
Abstract
Abstract
Background:
Experimental knowledge about mesh behavior at the esophageal hiatus is rare, but such information is essential in order to find a safe and effective method of mesh reinforcement. This study aimed to investigate the influence of mesh structure on the biological behavior of polypropylene prostheses placed at the hiatus.
Materials and Methods:
Twenty-four pigs in three groups of eight underwent implantation of heavyweight small-porous (HW-SP), heavyweight large-porous (HW-LP), or lightweight large-porous (LW-LP) circular polypropylene mesh at the hiatus. Eight weeks later, the meshes were explanted. Macroscopic analysis was performed evaluating mesh deformation, adhesions, and position relative to the hiatal margin. Histological analysis comprised evaluation of foreign body reaction and tissue integration by mononuclear cell count and immunostaining of Ki-67, collagen type I, and collagen type III.
Results:
No mesh-related complications occurred. Mesh shrinkage was observed within all groups and was the lowest for HW-LP, higher for HW-SP, and highest for LW-LP (13.8% versus 19.5% versus 25.5%; P<.001). The adhesion score was highest for HW-SP, lower for HW-LP, and lowest for LW-LP (11.0 versus 8.0 versus 6.0; P<.001). The collagen type I/III ratio was higher for HW-SP compared with HW-LP and LW-LP (3.1 versus 2.2 versus 1.8; P=.014).
Conclusions:
Heavyweight polypropylene meshes may be advantageous for application at the hiatus. They provide a solid fixation of the esophagogastric junction by adhesions, which may contribute to a reduction of hernia recurrence. In heavyweight meshes, the large-porous structure is associated with superior form stability, and small-porous meshes are superior with regard to solidity of tissue integration, which may prevent mesh migration.
Introduction
L
Only a few experimental studies have investigated the biological behavior of mesh prostheses if placed at the esophageal hiatus.8–12 Surgical meshes are commonly based on polypropylene, polyester, or polytetrafluororethylene. Besides polymer material, mesh types are categorized by their underlying structural specifications, such as weight, filament structure, thickness, and pore size. As demonstrated by the lightweight and large-porous concept for ventral hernia repair, weight and pore size in particular have a distinct influence on the biological behavior of mesh prostheses. 13 In a previous experiment we evaluated the behavior of circular heavyweight small-porous (HW-SP) polypropylene meshes at the hiatus, which was characterized by intense adhesion formation fixing the esophagogastric junction and a stable position around the esophagus without a tendency toward stenosis, migration, or erosion. 8
However, to date, there is no experimental knowledge about the influence of structural specifications on the biological behavior of meshes placed at the hiatus. This experimental study aimed to evaluate polypropylene meshes of different weight and pore size placed circularly at the hiatus and to answer to the question whether there is a structural configuration that can be regarded as advantageous for hiatal mesh reinforcement.
Materials and Methods
Study design
This experimental study was performed in an animal model. Twenty-four 8-week-old Landrace pigs were divided into three experimental groups of eight animals each. Each experimental group was assigned to one of the polypropylene mesh types used within this study (Table 1). An HW-SP and a heavyweight large-porous (HW-LP) mesh of similar weight were chosen to evaluate the influence of pore size on mesh behavior at the hiatus. In addition, a lightweight large-porous (LW-LP) mesh was used to assess the influence of mesh weight on mesh behavior at the hiatus. The meshes were placed circumferentially around the hiatus and fixed with fibrin glue (Beriplast®; Nycomed, Konstanz, Germany). After 8 weeks the animals were sacrificed, and meshes were explanted. Macroscopic analysis comprised evaluation of mesh deformation, adhesion formation, and tendency toward mesh-related complications. Histological analysis was performed in order to assess foreign body reaction and tissue integration.
All meshes are based on polypropylene.
All were from Covidien (Neustadt, Germany).
HW-LP, heavyweight large-porous; HW-SP, heavyweight small-porous; LW-LP, lightweight large-porous.
Animal care and anesthesia
The experiments were performed in accordance with the German Law for Animal Protection and were authorized by the local Committee on Animal Care of the Government of Karlsruhe, Germany. Before surgical procedures, all animals were denied food for 12 hours with free access to water. Premedication was performed intramuscularly with 10 mg/kg ketamine (Ketanest®; Roche, Grenzach-Wyhlen, Germany) plus 4 mg/kg azaperone (Stresnil®; Janssen, Neuss, Germany) and 0.5 mg/kg midazolam (Dormicum®; Roche). General anesthesia was induced via intravenous injection of 10 mg/kg ketamine (Ketanest) and 0.5 mg/kg midazolam (Dormicum) and sustained by using 2% isoflurane (Attane™ isoflurane for veterinary use; Provet, Lyssach, Switzerland) in an oxygen (1:1) mixture through an endotracheal tube on a closed circuit with mechanical ventilation. In addition, all animals received an intravenous injection of 0.5 mg/kg piritramide (Dipidolor®; Janssen) for analgesia. Prior to implantation surgery, the animals received a depot antibiotic via an intramuscular single-shot application of 10 mg/kg procaine penicillin and 16 mg/kg dihydrosteptomycin (penicillin–dihydrostreptomycin for veterinary use; Animedica GmbH, Frankfurt, Germany). The animals received food and water ad libitum immediately after surgery. Every 12 hours, the animals received a postoperative analgetic treatment for 5 days via intramuscular injection of 50 mg/kg metamizol (Novalgin®; Aventis Pharma, Frankfurt) and 4 mg/kg carprofen (Rimadyl®; Pfizer GmbH, Karlsruhe). All animals were sacrificed during explantation surgery by central venous injection of potassium chloride (2 mmol/kg).
Operative procedure
All surgical procedures were performed by the same team. Mesh implantation surgery was done under sterile conditions as described before. 8 In brief, after upper abdominal midline incision, a dorsal hiatoplasty was performed using two sutures (Ethibond 2/0 SH; Ethicon, Norderstedt, Germany). A standardized sterile template was used to cut out a circular 55-×55-mm mesh with a 16.5-mm eccentric hole from a mesh type corresponding to the experimental group (Fig. 1). The mesh was placed around the esophagus and centered at the hiatus while maintaining circumferential contact with the esophagus. After a plane mesh position on the diaphragm was affirmed, the mesh was fixed with fibrin glue (Beriplast).
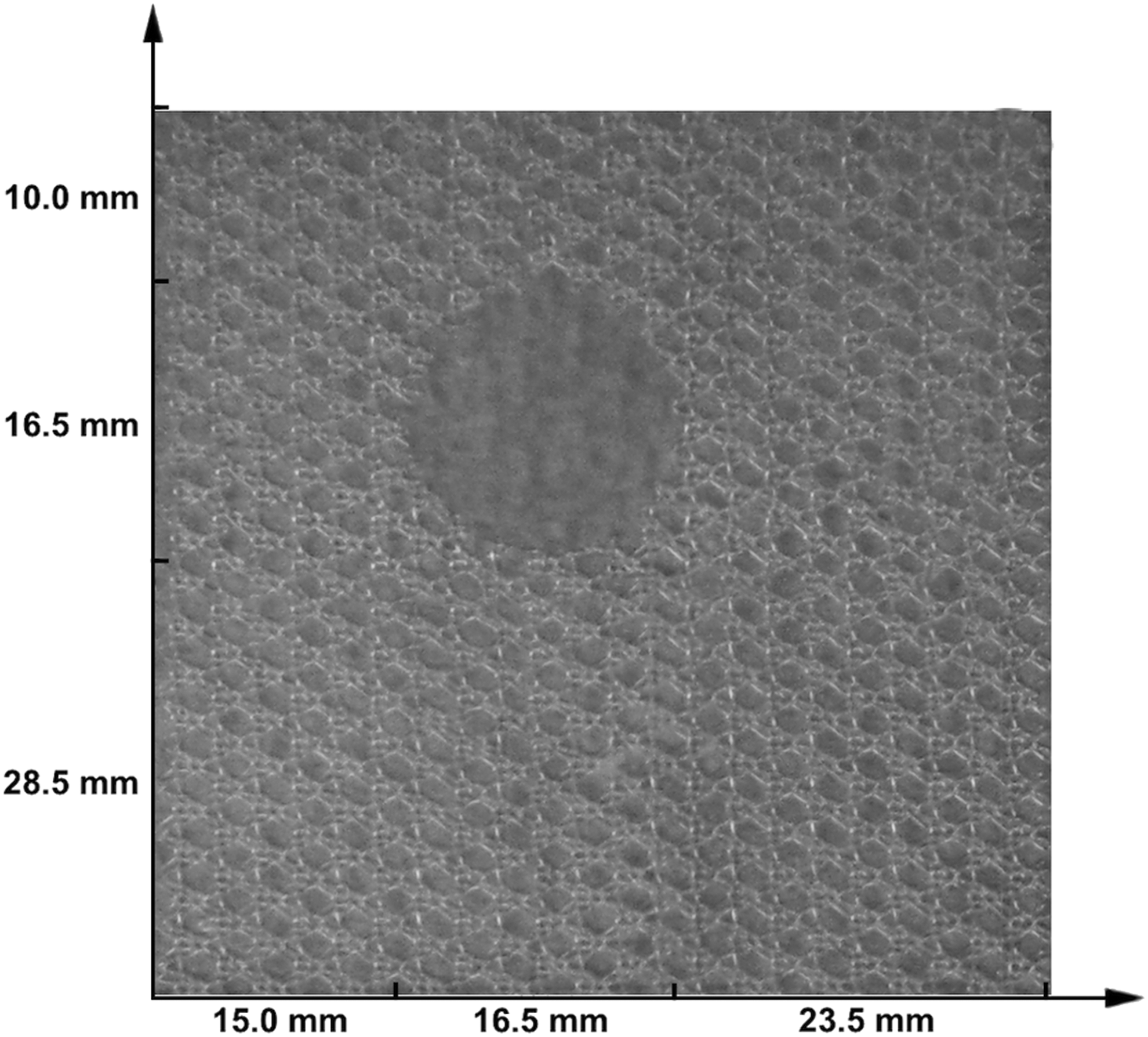
Mesh dimensions at implantation.
Mesh explantation surgery was performed 8 weeks after implantation. The hiatal region was re-approached via an upper midline incision and cautious adhesiolysis. After complete exposure, a specimen including the mesh, the central part of the diaphragm, the esophagogastric junction, and the tissue adherent to the mesh was explanted.
Macroscopic analysis
Evaluation of mesh deformation
In order to obtain accurate mesh dimensions, the meshes were photographed next to a measuring tape for size calibration before implantation and after explantation. A tripod was used to fix the camera in a standardized position 30 cm above the mesh. The camera's optical axis was aligned perpendicular to the working surface by the use of a common water level. We used the segmentation software Medical Imaging Interaction Toolkit 14 to determine size of the mesh and its aperture at all three measurements.
Evaluation of adhesions
During explantation surgery the number and kind of organs involved in adhesions to the mesh were determined. Furthermore, the percentage of mesh area covered by the adhesions was evaluated by two independent investigators. A published adhesion score was used in order to assess the degree of the adhesion formation (Table 2). 15 Additionally, mesh adhesions involving the cardia and the esophagus were quantified by the use of a score in order to evaluate the intraabdominal fixation of the esophagogastric junction to the mesh (Table 3).
Evaluation of mesh migration and esophageal erosion
Two independent investigators inspected the esophagus and all adherent organs for erosion using a magnifying glass. The position of the inner edge of the mesh relative to the border of the diaphragmatic hiatus was measured at the 3, 6, 9, and 12 o'clock positions. A protrusion of the mesh beyond the border of the hiatus was assigned a negative value in millimeters, whereas mesh retraction corresponded to a positive value in millimeters. At least one negative value was postulated for relevant mesh migration. 8
Histological analysis
Specimen extraction and fixation
After explantation, samples of mesh and adherent tissue were immediately stored in 4% formaldehyde and embedded in paraffin. Serial sections 3–5 μm thick were stained with hematoxylin and eosin for morphologic analysis and evaluation of mononuclear infiltrate. Six 2-μm sections were cut from each sample for immunoenzyme staining.
Immunoenzyme staining
Ki-67, collagen type I, and collagen type III stainings were performed using the following antibodies: monoclonal mouse anti-human Ki-67, 1:1000 dilution (clone MIB-1; IgG1; Dako Deutschland GmbH, Hamburg, Germany); polyclonal rabbit anti-human collagen type I, 1:50 dilution (IgG; Biotrend Chemikalien GmbH, Cologne, Germany); and polyclonal rabbit anti-human collagen type III, 1:25 dilution (IgG; Biotrend Chemikalien GmbH). Isotype- and concentration-matched control antibodies (Dako) were used for negative controls. For antigen retrieval, slides were incubated in a pressure cooker for 5 minutes in citrate buffer, pH 6.1. Standard avidin–biotin complex and anti–horseradish peroxidase (Vectorlabs, Burlingame, CA) were applied according to the manufacturer's instructions. The primary antibody was added overnight at 4°C. Donkey anti-mouse or donkey anti-rabbit biotinylated antibodies 1:100 dilution (Dako) were used as secondary reagents (30 minutes at room temperature). 3,3′-Diaminobenzidine (Vectorlabs) was used as the substrate for horseradish peroxidase. Slides were counterstained with hematoxylin and then mounted.
Microscopic evaluation
Microscopic evaluation was performed on six different serial sections of each mesh by an independent expert pathologist who was unaware of the treatment groups. Processed slides were scanned for image acquisition using the Aperio (Vista, CA) Scanscope® CS and analyzed with the Aperio ImageScope software. Mononuclear infiltrate was counted within a distance of 300 μm from the mesh fibers. Within each serial section, 500 cells were counted for evaluation of percentage positivity for Ki-67. Tissue integration was evaluated by determining partial volume of collagen type I and collagen type III using the ScanScope software color deconvolution algorithm.
Statistical analysis
Statistical analysis was performed using SPSS version 19.0 software (SPSS, Chicago, IL). Values of P<.05 were considered significant. The results were analyzed for statistical significance using the analysis of variance according to the Kruskal–Wallis test. In case of significance, a Mann–Whitney U test was performed for the paired comparison of two experimental groups. For the comparison of dependent samples, the Wilcoxon signed-rank test was used. Rank correlation according to Spearman was used for testing correlation. Results are expressed as median (interquartile range).
Results
All surgical procedures were performed without any complication. Among the three experimental groups, no significant differences were found for weight and operating time. At explantation, the animals within all experimental groups showed significant weight gain (Table 4).
Data are median values (interquartile range).
By Kruskal–Wallis test.
HW-LP, heavyweight large-porous; HW-SP, heavyweight small-porous; LW-LP, lightweight large-porous.
Measurement of mesh deformation
Mesh shrinkage was observed in all experimental groups (Fig. 2). The least shrinkage was noted in the HW-LP group, which lost 13.8% (4.8%) of its original size. The HW-SP and LW-LP meshes showed a higher shrinkage rate, decreasing by 19.5% (9.3%) and 25.5% (8.9%), respectively (Fig. 3).
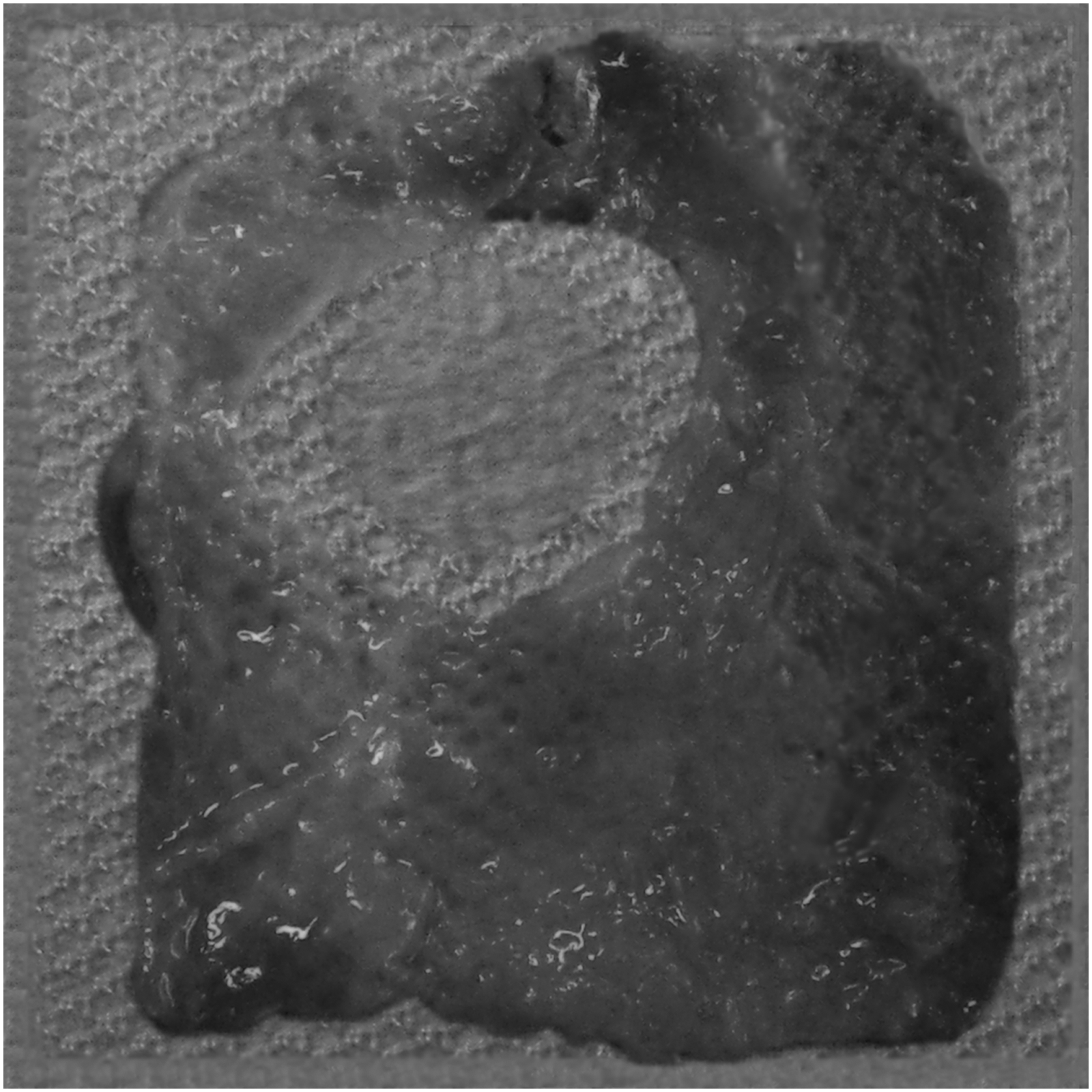
Mesh shrinkage of a lightweight large-porous mesh. An explanted lightweight large-porous mesh was projected 1:1 onto a picture of the same mesh captured before implantation using Photoshop version 12 (Adobe Systems, San Jose, CA).
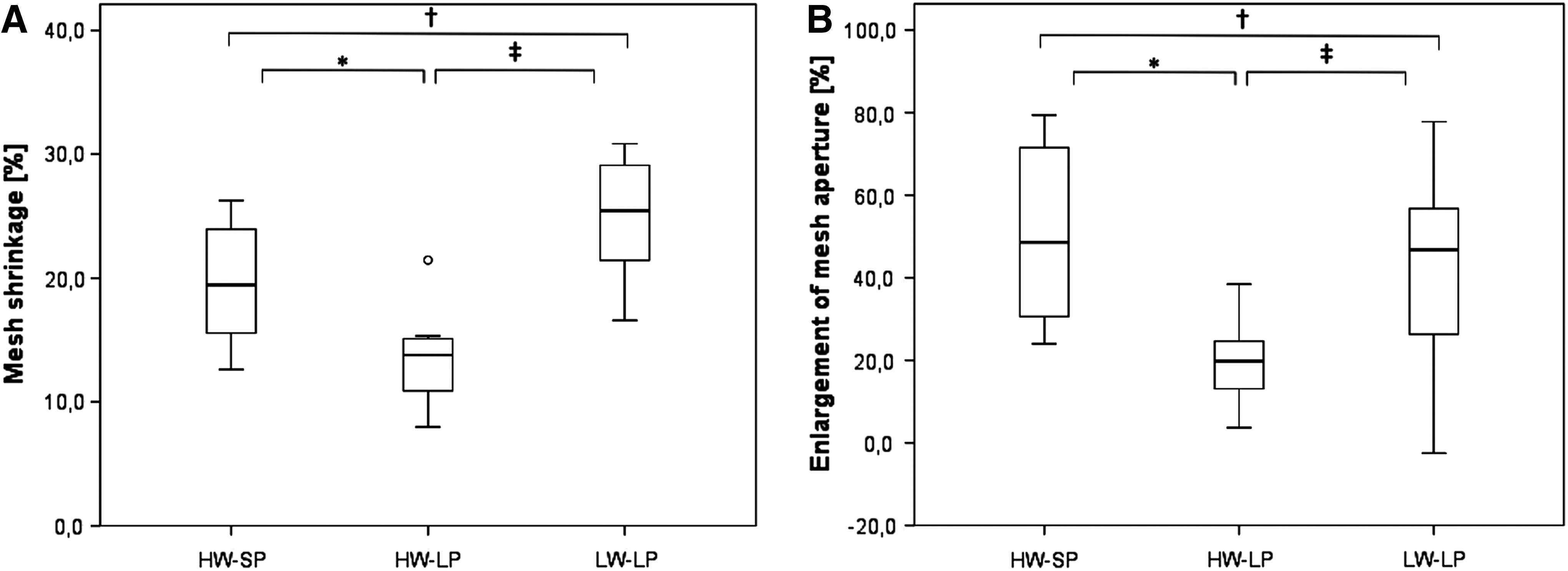
Deformation for heavyweight small-porous (HW-SP), heavyweight large-porous (HW-LP), and lightweight large-porous (LW-LP) mesh.
Mesh shrinkage correlated positively with enlargement of the mesh aperture (rs=0.427, P=.037). Correspondingly, the mesh aperture within the HW-SP and the LW-LP groups exhibited the greatest degree of enlargement, increasing by 48.6% (43.9%) and 46.8% (33.8%), respectively. Enlargement of the mesh aperture was less within the HW-LP group, increasing by 19.8% (12.8%) (Fig. 3).
Evaluation of adhesions
Within the HW-SP-group, the meshes were in most cases completely covered with adhesions involving larger parts of the mesh area. The LW-LP meshes showed an intermittent pattern of adhesion involving the least amount of mesh area compared with HW-SP and HW-LP (Table 4). The esophagus, stomach, and liver always adhered to the mesh and showed no signs of lesions. Within the HW-SP and LW-LP groups, adhesions involving the spleen could be found in 1 case each. No further organs were involved. The adhesion score was highest within the HW-SP group [11.0 (1.0)]. Lower scores were found for HW-LP [8.0 (1.0)], whereas the LW-LP group showed the lowest score [6.0 (2.0)] (Fig. 4). The adhesion score correlated positively with the score of esophagogastric fixation (rs=0.700, P<.001). Correspondingly, the score of esophagogastric fixation showed significantly higher values for HW-SP compared with LW-LP [4.5 (1.0) versus 3.3 (2.0); P=.021]. No significant difference was found upon comparing HW-SP with HW-LP [4.5 (1.0) versus 4.0 (1.0); P=.574] and HW-LP with LW-LP [4.0 (1.0) versus 3.3 (2.0); P=.065].
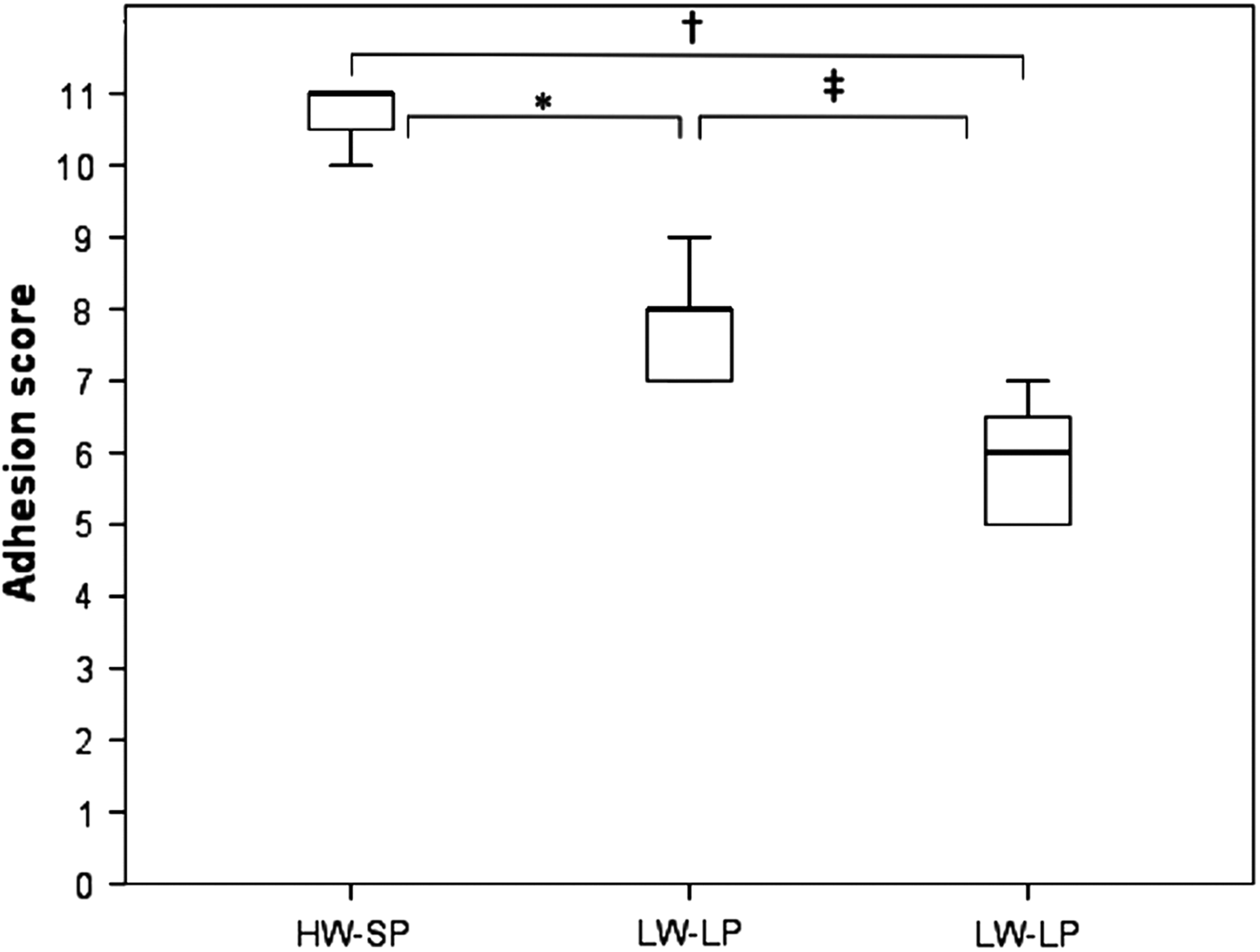
Adhesion score for heavyweight small-porous (HW-SP), heavyweight large-porous (HW-LP), and lightweight large-porous (LW-LP) mesh according to the Surgical Membrane Study Group. 23 By Mann–Whitney U test, *P<.001, †P<.001, ‡P=.001.
Evaluation of mesh migration and erosions
No mesh migration was observed. All meshes retracted from the hiatal border at each measured position, so the mesh margin never had direct contact with the esophagus. In accordance, no signs of erosion or stenosis could be observed. The median of mesh retraction correlated positively with mesh shrinkage (rs=0.414, P=.045), and the lowest median retraction was observed within the HW-LP-group. No significant differences were found between the HW-SP and the LW-LP groups in this regard (Table 4).
Histological analysis
Histology showed signs of a chronic inflammatory reaction within all experimental groups. All meshes were completely surrounded by connective tissue (Fig. 5). Variance analysis showed no significant difference with regard to partial volume of mononuclear cells. Partial volume of Ki-67-positive cells was significantly higher for HW-LP compared with LW-LP. Partial volume of collagen type I was significantly higher for HW-SP compared with HW-LP. No significant differences were found with regard to partial volume of collagen type III. The collagen type I/III ratio was highest for the HW-SP meshes (Table 5).
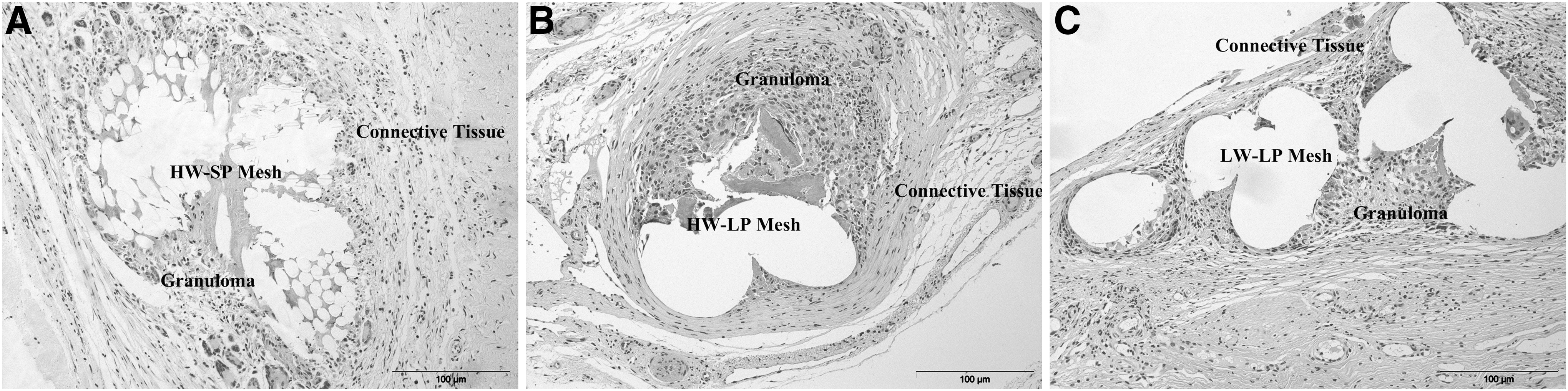
Mesh and surrounding tissue stained with hematoxylin and eosin:
Data are median values (interquartile range).
By Kruskal–Wallis test.
P<.050 by Mann–Whitney U test, heavyweight large-porous (HW-LP) versus lightweight large-porous (LW-LP).
P<.050 by Mann–Whitney U test, HW-SP, heavyweight small-porous (HW-SP) versus HW-LP.
P<.050 by Mann–Whitney U test, HW-SP versus LW-LP.
Discussion
An appropriate method for mesh reinforcement at the esophageal hiatus must be safe and stable. For the first time this study has investigated the influence of weight and structural specifications on mesh behavior at the hiatus.
Mesh deformation could be observed in all experimental groups. The interaction between tissue contraction, which is driven by the cellular elements of foreign body reaction, 16 and the meshes' structural and mechanical attributes may be responsible for the observed differences in mesh shrinkage. As Harrell et al. 17 hypothesized, small pores may facilitate a more efficient cross-linking between neighboring fibroblasts, which could account for greater propensity toward mesh shrinkage inherent to the HW-SP meshes compared with the HW-LP prostheses. On the other hand, the highest shrinkage rates were observed for LW-LP meshes. This finding is consistent to experimental studies on polypropylene meshes for ventral hernia repair reporting higher shrinkage rates for lightweight meshes compared with heavyweight prostheses.18,19 Although pore size is similar to the HW-LP meshes, reduction of polymer material is associated with an increase in mesh elasticity, 20 which may cause lightweight prostheses to respond with less resistance to tissue contraction. An important finding of this study is the positive correlation between mesh shrinkage and the enlargement of the mesh aperture for the esophagus. Consecutively, high propensity toward mesh shrinkage might be associated with increased risk of hiatal hernia recurrence.
The HW-SP and HW-LP meshes showed solid adhesions mostly covering large parts of the mesh area. Adhesion formation was less intense for the LW-LP meshes. Foreign body reaction and adhesion formation are assumed to be stimulated by surface and amount of implanted foreign material.21,22 Thus, the stimulus for adhesion formation may probably be reduced by large porous and lightweight mesh design. A further finding of this study is that the intensity of adhesion formation correlated with fixation of the esophagogastric junction. Adhesions to HW-SP and HW-LP meshes involved large parts of the cardia. Consequently, we postulated that intense adhesion formation may be beneficial for mesh reinforcement at the hiatus because it may prevent hiatal hernia recurrence analogous to the cardiopexy as proposed by Hill. 23
No tendency toward mesh migration, stenosis, or erosion of the esophagus could be observed within this study. At explantation, all meshes were found in a centralized position around the esophagus showing a retraction form the hiatal border. To our knowledge, there is only one experimental study reporting complications associated with circular prostheses. In that study, Jansen et al. 11 found esophageal erosion of polypropylene meshes in 11 of 16 rabbits; however, the anatomic disproportion of the rabbits' small esophagus and the thickness of the meshes conceived for use in humans must be taken into consideration. In porcine studies on circular mesh prostheses, no signs of esophageal erosion were observed.8,9 There are several clinical studies reporting on complications of circular mesh prostheses.24–26 It remains unclear whether these complications may be attributed to the circular mesh form or, more likely, to technical problems of mesh placement and the surgeon's experience. Within the largest published series, mesh-related complications were found in only 3 of 306 patients (1.0%). 25 Thus, even in the clinical setting this problem seems not to be that relevant.
Evaluation of foreign body reaction showed less positivity for Ki-67 for the LW-LP meshes compared with the HW-LP meshes, suggesting less inflammatory activity. Considering the structural similarity of the LW-LP and the HW-LP meshes, the results of this study provide evidence that reducing mesh weight is associated with higher biocompatibility. On the other hand, with regard to the comparison of HW-SP and HW-LP meshes, varying structural specifications like pore size and filament structure did not have a significant influence on biocompatibility. However, one does question whether or not pursuing the paradigm of biological inertness is reasonable regarding surgical meshes placed at the hiatus. Potential benefits of the implant's biological behavior like distinct adhesion formation fixing the esophagogastric junction or solid tissue integration by surrounding fibrosis seem to be attenuated in LW-LP meshes.
Solid tissue integration is essential in order to prevent mesh migration and erosion into the adjacent organs. HW-SP meshes are known to induce a distinct fibrosis and form a cicatrice plate enclosing the implanted mesh prostheses. 27 This tendency could also be observed in this experimental setting. Furthermore, immunostaining revealed the highest collagen type I/III ratio for the HW-SP meshes. The quality of collagen fiber scaffold may be decisive for its mechanical stability. Although collagen type III is found within reticular soft tissue, solid tissues such as fascia or tendons are composed of scaffolds based primarily on collagen type I. 28 Experimental studies on mesh prostheses used for ventral hernia repair in humans showed lower collagen type I/III ratios when explanted because of recurrent hernia. 29
Consequently, weight and pore size both have a decisive influence on mesh behavior at the esophageal hiatus. Heavyweight polypropylene meshes may be advantageous for hiatal mesh reinforcement, providing the best characteristics regarding form stability, adhesion formation, and tissue integration. Both heavyweight meshes showed a solid fixation of the esophagogastric junction by adhesions. These, in turn, may contribute to a reduction of hernia recurrence. Large pore size is associated with the best form stability in heavyweight meshes. The small-porous structure is superior with regard to solidity of tissue integration, which may prevent mesh migration.
There are certain limitations to be discussed. First, with regard to latency of mesh-related complications of up to several years, a follow-up of 8 weeks may be insufficient. However, because according to experimental evidence mesh shrinkage and tissue integration seem to stabilize within 60 days, the tendency toward mesh-related complications may be detectable by this experimental setting.30,31 Furthermore, all meshes were evaluated as circular-shaped prostheses because, according to our clinical and experimental experience, circular hiatal mesh reinforcement proved to be safe and effective.8,25 Finally, the implications of this study are limited by its experimental nature. We postulated that beneficial biological mesh behavior at the hiatus is characterized by form stability, solid fixation of the esophagogastric junction by adhesions, and solid tissue integration. Moreover, it should not exhibit a tendency toward mesh-related complications. Whether mesh types matching these experimental criteria provide safe and effective hiatal mesh reinforcement in humans will need to be confirmed by future clinical studies.
In conclusion, structural configuration has to be considered when selecting a mesh for application at the hiatus. Heavyweight polypropylene meshes may be advantageous for the application at the hiatus by providing a solid fixation of the esophagogastric junction by adhesions, which may contribute to a reduction of hernia recurrence. In heavyweight meshes, large pore size is associated with the best form stability, and the small-porous structure may be superior with regard to tissue integration. The latter may prevent mesh migration.
Footnotes
Acknowledgments
We would like to thank Elizabeth Corrao and Maya Müller-Wolf for reviewing the manuscript as a native speaker. Furthermore, we would like to thank Covidien (Neustadt, Germany) for providing mesh samples for this study.
Disclosure Statement
No competing financial interests exist.