no significant difference between Groups B and C. The harvest of lymph nodes from Group A (11.0±5.5) was significantly less than from Groups B (16.3±9.2) and C (17.2±8.7), but there was no significant difference between Groups B and C. The postoperative hospital stay and complications, overall survival, and disease-free survival showed no difference among the three groups.
Conclusions:
The learning curve of gastrointestinal surgeons with experience of laparoscopic operation is about 40 cases. The oncological principles and long-term outcomes were not sacrificed during the learning stage.
Introduction
L
However, compared with Japan and Korea, advanced gastric cancer (AGC), which requires a D2 lymph node (LN) dissection, makes up a larger proportion of the disease in China. Usually, laparoscopic surgery for AGC is technically more challenging because of extragastric lymphadenectomy, and the procedure's oncological adequacy and long-term outcome are still more concerning. Does the initial practice of laparoscopic surgery for gastric cancer, especially for AGC, impact the long-term outcomes? Some studies have reported the learning curve of laparoscopy-assisted distal gastrectomy (LADG) for gastric cancer, including advanced cases. Qian et al. 13 reported a learning curve of 50 cases, based on the data mainly from AGC. However, few studies concerned the oncological long-term outcomes of their initial experience during the learning curve period.
The aim of this study was to investigate the learning curve of LADG for those patients with gastric cancer, including advanced cases, who underwent an LADG procedure with D2 LN dissection, as well as the oncological long-term outcomes of LADG during the surgeon's learning stage.
Patients and Methods
This was an Institutional Review Board–approved retrospective study with data analysis on consecutive patients undergoing LADG for primary gastric adenocarcinomas in a single surgical unit. Medical records were collected on all adult patients (≥18 years old) with gastric cancer operated on between January 2004 and December 2009 from the prospectively maintained clinical gastric cancer database in the Shanghai Minimally Invasive Surgery Center, Shanghai Ruijin Hospital affiliated with the Shanghai Jiaotong University School of Medicine, Shanghai, China. Patients diagnosed with tumor pathology other than adenocarcinoma, patients with palliative operation, recurrent cases, or patients with inadequate data were excluded. Follow-up data were collected from review of medical and the annual outpatient follow-up records. Patients are annually contacted for a clinical and oncological follow-up, and an update of their medical status is reflected in their clinical charts.
Variables
Variables collected were as follows: demographic characteristics, Union for International Cancer Control (UICC) classification of tumor stage, location of the tumor, extent of LN dissection, procedure of reconstruction for gastrointestinal tract, operative time, estimated blood loss, conversion, and intraoperative complications. Pathologic results, postoperative outcomes including postoperative hospital stay, postoperative complications, and mortality, and long-term oncological outcomes were collected as well.
Before surgery, all patients had completed history and physical examinations, endoscopic assessment with biopsy, and preoperatively image examinations such as computerized tomography of the chest and abdomen. Both preoperative and postoperative Tumor-Node-Metastasis (TNM) stages were evaluated. For the patients with a postoperative pathologic result as stage II or greater lesions, adjuvant chemotherapy was routinely applied.
All the surgeries were performed by a systemic team of surgeons with abundant experience and expertise on conventional gastric surgery and laparoscopic skills. The operative time was defined as the time between when the operation started and finished, excluding the anesthesia time. The hospital stay was defined as the postoperative hospital stay. “Overall recurrence” included local recurrence, distant metastasis, and port-site metastasis. “Local recurrence” was defined as any recurrence of cancer that was located at the anastomotic line or abdominal cavity local to the primary lesion at any time after surgery and was proved by pathologic examination or imaging studies. “Distant metastasis” was defined as a metastatic carcinoma involving any distant organ secondary to the primary colon cancer, which was diagnosed by using imaging studies or biopsy.
Surgical technique
All patients were treated with radical gastrectomy and D1 or D2 LN dissection according to the TNM classification (6th) of gastric carcinoma by the UICC. All patients were placed in lithotomy position after general anesthesia. The surgeon stood on the patient's right, with the first assistant on the patient's left and the camera assistant between the patient's legs. LADG was performed using the reported previously methods of Kitano et al. 14 and Uyama et al. 15
Statistical analysis
All the data were analyzed with SPSS for Windows statistical software (version 11.0; SPSS, Inc., Chicago, IL). All the measurement data in this study were proven to be of normal distribution via the one-sample K test and were expressed by mean±standard deviation values. The one-way analysis of variance test was adopted in the analyses, and the least significant difference test was adopted in multiple comparison. All the enumeration data were expressed as percentages, and the chi-squared test was adopted. The disease-free survival and overall survival of the groups were calculated by the Kaplan–Meier method; the differences of the survival were compared with the log-rank test. All reported P values were two-sided: P values of <.05 were considered statistically significant, and P values of <.01 were considered to indicate obvious statistical significance.
Results
Between January 2004 and December 2009, in total, 144 consecutive patients had laparoscopic surgery for gastric cancer; 124 patients who underwent LADG were included in our study and divided into three groups (Group A, 41 cases; Group B, 41 cases; and Group C, 42 cases) according to the time (early, middle, or later) when they received the surgery.
Clinical outcomes
Demographic data, UICC classification of tumor stage, location of the tumor, extent of LN dissection, and procedure of reconstruction for gastrointestinal tract are described in Table 1. The distribution of tumor stage (AGC/EGC) and extent of LN dissection are shown in Figures 1 and 2, respectively.
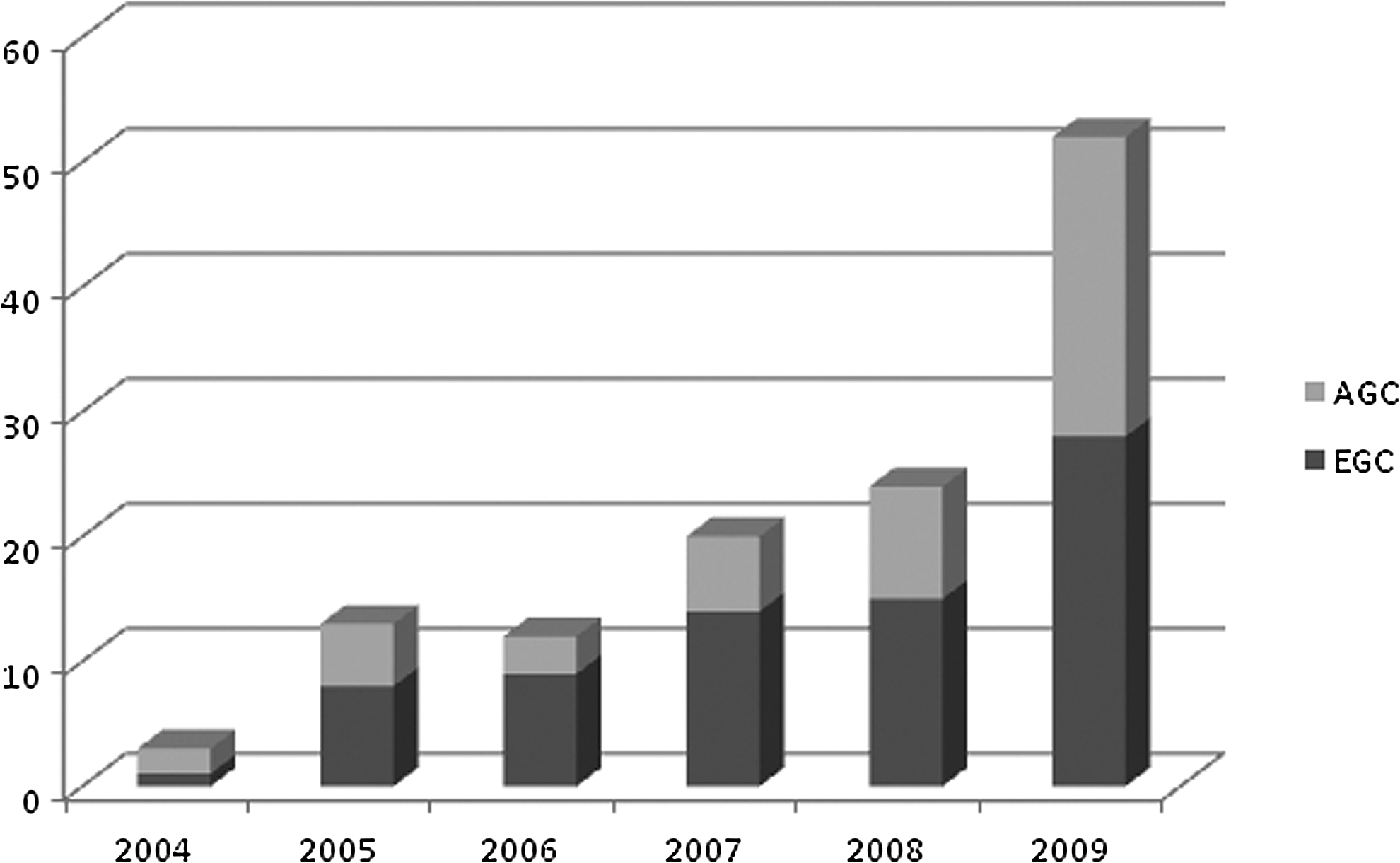
Distribution of tumor stage (advanced gastric cancer [AGC]/early gastric cancer [EGC]) among 124 cases.
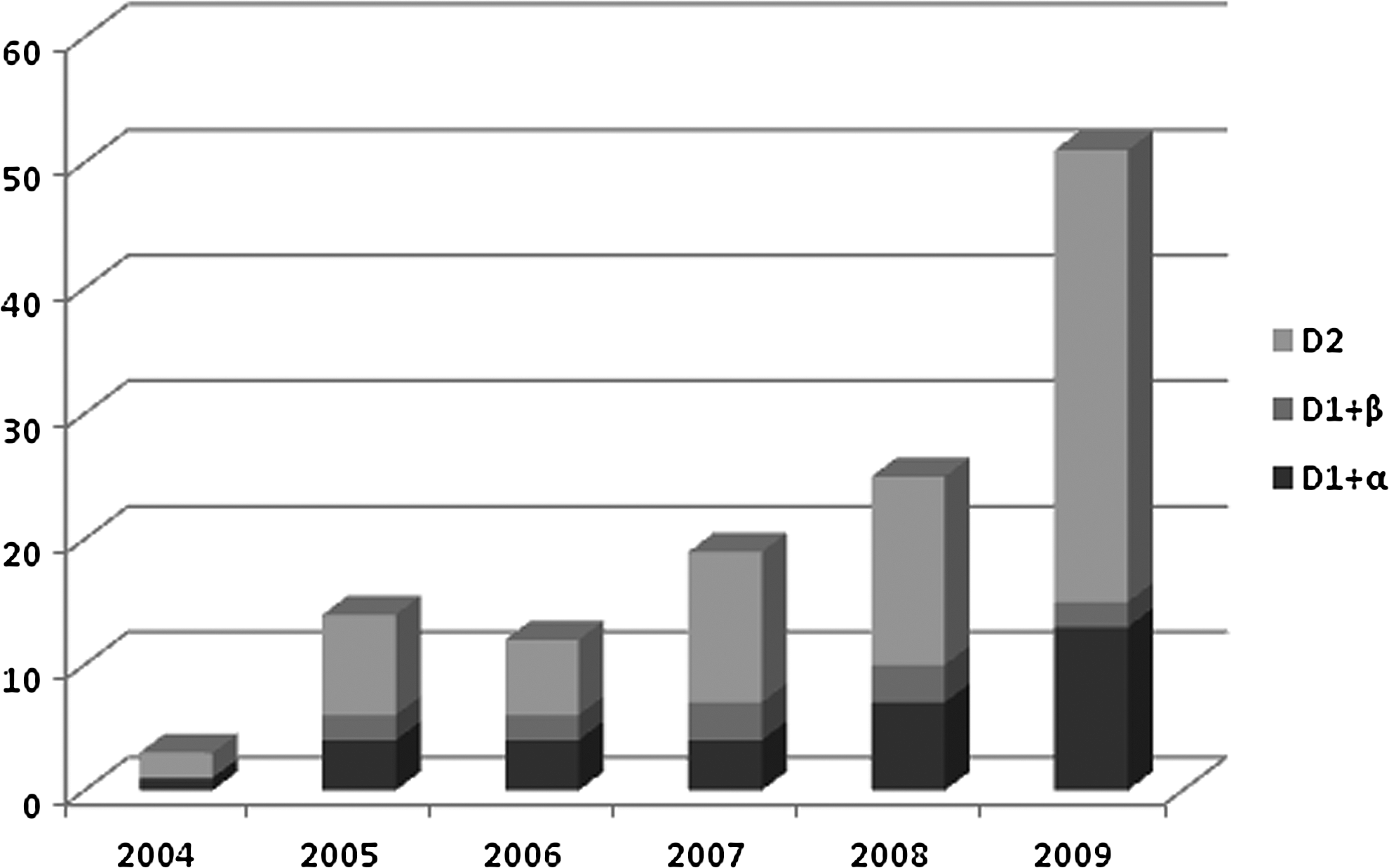
Distribution of lymph node dissection by laparoscopy-assisted distal gastrectomy among 124 cases.
UICC, Union for International Cancer Control; L, lower third; M, middle third.
Surgery-related results
The operative time in Group A was 235.0±50.3 minutes, which was significantly longer than that in Groups B (201.7±39.6 minutes) and C (199.0±44.7 minutes) (PA-B<.01, PA-C<.01), whereas the difference between Groups B and C was not significant (P=.991). The estimated blood loss in Group A was 197.8±173.1 mL, which was more than that in Groups B (183.9±188.8 mL) and C (163.6±215.8 mL), but the difference was not significant. The LN harvest in Group A (11.0±5.5) was significantly less when compared with Groups B (16.3±9.2) or C (17.2±8.7) (PA-B<.01, PA-C<0.01), but the difference between Groups B and C was not significant (P=.945). Postoperative hospital stay and postoperative complications among these three groups were comparable (Table 2).
Subgroup comparisons were analyzed separately for operative time and lymph node (LN) harvest.
EBL, estimated blood loss.
Long-term outcomes
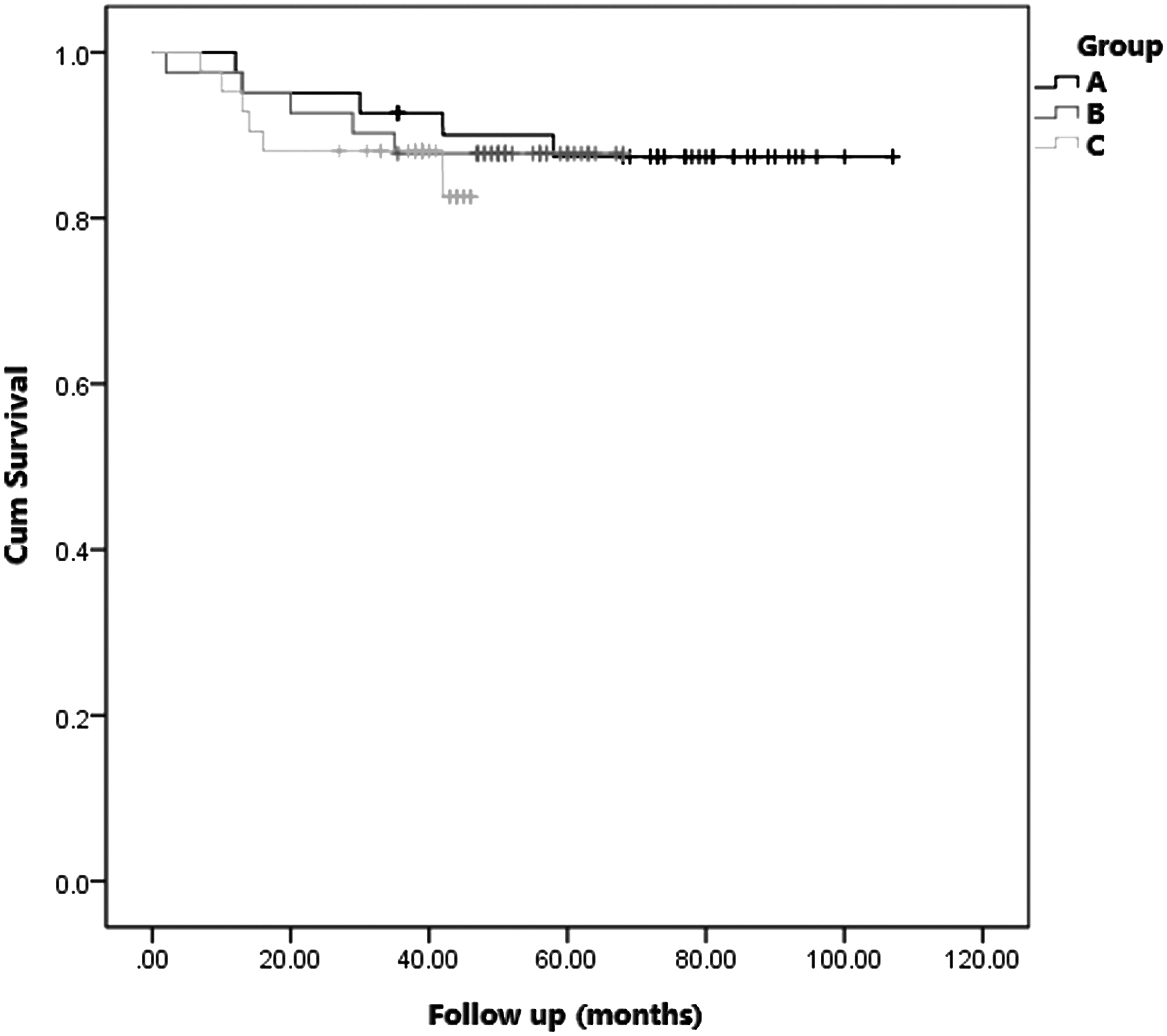
The mean follow-up time was 49.5 (range, 2–107) months. Fifteen deaths were observed in our study during the follow-up interval (more than 30 days after surgery). Fourteen of these patients died from primary gastric cancer-related diseases (local recurrence and/or metastasis). One case died because of heart disease. During the follow-up period, recurrence (local recurrence or distant metastasis) was observed in 16 cases. Overall survival was 86.6% in all cases, and disease-free survival was 85.4%. Overall survival for Groups A, B, and C was 89.8%, 87.7%, and 85.4%, respectively, and no significant difference was observed among these three groups (P=.4960 (Fig. 3). Disease-free survival for Groups A, B and C was 87.4%, 87.8%, and 82.6%, respectively, with no significant difference (P=.736) (Fig. 4).

Overall survival of the three groups. Overall survival for Groups A, B, and C was 89.8%, 87.7%, and 85.4%, respectively, and no significant difference was observed among these three groups (P=.496). Cum, cumulative.
Disease-free survival of the three groups. Disease-free survival for Groups A, B, and C was 87.4%, 87.8%, and 82.6%, respectively, with no significant difference (P=.736). Cum, cumulative.
Discussion
The operation results of 124 consecutive patients who underwent LADG were analyzed in our study. The time for performance of the operation was significantly different between Groups A and B and between Groups A and C, but not between Groups B and C, which means that the operation skill reaches a mature and stable level after the first 41 operations. The same phenomenon also shown in the factor of LN dissection number: surgeons executed more effective LN dissection after the first 41 operations. Although there was no difference among the three groups in blood loss during operation and in peri- and postoperative complications, the absolute value presented a tendency to decline from Group A to Group C. Therefore, the learning curve of LADG could be inferred as 40 operations in our study.
This result showed a shorter learning curve than that found by Kunisaki et al., 10 Kim et al., 11 or Qian et al. 13 The fact that in this study all the surgeries were performed by surgeons with abundant experience in conventional gastric surgery and laparoscopic colorectal resection could be the possible explanation. More skills are required to perform a laparoscopic surgery than a conventional one. Usually, the learning curve of a new technique depends on the clinical experience and operation skills of a surgeon. As reported by Yoshikawa et al., 16 the learning curve of LAG has a relationship with abundant experience with conventional gastric surgery and laparoscopic manipulation. Usually, laparoscopic cholecystectomy is considered as an indispensable learning procedure before the practice of LAG. According to the conclusion of Li et al., 17 surgeons without experience in laparoscopic cholecystectomy can improve their laparoscopy skills by other means, for example, virtual exercises, animal experiments, and observations of operation. Beginning with some simple operations (e.g., appendectomy, bowel exploration, repair of gastric perforation, and gastrointestinal benign tumor resection) by laparoscopy is another shortcut to accumulate experience of laparoscopic manipulation in order to shorten the learning curve of LAG.
Laparoscopic surgery relies on the coordination between surgeon and assistants. The cameraman is the “eyes” of the surgeon, whereas the first assistant is the “extra hands” of the surgeon. A good teamwork of surgeon, assistant, and cameraman can widely diminish the learning curve. Thus, a fixed LAG team has to be built to cultivate teamwork and tacit understanding during the surgery. In another hand, the application of advanced instruments (e.g., Harmonic® [Ethicon Endo-Surgery, Cincinnati, OH] scalpel, LigaSure™ [Covidien, Boulder, CO], etc.) helps simplify the mobilization and maintain hemostasis. The high-definition laparoscopy provides clear images of the surgical area, ensuring the learning effects of laparoscopic surgery.
In choosing patients for beginners of LAG, we place great emphasis on body mass index, total condition, and preoperation grade of patients. The security of the surgery procedure and the radical resection of a malignant tumor is the first procedure of LAG. In this study, 75 LADG procedures were accomplished for EGC, whereas 49 involved AGC. The majority of these cases (79 cases) involved D2 LN dissection, whereas D1+α LN dissection and D1+β LN dissection were 33 cases and 12 cases, respectively. The ideal patients for beginners in LAG were characterized as young, thin, having an early grade of tumor, and with a tumor located in the lower segment of the stomach. From EGC to AGC, from LADG to laparoscopy-assisted proximal gastrectomy and laparoscopy-assisted total gastrectomy, and from D1+α LN dissection and D1+β LN dissection to D2 LN dissection is a pathway we proposed to jumpstart the learning curve of LAG.
The long-term outcome is always one of the most important issues to be concerned in curative surgery for malignancy. With several advantages confirmed in short-term outcomes of laparoscopic surgery for gastric cancer,18,19 the long-term outcome currently becomes the focus in this field.6,20,21 In our study, both the overall survival and the disease-free survival were comparable in these three groups. Whether in the initial period or in the later period, all procedures were performed following oncological principles, which include en bloc resection, nontouch technique, proximal lymphovascular ligation, adequacy of resected margins, and complete lymphadenectomy. The oncological principles were never sacrificed to achieve “laparoscopic surgery” even in initial cases (Group A). So in our opinion, the learning curve only has an impact on technical parameters such as operation time, but not on quality control of the surgery, such as the oncological principles.
In conclusion, the learning curve of LADG for gastrointestinal surgeons with experience in laparoscopic operation is about 40 cases. Oncological principles and long-term outcomes were not sacrificed during the learning stage. The main impact factors of the learning curve are the experience of the operators, teamwork, and selection of the patients.
Footnotes
Disclosure Statement
No competing financial interests exist.