
Abstract
Abstract
Background:
In recent years, single-incision laparoscopic appendectomy has been used as an improved form of conventional laparoscopic appendectomy (CLA). We have started to perform gasless laparoscopy-assisted transumbilical appendectomy (GLATUA) in patients with uncomplicated appendicitis. This study aimed to evaluate the feasibility, safety, cosmetic results, and cost-effectiveness of this novel technique of GLATUA.
Patients and Methods:
In total, 30 patients with a diagnosis of acute appendicitis without evidence of periappendiceal abcess or perforation and indicated for operation were enrolled in the study. Attempts to operate by the GLATUA technique initially were made in all of the patients. When it was technically difficult to perform appendix extraction via the umbilicus, the procedures were converted to the CLA technique (conversion group). The following factors between the successful group and conversion group were investigated to evaluate feasibility and predictable factors for the success of GLATUA: age, gender, duration from symptom onset to hospital visit, preoperative ileus, preoperative white blood cell count, neutrophil count (%), body mass index, fat infiltration in abdominal computed tomography or ultrasonography, pathologic characteristics of the resected appendix, and postoperative complications.
Results:
Among the 30 patients, 19 patients underwent operation by the GLATUA technique (63.3%). There were no significant differences between the two groups in terms of demographics, duration from symptom onset to hospital visit, preoperative white blood cell count, neutrophil count (%), and pathologic characteristics of the appendix. Significant differences were observed between the two groups for preoperative ileus in simple abdominal x-ray and fat infiltration in preoperative diagnostic modality. There were no postoperative complications in both groups.
Conclusions:
GLATUA is a feasible, safe, and cost-effective technique for appendectomy in uncomplicated appendicitis and shows good cosmetic results. It did not increase the rate of complications and represents a possible alternative to the CLA technique in cases without fat infiltration in abdominal tomography or ultrasonography and small bowel ileus in simple abdominal x-ray.
Introduction
A
The purpose of the current study therefore was to test for the feasibility, safety, and possible advantages of GLATUA, using a single umbilical incision and laparoscopic instruments without a trocar with pneumoperitoneum for the resection of the appendix as a technique with the purpose of reducing the cost of laparoscopy while preserving all the benefits of the laparoscopic approach.
Patients and Methods
Between June 2012 and September 2013, 30 patients underwent the GLATUA technique initially by a single surgeon, at Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. All patients were informed about the operative technique and provided written informed consent. All patients in our study underwent an abdominal computed tomography (CT) or ultrasound to confirm the diagnosis of appendicitis and to rule out complicated forms of appendicitis, such as periappendiceal abscess or perforation. Individuals with complicated appendicitis on CT or ultrasound scan were excluded from the study. Preoperative and histopathological parameters were recorded. Data involving patients' demographics, operative time, duration from symptom onset to hospital visit, preoperative ileus, preoperative white blood cell count, neutrophil count (%), patients' body mass index (BMI), fat infiltration in diagnostic modality (abdominal CT or ultrasonography), diameter and length of the appendix, pathology of the resected appendix, appendicolith, and postoperative complications. Preoperative and postoperative antibiotics were administered intravenously with second-generation cephalosporin for 72 hours. All the patients had follow-up visits at postoperative weeks 1 and 2 to check for complications.
Statistical analysis
Statistical analysis of data was performed with SPSS version 19.0 software (SPSS Inc., Chicago, IL). Continuous data were expressed as mean and standard deviation values. All data were analyzed using the chi-squared test, independent t test, Mann–Whitney U test, and multivariate logistic regression test for calculation of significance. A P value of <.05 was considered statistically significant.
Surgical technique of GLATUA
With the patient under endotracheal intubated general anesthesia, we made a 10–15-mm longitudinal umbilical incision with or without a wound retractor. The right lower quadrant abdominal wall was then lifted with a thin surgical retractor (Senn retractor or Obwegeser retractor) to provide a working space in the abdominal cavity without the pneumoperitoneum. We inserted a 0° 5-mm laparoscope and a 5-mm laparoscopic Babcock forceps through the umbilical incision (Fig. 1). When the appendix was identified under laparoscopy, the tip of the appendix or mesoappendix was grasped and drawn out through the umbilical incision (Fig. 2). The mesoappendix was divided between the ligatures, the base of the appendix was ligated, and the mucosa of the appendix was cauterized. The appendiceal stump was then returned to the abdominal cavity. Finally, we removed the inflammatory peritoneal fluid in the pelvic cavity and right paracolic gutter through the suction tip and closed the wound cosmetically (Fig. 3). We used povidone-iodine soaking gauze instead of a wound protector for protection during the operation, and we placed a povidone-iodine soaking cotton ball on the umbilical wound for 24 hours after the operation. We converted to the CLA technique if the appendix or mesoappendix could not be extracted because of immobility of the appendix.
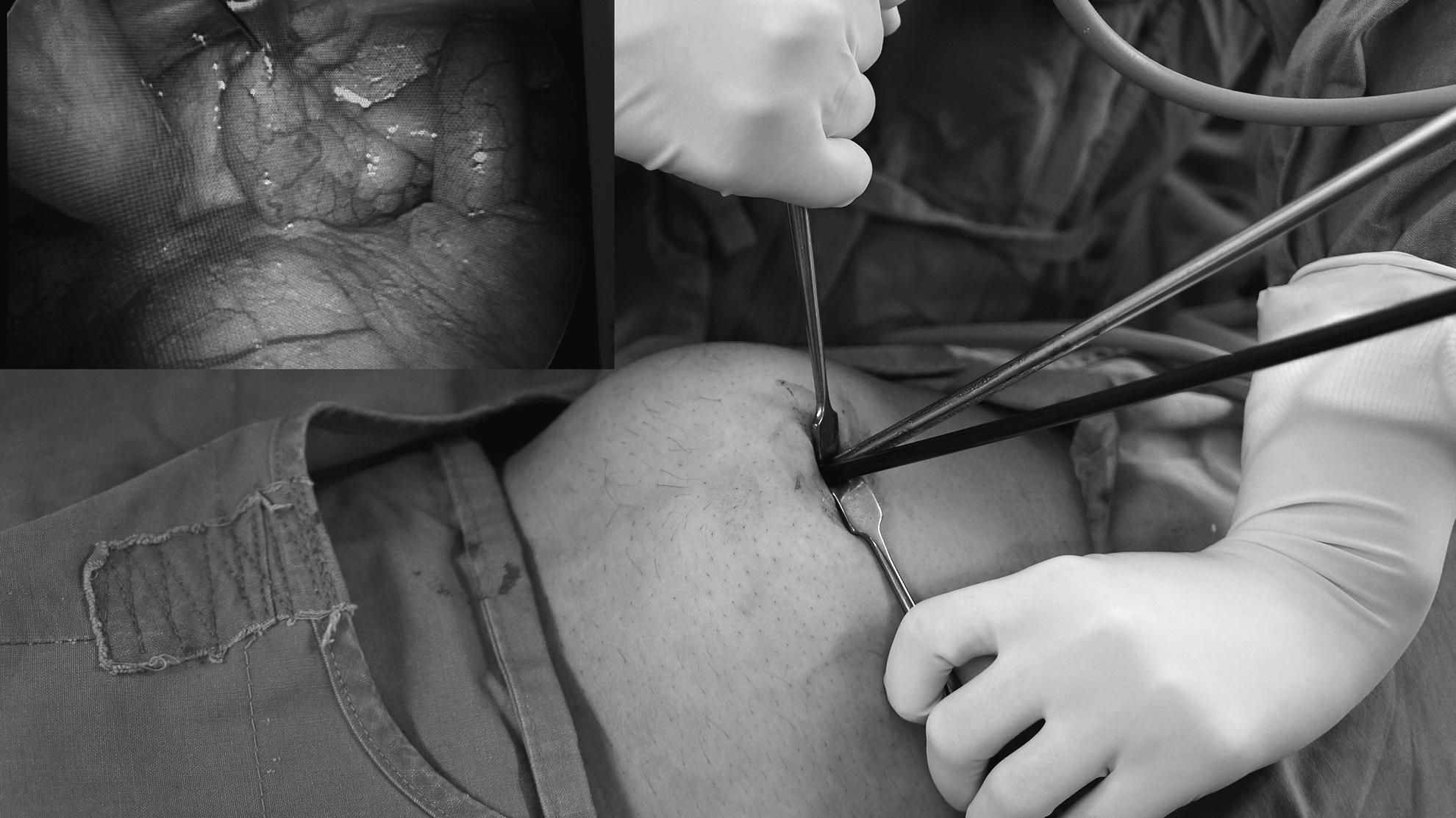
A longitudinal umbilical skin incision (1–1.5 cm long) was made. Under upward retraction of the abdominal wall with a Senn or Obwegeser retractor, the 5-mm laparoscope and endo-Babcock forceps were inserted.

Extracorporeal view of extracted appendix through the umbilical incision.

The sutured wound showed a highly favorable cosmetic effect after the gasless laparoscopy-assisted transumbilical appendectomy operation.
Surgical technique of CLA
CLA was performed using three trocars: umbilical (5-mm trocar), left lower quadrant (10-mm trocar), and suprapubic (5-mm trocar). Endoloops and endoclips were used through the left lower quadrant port to ligate and divide the appendix and mesoappendix. The appendix was removed through the left lower quadrant port with an endopouch. Once the operation was finished, the gas remaining in the abdominal cavity was extracted through the trocar sheath.
Results
From June 2012 until September 2013, 30 patients were admitted to our surgical ward with a diagnosis of uncomplicated appendicitis through preoperative abdominal CT or ultrasonography. The demographic characteristics of the success group and conversion group are summarized in Table 1. Among 30 patients, 19 patients received the GLATUA technique successfully (63.3%) (successful group), whereas 11 patients had to be converted to the CLA technique (36.7%) (conversion group). No drain was inserted in both groups. There was no statistical difference in age, gender, or BMI. The operative time (from incision to placement of the last skin suture) was 44.1±11 (range, 30–70) minutes in the successful group. There were no significant differences in duration from symptom onset to hospital visit, preoperative white blood cell count, or neutrophil count (%) between the two groups, but significant statistical differences were observed for small bowel ileus in preoperative simple abdominal x-ray and fat infiltration in the preoperative diagnostic study in univariate analysis (P=.007 and .005, respectively) (Table 2). In multivariate analysis, preoperative small bowel ileus (odds ratio=11.41; P=.012) and fat infiltration in the preoperative diagnostic study (odds ratio=8.93; P=.015) were found to be the prediction factors for conversion to the CLA technique (Table 3). The pathological characteristics of the appendix were not significantly different between the two groups (Table 4). There were no postoperative complications such as wound complications, wound hematoma, intestinal obstruction, and intraabdominal abscess in both groups.
BMI, body mass index; SD, standard deviation.
CLA, conventional laparoscopic appendectomy; CT, computed tomography; GLATUA, gasless laparoscopy-assisted transumbilical appendectomy; SD, standard deviation; WBC, white blood cell.
CI, confidence interval; CT, computed tomography.
CLA, conventional laparoscopic appendectomy; GLATUA, gasless laparoscopy-assisted transumbilical appendectomy SD, standard deviation.
Discussion
CLA is a widely accepted treatment for acute appendicitis. 6 In recent years, the search for greater patient comfort and better cosmetic outcome due to scarless procedures, such as NOTES and single-incision laparoscopic surgery, has led surgeons to newer means of access to the abdominal cavity with less surgical trauma. However, single-incision laparoscopic surgery using specifically designed trocars or instruments has increased the costs significantly.
The TULAA technique was first proposed by Pelosi and Pelosi, 3 but TULAA is not a routinely accepted technique for appendicitis in adults because of the difficulty in extracting the appendix through the umbilicus in adult patients, However, the distance from the umbilicus to the ileocecum is quite small, and the abdominal wall is flexible in pediatric patients, which has led surgeons to limit TULAA to children. 7 We modified the TULAA technique to GLATUA and extended the indication to adult patients without complicated appendicitis and evaluated the feasibility and safety of GLATUA. As seen in our study, the GLATUA technique is feasible and safe, and there is no greater incidence of complications compared with the CLA technique. Furthermore, it was also performed successfully on adult patients. The GLATUA technique might require a shorter operating time than the CLA technique because GLATUA enables quicker extracorporeal dissection and resection.8,9 However, in the current study, we could not analyze the operation time between the GLATUA technique and the CLA technique because the CLA technique had difficulties in exteriorizing the appendix through the umbilicus after the initial trial of the GLATUA technique. The GLATUA technique is a gasless laparoscopic procedure that protects the patient from pneumoperitoneum-associated complications such as hypercarbia, acidosis, gas embolism, subcutaneous emphysema, deep venous thrombosis, instability of hemodynamics, decrease in renal function, and peritoneal oxidative stress.10,11 One of the advantages of GLATUA is the absence of trocar-related complications.
The most significant difference between GLATUA and CLA is the cost. In spite of reported decrease in cost of laparoscopic instruments and supplies (trocar, endoloop, endoclips, and endostaplers) over time, laparoscopic operative procedures are still more expensive than open surgery. In GLATUA, the cost of the operative procedure equals that of open appendectomy, and the operative cost surplus of laparoscopy is eliminated; we did not use the three trocars, three endoloops, endopouch, and endoclips that are used in the CLA technique, so we could reduce the cost by a mean of $356 in U.S dollars. At the same time, the GLATUA technique provides all the clinical benefits and secondary savings associated with laparoscopy such as decreased hospital stay and earlier resumption of normal activities. For this reason, GLATUA could be an alternative and cost-effective minimally invasive technique for uncomplicated appendicitis.
Most of the patients in our study had normal BMI, and we did not intentionally exclude obese patients; however, we observed no relationship between BMI and the conversion rate. According to our GLATUA experiences, it is presumed that the insufficient working space due to difficulty in retraction of the fatty abdominal wall and the abdominal fat, including the omentum, might provide disturbances in identification of the appendix, extraction of the appendix through the umbilical wound, and extracorporeal appendectomy. The potential problem of the GLATUA technique is that the inflamed appendix is brought directly through the umbilical wound, increasing the chance of wound infection.12,13 However, in our study, umbilical wound infection did not occur. Umbilical wound infection can be prevented by using a small wound protector. In the present study, we did not use a wound protector except in the first 2 cases because of the difficulty in inserting and pulling the umbilical protector out the small-sized umbilical wound (10–15 mm). It is presumed that there was no perforated appendicitis in our study, and umbilical infection can be controlled if adequate skin gauze protection is secured around the umbilical opening when bringing the appendix out. Another aspect related to wound-related complications is asymptomatic periumbilical wound hematoma due to the involuntary trauma caused by the surgeon when making a forced movement in a limited workspace. 6
Another limitation of the GLATUA technique is difficulty in exploration of abdominal structures. This is due to the limitation of mobilizing abdominal contents with a single instrument, a 0° laparoscope, and insufficient working space without gas insufflation. To improve this problem, it is necessary to design a specialized retractor with a long rigid blade for more sufficient working space and to minimize the necessity of abdominal exploration by performing a careful physical examination and imaging study. Conversion to the CLA technique was required in 11 patients because of an immobility of the appendix through the umbilical wound due to the presence of severe inflammatory adhesion between the appendix and periappendiceal structures, such as the cecum, terminal ileum, and retroperitoneum. All of the patients in the conversion group had small bowel ileus and/or fat infiltration in their preoperative radiologic studies. In univariate and multivariate statistical analyses, the small bowel ileus and the fat infiltrations were significantly greater in the converted cases than in the successful cases. We presume that in less severe inflammation cases, the success rate of GLATUA might be higher. Some limitations of the current study exist. These include the small sample size and no long-term follow-up after the operation. To standardize the GLATUA technique, case accumulation and long-term follow-up are needed.
Conclusions
According to our experience, the GLATUA technique is a feasible, safe, esthetic, and cost-effective procedure for uncomplicated appendicitis. Conversion to the CLA technique could be possible in any case when optimal conditions are not present. We therefore recommend its initial use in uncomplicated appendicitis patients.
Footnotes
Disclosure Statement
No competing financial interests exist.