
Abstract
Abstract
Background:
This study aimed to evaluate the safety and quality of laparoscopic colorectal cancer surgery undertaken by trainees.
Patients and Methods:
From a prospectively maintained database, we identified 456 consecutive patients who underwent laparoscopic resection for colorectal cancer between 2006 and 2010. Short-term operative outcomes, relapse-free survival (RFS), and overall survival (OS) were compared between operations undertaken by the experts (E group) and trainees (T group). Multivariate analyses were performed for RFS and OS in stage II/III disease.
Results:
Trainees performed 313 surgeries (68.6%) and completed the procedure by themselves in 297 cases (94.9%). Short-term outcomes, including operative time, blood loss, conversion, complication, mortality, and retrieval of less than 12 lymph nodes, were comparable between the E group and the T group. After a median follow-up period of 35 months, RFS and OS were similar between the two groups, with the exception of OS for stage II (3-year OS for E group versus T group, 96.9% versus 87.0%; P=.029); however, this difference disappeared after multivariate analyses. Multivariate analyses showed that positive resection margin and higher log carcinoembryonic antigen (CEA) levels were associated with lower RFS. Furthermore, increasing age, positive resection margin, higher log CEA levels, intraoperative surgeon exchange, rectal cancer, postoperative complications, absence of postoperative chemotherapy, and shorter operative time were associated with poor OS.
Conclusions:
Laparoscopic operations undertaken by trainees did not negatively affect short-term outcomes and were not associated with impaired mid-term oncologic outcomes. Our findings support early initiation of training in laparoscopic surgery for colorectal cancer treatment.
Introduction
D
Patients and Methods
Patients
From a prospectively maintained single-institution database, we identified 456 consecutive patients who underwent laparoscopic resection for colorectal cancer between 2006 and 2010. The indications for laparoscopic surgery were colorectal cancer tumors that did not form a bulky mass and did not involve a massive lymph node or invasion of the adjacent organs. Surgeries were performed by an experienced, board-certificated, expert surgeon (T.Y.) or by 10 trainees who had been trained in open and laparoscopic surgery for 1–3 years previously.
Data regarding the patients' demographics, operative details and outcomes, and follow-up status were collected prospectively. Tumors were staged according to the Sixth Tumor-Node-Metastasis (TNM) classification of the International Union Against Cancer on the basis of the histological findings of the surgical specimens.
This study was approved by the local committee for medical ethics and clinical studies of Kyoto Medical Center, Kyoto, Japan.
Surgical procedures
The surgical procedures used for laparoscopic colorectal resection (LCR) at our institution have been previously described.13,16,17 The surgical team comprised an operating surgeon (primary surgeon), assistant surgeon, and endoscopist. In total, five ports were inserted: the 12-mm umbilical port for the telescope and one port each (diameter, 5–12 mm) into the left upper, left lower, right upper, and right lower abdominal quadrants. Lymph node dissection was performed in accordance with the oncologic surgical principles recommended by the Japanese Society for Cancer of the Colon and Rectum18,19; in brief, a D3 lymph node dissection, including the pericolic nodes (local nodes), mesocolic nodes (intermediate nodes), and nodes at the origin of the feeding artery (main nodes), was generally performed, except in cases of elderly patients, of tumors confined to the submucosa, or of palliative resection for stage IV cancer. With regard to rectal cancer, total mesorectal excision was performed in cases of low rectal cancer (0–8 cm above the anal verge) and anal canal cancer. Meanwhile, tumor-specific mesorectal excision was performed in cases where the tumor was confined to the upper rectum (8–12 cm above the anal verge).
Training program
Initially, novice surgeons are required to perform basic laparoscopic procedures such as cholecystectomy and act as endoscopists in LCRs. They are also encouraged to view a collection of video recordings of LCRs. Second, trainees are required to act as a primary surgeon in laparoscopic sigmoid colectomy and ileocecal resection, followed by laparoscopic hemicolectomy (both sides) and transverse colectomy. Laparoscopic surgery for rectal cancer is the last procedure that trainees perform. This program offers trainees sufficient experience and enables stepwise acquisition of laparoscopic skills.
Our program used a few principles to maintain the quality of LCRs operated on by trainees: (1) The primary surgeon was selected by an expert surgeon, considering each trainee's skill and the technical difficulty associated with patient-related factors. (2) An expert served as an assistant to retract the colorectum and its mesentery for organizing good operative field and to push the small bowel away from the operative field. (3) Trainees were uniformly required to use the standardized techniques to achieve mobilization of the colon and rectum, proximal ligation and division of the feeding artery, and transection and reconstruction of the colon and rectum. (4) Trainees were not given any essential advice to learn procedural or anatomical details intraoperatively. The expert did not perform any part of a trainee's procedure until assuming the position of primary surgeon, which was carried out when trainees were stuck with technical difficulties, developed inadequate dissection plane, or caused inadvertent bleeding.
Statistical analysis
Differences in clinicopathological characteristics and operative outcomes between the E group and the T group were analyzed according to the intention-to-treat principle. Comparison of the categorical variables was performed using Fisher's exact tests or chi-squared tests where appropriate. Continuous variables were presented in median values with interquartile ranges. Comparisons were performed using the Mann–Whitney U test. Relapse-free survival (RFS) and overall survival (OS) was analyzed. All time-to-event end points were plotted by the Kaplan–Meier method, and the significance was then determined using the log-rank test. Multivariate analysis was performed for RFS and OS in stage II/III disease to determine the hazard ratio (HR) and independence of prognostic impact by the Cox regression model in the backward stepwise method using variables with P<.10. All analyses was performed using Statistical Package for Social Sciences™ (SPSS) version 15.0 software (SPSS Inc., Chicago, IL), and significance was defined as P<.05.
Results
Among 456 consecutive laparoscopic resections for colorectal cancer between 2006 and 2010, the expert performed 143 (31.4%) cases, and trainees performed 313 (68.6%) cases. The patients and tumor characteristics are described in Table 1. The median age was lower (67.0 versus 71.0 years; P=.007), and the incidence of rectal cancer (37.8% versus 12.5%; P<.001) and sphincter-preserving procedures for rectal cancer (high anterior resection and low anterior resection, 85.2% versus 59.0%; P=.004) were higher, in the E group than in the T group. Carcinoembryonic antigen (CEA) level, carbohydrate antigen 19–9 level, and nodal involvement were the same between the two groups, whereas tumor diameter was larger (mean, 4.2 versus 3.7 cm; P=.005) and the incidence of T2–T4 tumors (79.7% versus 68.7%; P=.02) and stage II/III tumors (58.7% versus 45.4%; P=.008) were significantly higher in the E group than in the T group.
APR, abdominoperineal resection; CA 19–9, carbohydrate antigen 19–9; CEA, carcinoembryonic antigen; HAR, high anterior resection; IQR, interquartile range; ISR, internal sphincteric resection; LAR, low anterior resection.
Operative outcomes, postoperative complications, and recovery times are given in Table 2. Trainees completed the procedure by themselves in 297 cases (94.9%), whereas they were replaced by the expert intraoperatively in the remaining 16 cases (5.1%). Operative time (253 versus 245 minutes; P=.01) and time to resume diet (median, 3.2 versus 2.6 days) were longer in the E group than in the T group. Postoperative complications were observed with a similar incidence in the two groups (8.4% versus 9.9%). Hospital death occurred in 2 patients treated by the T group: 1 stage II patient died of duodenal peptic ulcer perforation complicated with liver cirrhosis, and another stage IV patient died of bleeding after liver metastasectomy.
APR, abdominoperineal resection; IQR, interquartile range.
Oncologic outcomes are summarized in Table 3. The incidence of the retrieval of less than 12 lymph nodes was similar between the two groups in each tumor stage. The incidence of postoperative chemotherapy in stage III patients was significantly different between the E group and the T group (83.0% versus 56.1%; P=.002). The median follow-up period was 35 (interquartile range, 3–73) months. The 3-year RFS was similar between the E group and the T group in each stage (for stage 0, 100% in both groups; for stage I, 94.2% versus 98.8% [P=.14]; for stage II, 94.3% versus 87.4% [P=.22]; and for stage III, 73.7% versus 76.9% [P=.84]) (Fig. 1). However, the 3-year OS for stage II was higher for the E group than for the T group (96.9% versus 87.0%; P=.03). The 3-year OS for stage 0 (100% in both groups), stage I (100% versus 93.3%; P=.22), stage III (91.3% versus 75.9%; P=.15), and stage IV (46.8% versus 30.7%; P=.61) were similar between the E group and the T group (Fig. 2).
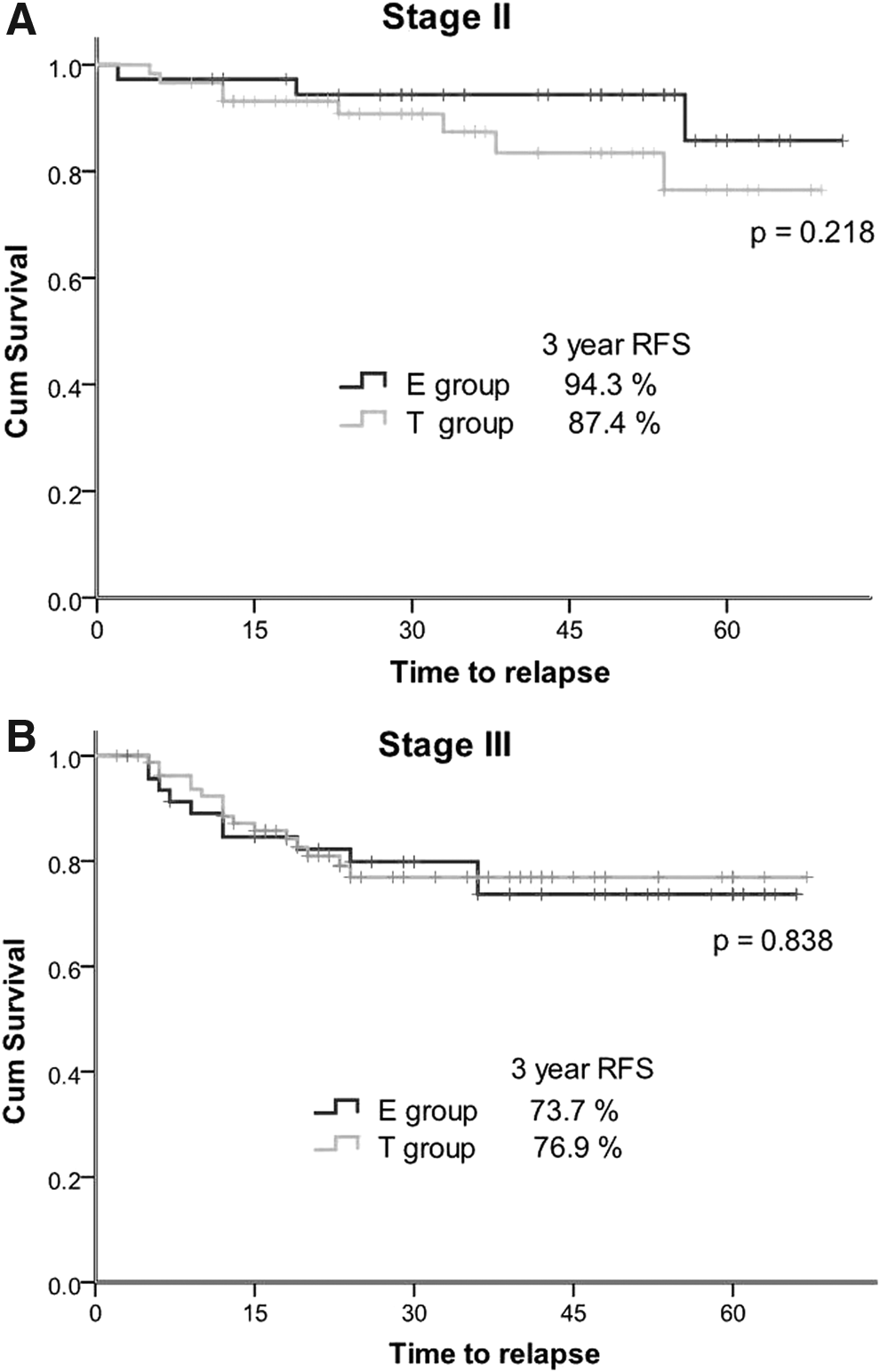
Comparison of relapse-free survival (RFS) rates of patients with

Comparison of overall survival (OS) rates of patients with
LN, lymph node; R1, microscopic residual tumor; R2, macroscopic residual tumor.
Univariate analyses of factors affecting RFS and OS for stage II/III patients were performed using Cox regression model stratified by tumor stage (Table 4), and parameters with P<.10 in each univariate analysis were selected as independent variables for multivariate analyses. After univariate analyses, margin status, log CEA level, and operative time were selected as independent variables for multivariate analysis for RFS, which showed that positive resection margin (R1 versus R0: HR, 9.017; P=.04) and higher log CEA level (HR, 1.560; P=.002) were significantly associated with lower RFS (Table 5). The 3-year RFS, adjusted for these significant parameters, was 92.0% for stage II patients and 77.4% for stage III patients. After univariate analysis, age, margin status, postoperative chemotherapy, log CEA level, intraoperative surgeon exchange, primary surgeon, tumor location, operative time, and postoperative complications were selected as independent variables for multivariate analysis for OS, which showed that increasing age (HR, 1.045; P=.04), positive resection margin (R1 versus R0: HR, 12.821; P=.02), higher log CEA level (HR, 1.521; P=.01), intraoperative surgeon exchange (HR, 3.477; P=.04), tumor location (rectum versus colon: HR, 2.537; P=.02), and postoperative complications (HR, 2.702; P=.04) were significant predictors of worse OS. Furthermore, postoperative chemotherapy (HR, 0.215; P=.009) and longer operative time (HR, 0.993; P=.01) were significant predictors of better OS (Table 5). The primary surgeon did not correlate with RFS. The primary surgeon was associated with OS in the univariate analysis, but this did not remain significant after multivariate analysis.
CEA, carcinoembryonic antigen; LN, lymph node; R1, microscopic residual tumor; T group, trainee group.
CEA, carcinoembryonic antigen; OS, overall survival; R1, microscopic residual tumor; RFS, relapse-free survival.
The causes of death are summarized in Table 6. Overall, 1 of 10 stage II patients in the T group (10%), 3 of 6 stage III patients in the E group (50%), and 8 of 16 stage III patients (50%) in the T group died from the progression of colorectal cancer.
Data are number of patients.
Discussion
The current study showed that laparoscopic operations undertaken by trainees did not negatively affect short-term outcomes, and, furthermore, they were not associated with impaired mid-term oncologic outcomes. The OS of stage II patients was lower for the T group than for the E group, although RFS was not different between the two groups. The difference of OS for stage II patients was not maintained after multivariate analysis. This would suggest that any differences observed were not attributable to oncologic impairment by trainees. Indeed, of the 10 stage II patients who died from the T group, only 1 died of colorectal cancer, whereas 9 patients died of other diseases. RFS and OS for stage III patients were also similar between the groups. Our study demonstrates the safety and quality of laparoscopic colorectal cancer surgery undertaken by trainees in terms of oncologic outcomes. Furthermore, these findings support our belief that this complicated laparoscopic procedure can be introduced early into the initial training period of novice surgeons.
The differences in demographic characteristics between patients treated by the E group and the T group are explained by our policy of assigning trainees to easier cases. An explanation for the higher incidence of rectal cancer and sphincter-preserving procedures in the E group is that laparoscopic resection for rectal cancer, especially sphincter-preserving procedures, is more demanding than that for colon cancer, with subsequent disadvantages such as longer operative time8,20,21 and an increased incidence of positive surgical margins. 6 We have previously reported that greater tumor depth and diameter are associated with greater operative difficulty,16,17 and this accounts for the higher incidence of T2–T4 tumors and greater tumor diameter in the E group. Meanwhile, the differences of age and tumor stage are associated with the range of lymph node dissection. In the case of elderly patients and Tis/T1 or stage 0/I/IV tumors, main node dissection (D3 lymph node dissection) is often skipped, and then these cases are considered as suitable for trainees' operation.
Survival is the most important outcome to assess treatment success for malignant disease. In this study, we evaluated RFS as well as OS, as many patients were elderly, and death might be due to other diseases. We demonstrated that RFS was not different for each stage, but OS was worse for stage II in the T group. Multivariate analysis revealed this difference was not due to the primary surgeon but due to other factors. Significant factors in our multivariate analyses for stage II/III OS such as age, margin status, postoperative chemotherapy, log CEA level, tumor location, and postoperative complications have been commonly reported.22–24 The presence of postoperative complications and anastomotic leakage affects the survival.25–27 This study found a low incidence of complications in both the E group (8.4%) and the T group (9.4%) and only 1 case (0.7%) of anastomotic leakage in the E group, indicating excellent intraoperative performance by the trainees under supervision of the expert surgeon. Some studies report that conversion to open surgery is associated with poor outcome 6 and that a low incidence of conversion is important to generate the benefit of laparoscopic surgery.2,28 In our study, the incidence of conversion was low in both groups and not statistically difference (2.1% versus 2.9%). Furthermore, conversion to open surgery did not correlate with survival rates, which is contrary to the finding reported previously.2,6,28
In our study, a significant association was found between rectal cancer and worse OS, which is in accordance with the results of previous studies.6,29 Laparoscopic rectal cancer surgery has also been reported to require longer operative times.8,20,21 Therefore, the higher incidence of rectal cancer in the E group could explain the longer operative time in this group. Alternatively, this may also be explained by the trend toward higher incidence of simultaneous major resection of other organs in the E group. Furthermore, higher incidences of sphincter-preserving procedures in the E group may account for the prolonged time to resume a normal diet in patients treated by the E group, as these procedures are associated with a high risk for anastomotic leakage 30 and are often managed with longer periods of fasting after surgery for the purpose of anastomotic decompression.
The primary surgeon was replaced by the expert in 16 patients (5 patients each in stage II and III), in order to prevent surgeon-related adverse outcomes. Therefore, we were surprised to discover a significant relationship between intraoperative surgeon exchange and worse OS for stage II/III patients in the multivariate analysis (HR, 2.585; P=.04). On reviewing the follow-up data of these 16 patients, we identified 5 deaths, of which colorectal cancer caused only 1 death, which occurred 2 months after palliative resection for stage IV disease. The remaining 4 deaths were due to other causes (pneumonia and suicide in stage II and cardiac failure and abscondence secondary to dementia in stage III). Colorectal cancer recurred in a single stage III patient, who underwent liver metastasectomy 6 months after his first surgery and is alive and free of disease 21 months after the first surgery. Considering these findings, we propose that the relationship between intraoperative surgeon exchange and worse OS for stage II/III patients was due to an accidentally high incidence of deaths not associated with colorectal cancer or postoperative complications.
The more lymph nodes that are evaluated, the better the survival rate,31–33 and most practice organizations and consensus panels promote surgical evaluation of a minimum of 12 lymph nodes as acceptable staging of colorectal cancer.34–36 Patients in both groups underwent the retrieval of enough lymph nodes for adequate therapeutic effect and nodal staging (mean, 23.5 in the E group and 20.6 in the T group). The incidence of the retrieval of less than 12 lymph nodes was not different between the E group and the T group and was especially low in stage II cancers (10.8% versus 15.0%) and in stage III cancers (10.6% versus 11.0%).
In the current laparoscopic era, surgical education has been also changing. It has been generally assumed that surgical training for advanced laparoscopic procedures will take longer than conventional surgery, because of the steep learning curve, and that it should be started after completion of open surgical training. However, nowadays, most colorectal procedures are performed using the laparoscopic approach, and novice surgeons may have little open experience before they start laparoscopic training. Our study not only demonstrates the safety and quality of laparoscopic colorectal cancer surgery undertaken by trainees but also supports the concept that laparoscopic colorectal cancer surgery, one of the more complicated laparoscopic procedures, can be safely introduced during the early initial training period of novice surgeons and would warrant an aggressive training program for advanced laparoscopic procedure.
There are several limitations to consider. First, the possible effect of biases in the selection of patients for operation by trainees may influence the findings of this study. Admittedly, if we aim to compare the outcomes after the procedure performed by the expert and trainees and decide which is better, a randomized control study may be desirable. However, we believe that the careful selection of patients for operation by trainees is essential and warranted to maintain its safety and quality. Instead, we used multivariate analyses to eradicate effects of differences of patient demographics between the two groups. Furthermore, we wanted to evaluate the safety and quality of trainees' operations in order to support and disseminate aggressive education; we did not wish to compare the skill of trainees directly with that of the expert. For this purpose, this cohort study is meaningful because it revealed favorable short- and mid-term outcomes after laparoscopic colorectal cancer surgery undertaken by trainees. Another limitation is the small sample size of this study, which evaluated cases in a single institution. With the increasing use of laparoscopic approaches for the treatment of colorectal cancer worldwide, it is expected that more data from large-volume teaching centers or population studies will give more information on the impact of survival with aggressive education.
In summary, our study showed that laparoscopic operations undertaken by trainees did not negatively affect short-term outcomes and were not associated with impaired mid-term oncologic outcomes. Our findings support early initiation of training in laparoscopic surgery for the treatment of colorectal cancer.
Footnotes
Acknowledgments
The authors are grateful to Mrs. Juri Akai and Mrs. Junko Odahara for their help in data collection.
Disclosure Statement
No competing financial interests exist.
S.O., T.Y., and Y.S. were responsible for the study's conception and design. T.Y., Y.O., T.M., and H.H. were responsible for acquisition of data. S.O., M.F., and I.I. were responsible for analysis and interpretation of data. S.O., T.Y., T.M., and H.H. were responsible for drafting the article. Y.S., Y.O., M.F., and I.I. were responsible for revising the article. All of the authors gave final approval of the version to be published.