
Abstract
Abstract
Introduction:
Objective performance feedback has potential to maximize the training benefit of laparoscopic simulators. Instrument movement metrics are, however, currently the preserve of complex and expensive systems. We aimed to develop and validate affordable, user-ready software that provides objective feedback by tracking instrument movement in a “take-home” laparoscopic simulator.
Materials and Methods:
Computer-vision processing tracks the movement of colored bands placed around the distal instrument shafts. The position of each instrument is logged from the simulator camera feed and movement metrics calculated in real time. Ten novices (junior doctors) and 13 general surgery trainees (StR) (training years 3–7) performed a standardized task (threading string through hoops) on the eoSim (eoSurgical™ Ltd., Edinburgh, Scotland, United Kingdom) take-home laparoscopic simulator. Statistical analysis was performed using unpaired t tests with Welch's correction.
Results:
The software was able to track the instrument tips reliably and effectively. Significant differences between the two groups were observed in time to complete task (StR versus novice, 2 minutes 33 seconds versus 9 minutes 53 seconds; P=.01), total distance traveled by instruments (3.29 m versus 11.38 m, respectively; P=.01), average instrument motion smoothness (0.15 mm/second3 versus 0.06 mm/second3, respectively; P<.01), and handedness (mean difference between dominant and nondominant hand) (0.55 m versus 2.43 m, respectively; P=.03). There was no significant difference seen in the distance between instrument tips, acceleration, speed of instruments, or time off-screen.
Conclusions:
We have developed software that brings objective performance feedback to the portable laparoscopic box simulator. Construct validity has been demonstrated. Removing the need for additional motion-tracking hardware makes it affordable and accessible. It is user-ready and has the potential to enhance the training benefit of portable simulators both in the workplace and at home.
Introduction
O
There have been many previous studies describing techniques for tracking instrument movement in laparoscopic box simulators.8,11–15 The problem with these systems is that they require either multiple cameras or additional and costly motion-detection hardware. The “InsTrac” software described here is different in that it works through the camera feed and requires only a standard desktop or laptop computer running either the Windows™ (Microsoft, Redmond, WA) or the Mac™ (Apple, Cupertino, CA) operating system. It is “user-ready” and available for online download (eoSurgical.com/products/InsTrac). The eoSim minimally invasive surgery simulator used in this study (eoSurgical™ Ltd., Edinburgh, United Kingdom) (regular retail price from $600 U.S.) has recently been demonstrated to have both construct validity and concurrent validity with the established but more expensive Fundamentals of Laparoscopic Surgery (FLS™) simulator (Society of American Gastrointestinal and Endoscopic Surgeons, Los Angles, CA). 16
Generating objective performance metrics in a take-home box simulator may represent the optimal combination of performance feedback, real instrument handling, and accessibility.9,17,18 In this study we report the development and construct validity of software that aims to achieve this.
Materials and Methods
Instrument tracking software
Computer-vision technology is used in many applications in high-dependency environments such as space travel, high-fidelity industrial manufacturing, and unmanned vehicles. 19 We have developed a color-thresholding motion-tracking program that uses the “hue,” “saturation,” and “value” color classification system to track the movement of colored laparoscopic instrument tips. The Hue-Saturation-Value system is superior to red, green, blue color coding as it separates “luma” (image intensity) from “chroma” (color information). This is important in maintaining tracking during the changing light conditions caused by movement of the instruments.
With a blue band wrapped around the left instrument tip and a red one around the right, each frame from the simulator camera's image feed is analyzed. In real time every frame is thresholded for each color, and the center of the resultant thresholded area is plotted as an x- and y-axis coordinate (Fig. 1). Combining these position data with elapsed time allows several metrics to be calculated. We chose to track in two dimensions as a recent experimental study demonstrated a strong correlation between two-dimensional and three-dimensional metrics. 12 This suggests that two-dimensional may be as effective as three-dimensional tracking in generating metrics useful to provide incentives for practice and monitor skills progression. The movement metrics that we chose to calculate are based on parameters and formulas previously shown to be able to distinguish novice from expert surgeons in studies that used virtual reality or other complex instrument tracking hardware7,8,11–13,20,21 (Fig. 2 and Table 1).
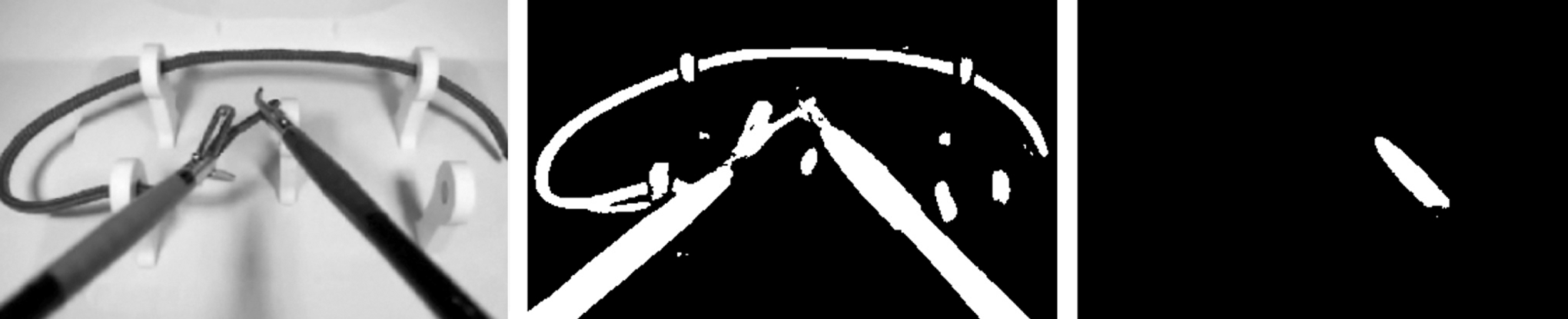
The process of taking a frame from the simulator camera output, thresholding for non-white, and then refining the thresholding to the specific instrument tip color.
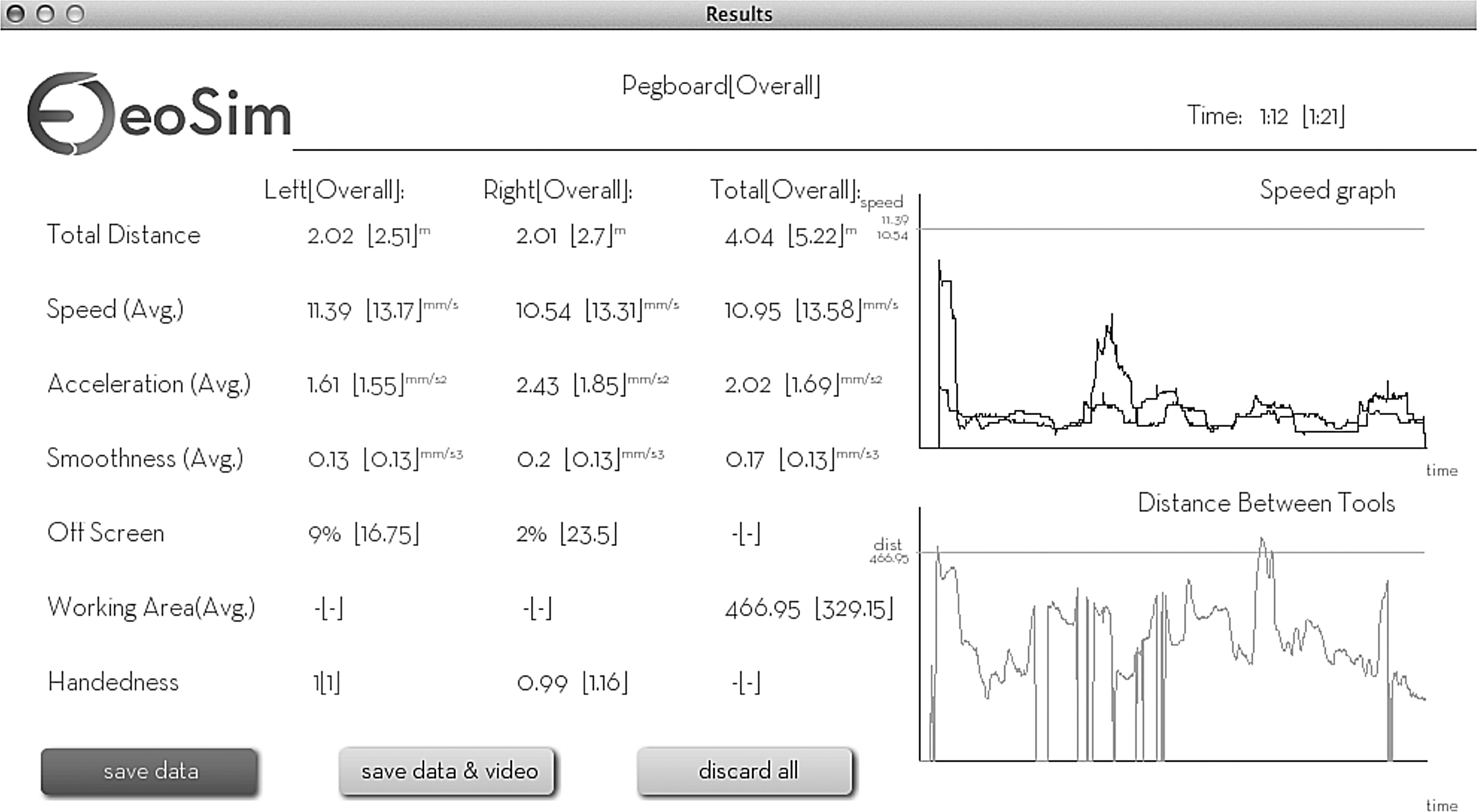
The instrument movement metrics results screen.
Construct validation
Two groups undertook a standardized laparoscopic task of threading string through hoops on the eoSim take-home simulator. Neither group had used the eoSim previously. Prior to performance assessment, each participant had 30 minutes of practice to familiarize him- or herself with the equipment. Group 1 consisted of 10 novices (Foundation Year [FY] junior doctors) with no previous laparoscopic experience. Group 2 comprised 13 general surgical specialty trainees (StR) (training years 3–7) who all regularly perform laparoscopic procedures.
Performance assessments were overseen by the authors, and the metrics result screen was recorded for each participant (Fig. 2). These data were collated, and statistical analysis was performed using unpaired t tests with Welch's correction (Prism 6 software; GraphPad™ Software Inc., San Diego, CA).
Results
Instrument tracking software
The software was run on the study participants' personal computers, including machines of different ages with both Mac and Windows operating systems. This demonstrates that it is applicable to real-life scenarios and has the potential to be used by individuals at home. A calibration step in the software set-up ensures that instrument tips are reliably tracked. When the calibration function is selected, five circles are superimposed on the screen: in the four corners and at the center of the visual field. The instrument tips are moved such that they are both within the same circle at the same time. When the software detects their presence consistently for 5 seconds, that circle turns green. The process is then repeated for the remaining four circles. We tested this in different lighting conditions, ranging from very bright ambient sunlight to a dark room, with just the built-in light-emitting diodes and no ambient light. Both instrument tips were detected in all areas of the screen in all cases. The only way we were able to interfere with the tracking was to place another red or blue object within the visual field. All practice models used were thus free from red or blue aspects.
Construct validation
Significant differences were observed between the novice FY group and experienced StR group in the following variables: time to complete task, StR versus novice, 2 minutes 33 seconds versus 9 minutes 53 seconds (P=.01); total distance traveled by instruments, 3.29 m versus 11.38 m, respectively (P=.01); average instrument motion smoothness, 0.15 mm/second 3 versus 0.06 mm/second 3 (P<.01); and handedness (mean difference between dominant and nondominant hand), 0.55 m versus 2.43 m (P=.03) (Fig. 3). The dominant hand was demonstrated to move further than the nondominant hand.
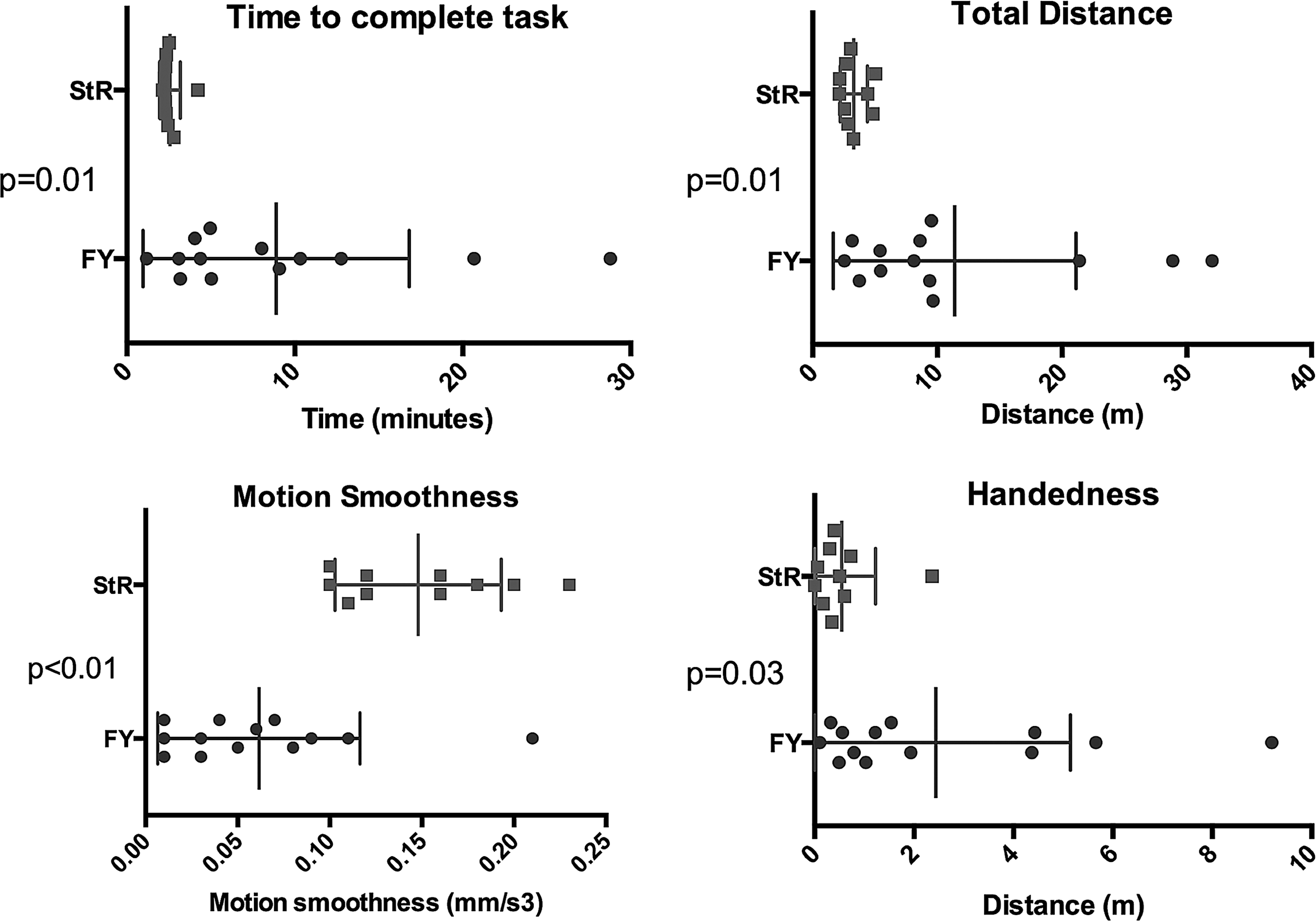
Significant differences in instrument movement metrics between novices (Foundation Year [FY]) and active laparoscopic surgeons (surgical trainees [StR]). Total distance represents the combined left- and right-hand instruments' path length. Motion smoothness represents a measure of the rate of change of acceleration or “jerkiness” of the instrument movement. Handedness represents the mean difference in instrument path length between dominant and nondominant hands. From the data points, mean and standard deviation values (vertical lines) were calculated. Statistical analysis was performed using the unpaired t test with Welch's correction.
There was no significant difference seen in the average distance between instrument tips, average speed of instrument tips, mean acceleration, or time out of operative field (Fig. 4).
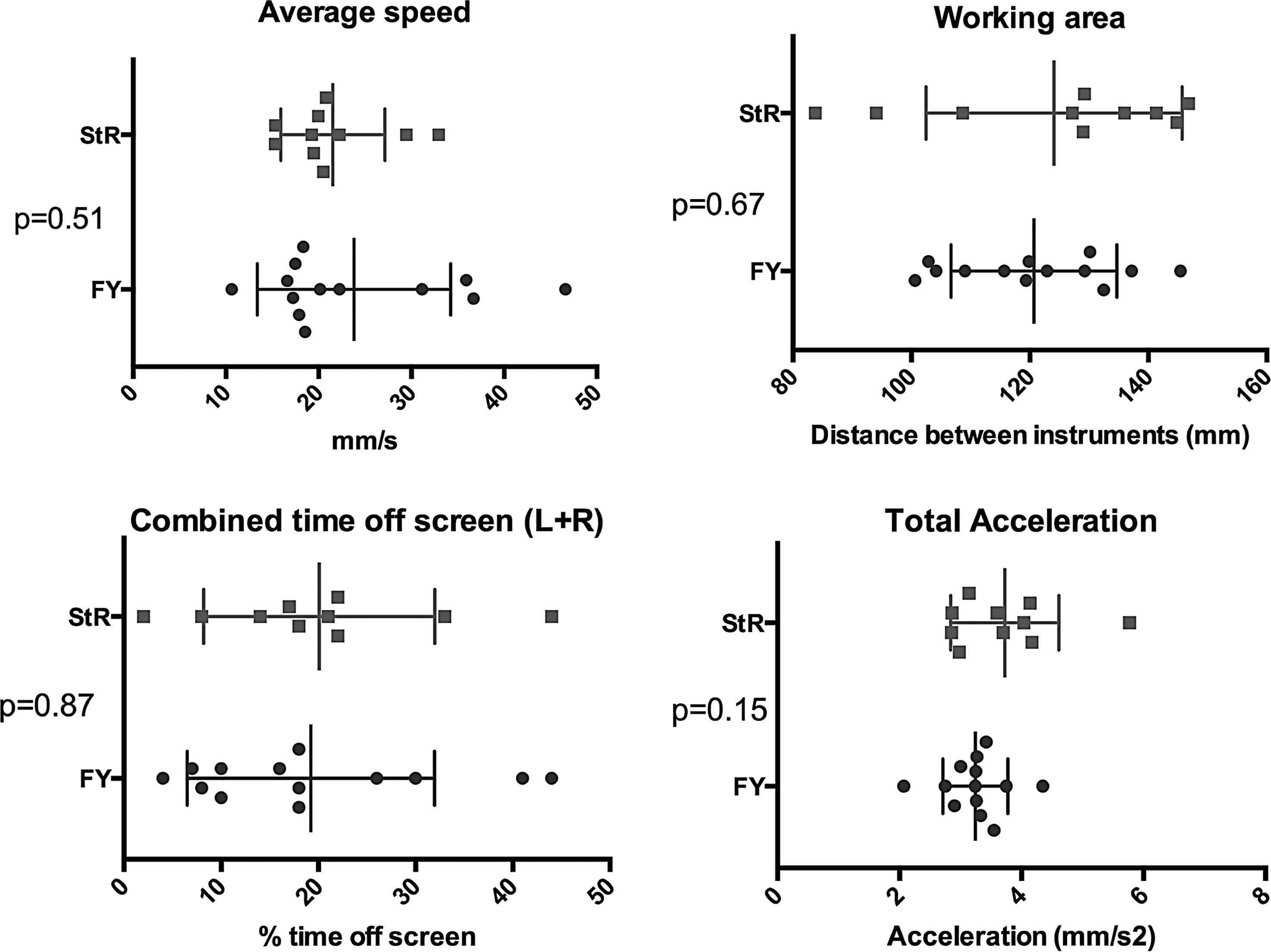
Instrument movement metrics in novices (Foundation Year [FY]) and active laparoscopic surgeons (surgical trainees [StR]), which were not significantly different. Working area represents the average distance between the instrument tips while the task is completed. A larger average distance indicates the instruments are occupying a larger operating area within the visual field. From the data points, mean and standard deviation values (vertical lines) were calculated. Statistical analysis was performed using the unpaired t test with Welch's correction. L, left; R, right.
Discussion
This study demonstrates construct validity of an accessible performance measurement tool in a portable laparoscopic box simulator. It is an advance in the field because it is user-ready and requires only a standard desktop or laptop computer. By using the camera feed alone, it removes the need for additional cameras or expensive motion-sensing hardware. This study was completed in a classroom setting, but the compatibility with personal computers and the portability of the system make it suitable as a take-home device.
The accessibility of take-home simulation has the potential to facilitate skills acquisition free from working-time restrictions and the problem of limited access to institutional simulators.10,18 It is known that skills development in a simulated environment helps optimize the utility of time spent in the real operating theater. 17 It is also known that simulation training is most effective when goal-directed and accompanied by performance feedback.2,17 This software package successfully combines accessibility and objective performance feedback.
Construct validity is demonstrated by distinguishing between novices and surgical trainees with previous laparoscopic experience (using metrics of time, total distance moved by instruments, degree of ambidexterity, and motion smoothness). Distance between instrument tips, average speed of instrument tips, mean acceleration, and time out of operative field were not distinguishing metrics in this study.
The significant differences in time and total instrument distance moved to complete the task are consistent with other studies comparing instrument movement metrics between novice and experienced surgeons.8,11,12 The greater variance of the data points in the novice group is also in keeping with other studies using both virtual reality and augmented reality systems.12,21 The finding that novices demonstrated greater reliance on their dominant hand is consistent with previous work highlighting a greater degree of ambidexterity in trained surgeons. 22 Motion smoothness (“jerk”) is a measure of the rate of change of acceleration. There is conflicting evidence as to its usefulness as a measure of surgical performance.23–25
The lack of a significant difference between the groups regarding distance between instrument tips, average speed of instrument tips, mean acceleration, and time out of operative field is also in keeping with the findings of some experimental studies assessing instrument tip movement, but at odds with others.12,26,27 It is noted that most existing studies assessing such metrics are small, likely because of limited access to equipment capable of generating appropriate data. The accessibility of the eoSim simulator and “InsTrac” software package presents an opportunity to facilitate much larger, multicenter studies.
We have developed software that brings objective performance feedback to the portable laparoscopic box simulator. Construct validity has been demonstrated. Removing the need for additional motion-tracking hardware makes it affordable and accessible. It is user-ready and has potential to enhance the training benefit of portable simulators, both in the workplace and at home.
Footnotes
Acknowledgments
The authors would like to thank all study participants for facilitating the data collection.
Disclosure Statement
R.W.P., M.A.H., P.M.B., and I.A.M.H. have taken steps to address the poor access to surgical simulation tools by designing and manufacturing affordable take-home simulation equipment. They established a company, eoSurgical Ltd. (Edinburgh, United Kingdom) (eoSurgical.com), in order to achieve this. All authors are shareholders in eoSurgical Ltd. The eoSim take-home laparoscopic simulator used in this study is manufactured by eoSurgical Ltd. The InsTrac software was developed in conjunction with a separate company, Peekabu Studios Ltd. (Edinburgh), and is marketed by eoSurgical Ltd.