
Abstract
Abstract
Objective:
To describe our technique of robotic rectovesical fistula (RVF) repair through the report of a case unique for its pathogenesis. RVF is a rare but devastating complication of prostatic surgery and can nowadays be managed with a minimally invasive approach.
Patient and Methods:
We describe in detail all the steps of our robotic RVF repair, performed on a 76-year-old man who developed RVF after radical prostatectomy. The RVF had been induced by tissue erosion due to Hem-o-lok® (Teleflex Medical, Research Triangle Park, NC) clips and had been unsuccessfully treated with an over-the-scope clip.
Results:
Our surgery was successful with an operative time of 70 minutes and an estimated blood loss of 150 mL. The postoperative course was uneventful, and the patient was discharged on postoperative Day 3.
Conclusions:
Our technique of robotic RVF repair was safe and effective. Care must be taken when considering new, endoscopic devices for the cure of RVF. A prospective study with a long follow-up is advised to validate our results.
Introduction
R
Patient and Methods
Patient
A 76-year-old man with a clinically localized prostate cancer had undergone a robotic radical prostatectomy for intermediate-risk disease (Gleason score of 3+4=7, pT2cN0M0R0). During the surgery no rectal injuries were reported, and Hem-o-lok® (Teleflex Medical, Research Triangle Park, NC) clips were used for the nerve-sparing approach. The postoperative course was uneventful, and no adjuvant radiotherapy was needed, considering the pathological findings. Two months later, the patient experienced urine leakage from the rectum, pneumaturia, and fecaluria; cystourethrography confirmed the presence of an RVF. After a conservative approach was attempted without success, a loop colostomy was performed, and a transurethral catheter was placed. Despite the fecal diversion, however, at 6 months the RVF was not closed. An abdominal computed tomography scan detected a 1-cm RVF on the right posterolateral wall of the bladder. Cystoscopy confirmed the presence of the RVF not far from the urethrovesical anastomosis, revealing two Hem-o-lok clips eroding the bladder surface; the clips were then endoscopically removed. An endoscopic repair of the RVF was then attempted during rectoscopy, deploying an over-the-scope clip system called OTSC (Ovesco Endoscopy, Tübingen, Germany) 9 and applying fibrin glue. Despite these procedures, however, the fistula persisted. At almost 1 year after the radical prostatectomy, the patient came to our attention with his symptoms unchanged. Based on our prior experience in the setting of laparoscopic and robot-assisted RVF repair, a robot-assisted fistula repair was planned.
Surgical technique
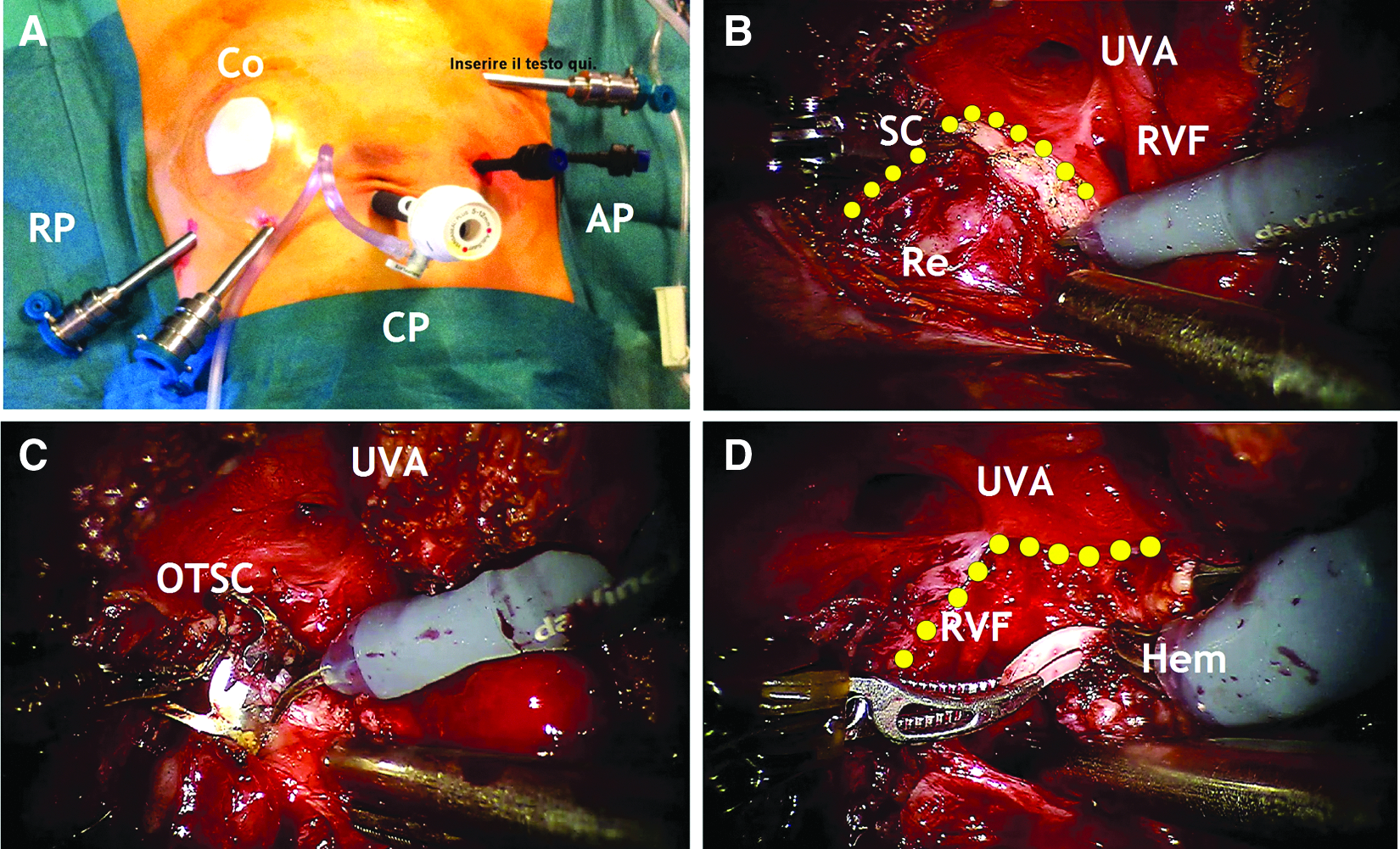
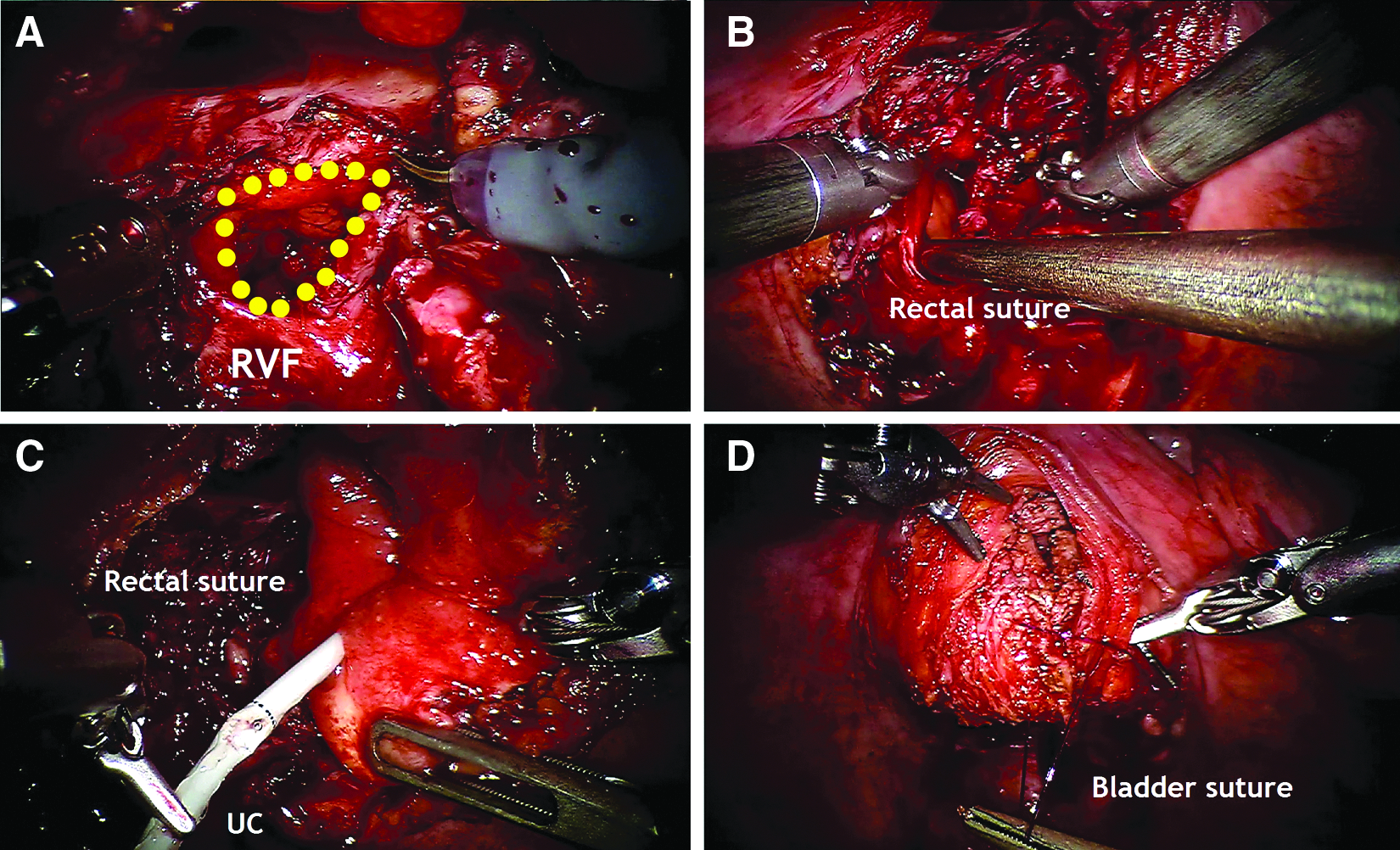
The patient was placed in a modified lithotomic position, with the legs abducted and parallel to the level of the bed. A 30° Trendelenburg position was obtained, and pneumoperitoneum was established with 12 mm Hg insufflation pressure. The surgical technique is detailed in Figure 1. The port placement was identical to that commonly used for robotic radical prostatectomy, and care was taken not to injure the left colostomy. Six trocars were placed: a 12-mm camera port 2 cm above the umbilicus, two 8-mm robotic ports bilaterally at a distance of at least 8 cm from the camera port, and a third 8-mm robotic port 5 cm above the left anterior superior iliac spine. Finally, two 5-mm assistant ports were triangulated above the right robotic port, as shown in Figure 2A. Surgery began with careful lysis of small bowel adhesions, caused by previous surgeries. A sagittal, bivalve cystotomy was performed on the bladder dome and the posterior wall (Fig. 2B), exposing the fistulous orifice on the right posterolateral wall, near the right ureteral meatus. During the inspection of the RVF, the OTSC was found attached to the rectal mucosa and removed (Fig. 2C). Two eroding Hem-o-lok clips were also identified in the fistulous tract and removed (Fig. 2D). A careful dissection of the rectovesical plane was performed, starting from the RVF. At the end of the dissection, an RVF measuring about 2 cm was found (Fig. 3A). Considering the presence of healthy tissue around the fistulous tract, we decided not to resect the borders of the RVF. A running, one-layer suture of the rectal breach was performed using 3-0 poliglecaprone (Fig. 3B). After temporary catheterization of the right ureteral meatus to ensure its patency (Fig. 3C), the bladder was closed in two layers: a 3-0 poliglecaprone running suture for the mucosa and a 2-0 V-Loc™ (Covidien, New Haven, CT) for the muscle, adventitia, and peritoneum, restoring the Douglas pouch (Fig. 3D). A 18 Ch. Foley urethral catheter was placed. The operative time was 70 minutes, and the estimated blood loss was 150 mL. The postoperative course was uneventful, and the patient was discharged on postoperative Day 3. The urethral catheter was removed 15 days later, after normal cystourethrography. Bowel continuity is planned to be restored at 2 months from surgery.
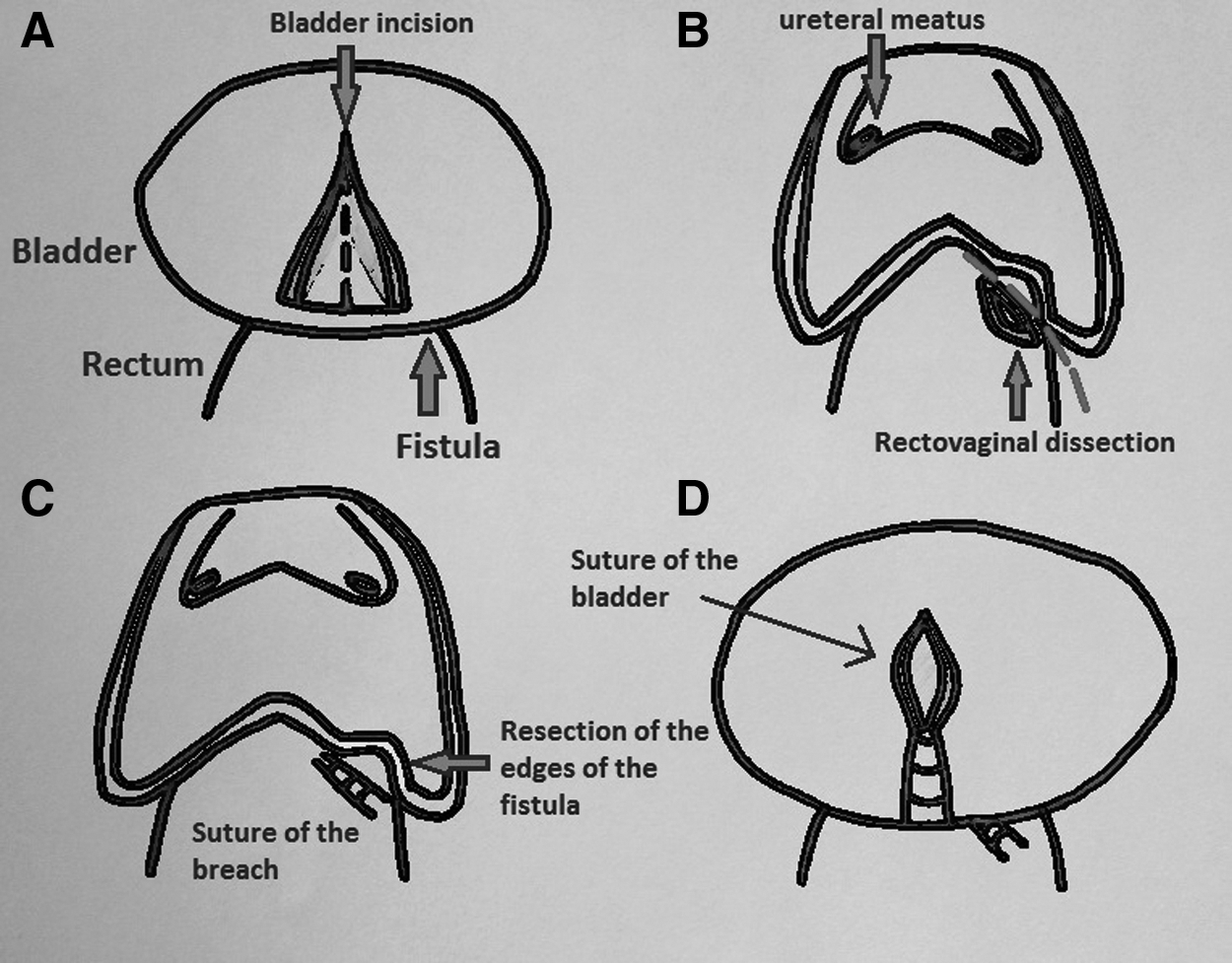
Surgical technique of rectovesical fistula repair:
Discussion
RVF is a rare but devastating complication that can usually develop after prostatic ablative or extirpative procedures. The RVFs were differentiated into two groups by Munoz et al. 10 : the benign ones (infectious and traumatic) and the malignancy-related complex fistulas, for which treatment is even more challenging. Conservative management with placement of a transurethral catheter is often initially attempted with success rates up to 25%–50%11–13 ; the second step of treatment is the fecal diversion, especially if the fistula is not closed after 3 months of catheterization. 4 In our patient, an endoscopic management had been attempted with the placement of an OTSC. These clips have achieved promising results for the treatment of colorectal postsurgical fistulas that are <15 mm, including rectovaginal and colocutaneous ones. 14 However, the indication of such clips for the treatment of RVF remains controversial, as shown in our patient: the fistula was not closed. and an enlargement in diameter was even demonstrated during the next surgery.
As for the surgical treatment of RVF, several techniques have been described, including transanal, transanorectal, transsphincteric, transabdominal, perineal, and combined approaches.15–18 There is no consensus about which is the best method, even if the rectal flap method with the York–Mason approach 7 and the gracilis muscle flap interposition are considered the most common procedures, with high success rates and minimal morbidity. 4 Basic surgical principles include excision and debridement of the fistula tract to healthy tissue, separation of the rectal and bladder suture lines with tissue interposition, especially for fistulas in irradiated fields, and effective urinary and/or fecal diversion.3,19 Some authors believe that fecal diversion is mandatory; others feel that it is necessary only when there have been previous failed repairs, complex fistulas, or a history of radiotherapy. 20 In our patient, we were able to perform a very precise dissection of the rectovesical plane thanks to the improved vision and dexterity of the robotic platform. On the other hand, as we found very healthy and vascularized tissue around the fistulous orifice, we decided not to resect the RVF with a wide margin, whereas we took care to separate our rectal and bladder suture lines. As our patient had not undergone radiation therapy, we did not interpose any flap or tissue between the rectum and the bladder.
Minimally invasive procedures in urology have spread widely in recent years. A few laparoscopic and robotic RVF repairs have recently been described, with promising results.1,3,4,8 Our robotic technique is modeled after open principles, taking advantage of the enhanced magnification, improved dexterity, and improved precision of movements. Furthermore, the minimally invasive, transperitoneal approach permits an exposition and a dissection of the deep pelvic cavity structures that cannot be achieved with another approach. With the same robotic technique we treated 8 other cases with an excellent success rate, even if our follow-up is limited, and a prospective study should be performed to confirm these preliminary results.
A final comment addresses the unique pathogenesis of our case, involving a few Hem-o-lok clips that eroded the rectal and bladder walls. Several complications due to these clips have been reported in the literature, including migration, calcification, or induction of fibrosis. A recent study reported a Hem-o-lok-induced bladder erosion and concluded by advising minimizing their use in the midline, in deferent ducts, or close to the urethrovesical anastomosis during radical prostatectomy. 21 In our case, we believe that the clips were placed too close to the rectal wall, thus favoring the formation of the RVF. In the light of these reports, care must be taken when using Hem-o-lok clips during radical prostatectomy.
Conclusions
Our technique of robotic RVF repair represents an attractive, minimally invasive alternative to the classic, open procedures. Care must be taken when considering new, endoscopic devices for the cure of RVF. The safety and efficacy of our technique must be validated by the execution of a prospective study with a long follow-up.
Footnotes
Disclosure Statement
No competing financial interests exist.