
Abstract
Abstract
Introduction:
Inguinal hernia repair is one of the most common operations performed by pediatric surgeons. Although the practice of sending the hernia sac for histologic examination after routine hernia repair is common, the indications and practice patterns for this have not been evaluated. The objective of this survey was to determine practice patterns and indications for histologic analysis of the pediatric inguinal hernia sac.
Materials and Methods:
A 9-question online survey was sent to all members of the International Pediatric Endosurgery Group (IPEG). A Kruskal–Wallis test was used to determine whether practice patterns of sending the hernia sac for histologic evaluation were associated with respondent characteristics. The chi-squared test with Yates's correction was used where appropriate.
Results:
The survey was completed by 315 IPEG members, for a response rate of 54.4%. Hernia sacs were sent for histologic evaluation always by 23.9%, often by 5.1%, rarely by 17.5%, and never by 53.5%. The respondent characteristics were not associated with whether or not specimens were sent for histology review. Of the 128 who reported sending the inguinal hernia sac, the most common reasons were hospital/state requirements (47.6%), followed by routine practice (25.7%) and concern for missed pathology (24.2%).
Conclusions:
The majority of IPEG respondents report never sending the inguinal hernia sac for histologic analysis. Of those that do, most are influenced by hospital/state requirements. The value of sending the hernia sac after routine inguinal hernia repair should be validated if it is to remain an institutional requirement.
Introduction
I
Materials and Methods
In October 2011 an online-based survey (Fig. 1) was sent to all members of the International Pediatric Endosurgery Group (IPEG). The survey addressed respondents' years of experience, details of surgical practice, management of excised inguinal hernia sacs, and opinions regarding histologic management. The survey was sent by e-mail to all current IPEG members. The anonymous responses were collected until February 2012. Replies were tabulated on a computer database. The Kruskal–Wallis test was used to evaluate for association between respondent surgical practice characteristics and practice patterns of sending the hernia sac for histologic evaluation. The chi-squared test with Yates's correction was used where appropriate.
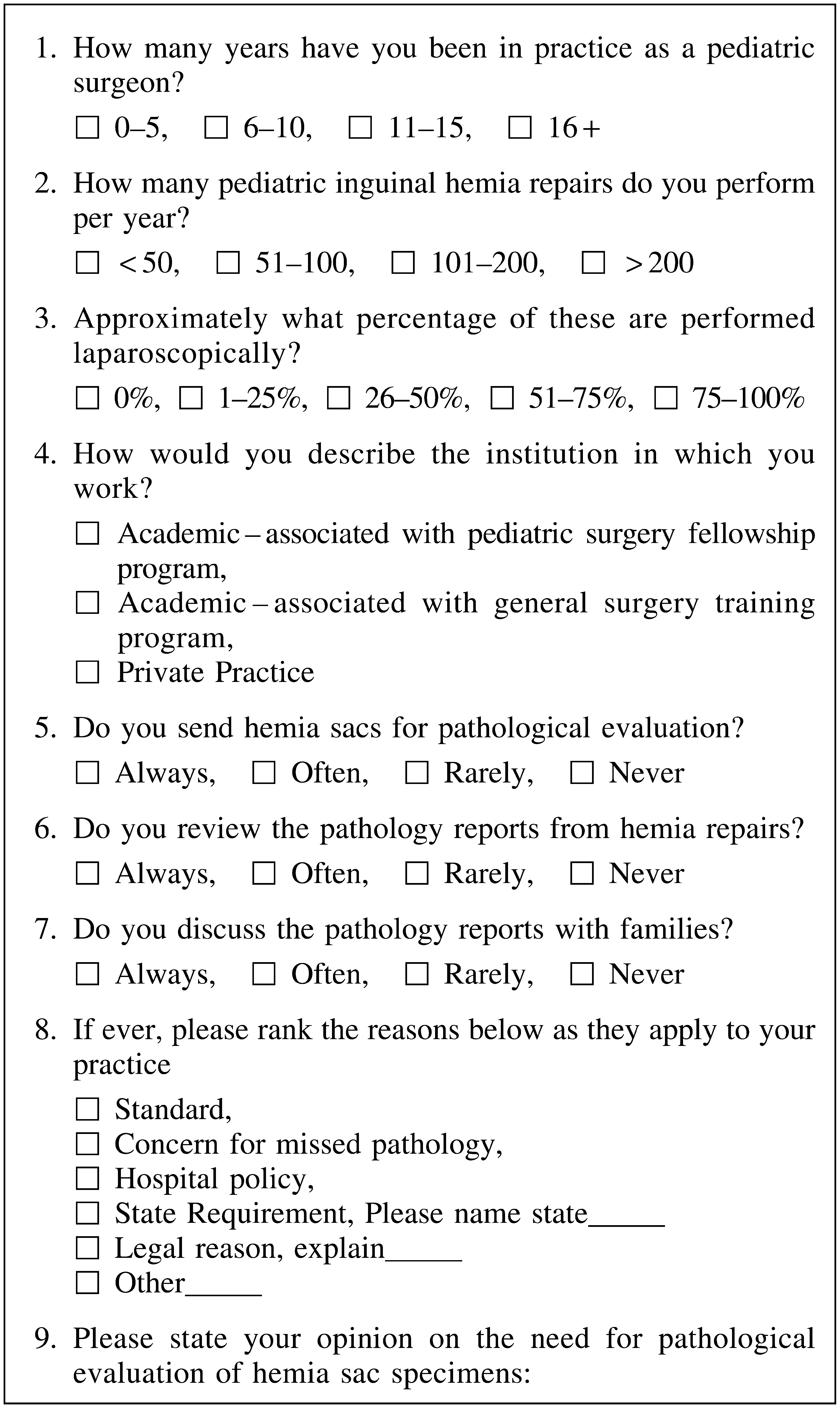
Questionnaire administered to International Pediatric Endosurgery Group members.
Results
The online survey was sent to 579 registered e-mail addresses, with responses received from 315 (54.4%) IPEG members. Characteristics of the respondents, including years of experience, surgical practice (number of repairs performed annually, percentage of hernia repairs performed laparoscopically), and institutional setting, are reported in Table 1.
Hernia sacs were sent for pathologic evaluation always (23.9% of respondents), often (5.1%), rarely (17.5%), and never (53.5%). The Kruskal–Wallis test demonstrated that there was no association with years of experience (P=.25), number of repairs performed annually (P=.13), percentage of hernia repairs performed laparoscopically (P=.13), or type of institution at which the surgeon was practicing (P=.06) when comparing whether or not the hernia sac was sent for histologic evaluation.
Of the 146 respondents who reported sending inguinal hernia sacs at any frequency, 128 provided specific reasons: 47.6% cited hospital/state requirements, 25.7% consider it routine practice, and 24.5% expressed a concern for missed pathology. Of the 75 respondents who reported always sending the hernia sac, 74 provided reasons, including 54.1% citing hospital/state requirement, 27% following standard practice since training, and 6.8% listing both as a primary reason; only 10.8% reported concern for missed pathology as the primary motivation for sending the hernia sacs for evaluation.
Of those respondents who ranked hospital/state requirement as their top motivating reason behind always sending specimens for pathology review, 61.9% do not believe it is necessary after routine repair, with an additional 19% qualifying that the specimen should be sent if there are any concerns at time of surgery.
Of 250 IPEG members providing a free response opinion, 61.6% do not believe that routine histologic evaluation of inguinal hernia sac is necessary. An additional 18.8% agree that routine histologic evaluation is not necessary and qualified that the hernia sac should only be sent if there is some concern for technical injury or gross abnormality noted at the time of surgery.
Of the 146 IPEG members who reported rarely, often, or always sending the hernia sac for histology review, 125 members provided a free response opinion. Of these members, 47.2% do not believe that routine histologic evaluation is necessary, with an additional 23.2% who qualified that the sac should only be sent if there is some concern at the time of surgery. Of these members, only 12 (9.6%) believe that the inguinal hernia sac should always be sent for histopathology review to evaluate and or document no injury to the vas deferens. Six respondents (4.8%) believe the inguinal hernia sac should always be sent as a matter of routine and quality assurance. Eight members (5.4%) believe that the inguinal hernia sac should be sent for medicolegal purposes—comments included need for documentation of sac excision, documentation of no injury to the vas, and aid in potential litigation.
Of the 31 surgeons who perform greater than 50% of their inguinal hernia repairs laparoscopically, 21 (67.7%) never and 1 (3.2%) always send the hernia sac for pathology review. Of the 283 surgeons who perform less than 50% of their inguinal hernia repairs laparoscopically, 146 (51.6%) never and 136 (48.1%) always send the hernia sac for pathology review. When comparing these two groups, there is a significant difference (P=.003) in number of surgeons who always versus never send the sac for pathologic review.
Discussion
Our survey demonstrates that the majority opinion of IPEG members is that the inguinal hernia sac does not need to be routinely sent for histologic analysis, and such a procedure should be reserved for select cases, especially if there is a concern for injury or abnormal pathology. This majority opinion, however, is not reflected by the current practice trends.
Open repair of pediatric inguinal hernias is still the most common approach. A recent international survey of surgeons from 27 European countries carried out in 2012 reported that 17% of those surgeons prefer a laparoscopic approach. 10 Although only 9.9% of respondents to our survey perform the majority of their repairs laparoscopically, 44.7% of the surgeons surveyed report using this method in their practice. The lower incidence of sending the sac for pathology within this group of surgeons who perform the majority of their repairs laparoscopically is expected given that the various methods of laparoscopic repair do not involve resection of the inguinal hernia sac.11–13 The volume of inguinal hernia sacs sent for histologic review will decrease in the same proportion as the laparoscopic approach becomes more commonplace. This fact calls into question for the need of microscopic review. If the repair can be done without sac removal, then it seems antiquated to be sending the sac for evaluation when it is resected.
The need to document no injury to the vas deferens is frequently cited as a reason to send hernia sacs for pathology in our survey; however, the true incidence of iatrogenic injury in uncomplicated cases is extraordinarily low. The incidence that has been reported in the literature ranges from 0.05% to 1.6%.2,6,8,14 However, of those reported, not all can be claimed as incidentally found iatrogenic injury. In a retrospective review of 7924 inguinal hernia sac specimens, 4 (0.05%) documented vas deferens were reported on histologic review. 6 Of those abnormal specimens identified, both were consistent with the primary indication of surgery and final diagnosis—exploration of atrophic/absent testes. In another retrospective review of 1494 pediatric hernia sac specimens, 2 (0.13%) were found to have evidence for vas deferens histologically. Both of these specimens were associated with suspected injury at the time of surgery. 8 Another retrospective review of 456 specimens yielded 5 (1.1%) abnormal reports. All of these specimens had injury suspected at the time of operation as well. Another four specimens in this study were reported to have epididymis on histologic review; all four of these operations were not simple routine inguinal hernia repairs but included resection of a communicating hydrocele. 5 In a review 8 of 1414 specimens, 80 (5%) demonstrated additional pathology, including inflammation, embryonal remnants, adipose tissue, vas deferens, adrenal cortical rests, fibrosis, and mesothelial reactivity. The two specimens identified as vas deferens were suspected in the operating room. The remaining additional findings were of no clinical significance. When the above-noted reviews are combined, all identifications of reproductive structures on microscopic review were associated with noted concern for injury at the time of surgery or with additional procedures performed.
The above-stated studies demonstrate the poor utilization of resources for the practice of sending inguinal hernia sacs for histopathology, particularly because the information cannot be used in a clinically relevant way. In addition, there is a tremendous disconnect between histologic evaluation and injury to the vas deferens, which can also occur from tissue handling at the time of surgery with manipulation or compression of the vas deferens. 15 The vas can be divided and, once recognized, repaired, and the peritoneal sac is still sent separately.
Some of the respondents reported the need to send the hernia sac not for clinical benefit to the patient, but for proof of hernia for billing and for medicolegal reasons. Incidence of tubular embryonal remnants is estimated at about 1.5%. 2 An accessory ductal structure, or incomplete duplication of the vas deferens, can be misinterpreted as injured vas deferens.2,16 In a retrospective review of 1119 inguinal hernia sacs, 4 (0.49%) demonstrated epididymal tissue. At the time of surgery, a normal vas deferens and epididymis were identified and documented. It was not until re-examination of these specimens that histology was revealed to be consistent with accessory or incompletely developed ductal structures. 4 Misidentification of these structures, as further outlined by a case report describing bilateral inguinal hernia repair with histologic reporting of well-formed segments of vas deferens bilaterally, highlights the negative impact this can have. In this case, the patient was explored bilaterally and found to have intact vas deferens bilaterally, indicating that the initial pathology report was consistent with embryonic remnants or partial duplication bilaterally. 16
Concern for missed malignancies is also cited as a reason to send all tissue specimens for review. In a review of 800 inguinal hernias, three (0.4%) malignancies were found; however, each patient had previously known clinical history of the noted malignancy. 9 Reports of malignancy within inguinal hernia sacs in the pediatric population is exceedingly low. A case of extrarenal Wilm's tumor masquerading as inguinal mass has been reported. 17 Another case of mesothelioma has been reported in a 6-year-old boy. 18 However, both of these cases of identified malignancy were associated with grossly visible disease at the time of surgery and were not incidental findings on histology review.
The cost of evaluating inguinal hernia sacs varies across institutions and countries. Reported institutional costs range from $14 per specimen ($15,852 annually) in Pakistan to $138.50 per specimen ($54,970 annually) in the United States. Considering inguinal hernia repair is one of the most common pediatric specimens sent for pathology review, national costs are likely to be much more significant. A cost analysis of adult hernia sacs was estimated to provide annual savings of $18 million in the United States if routine evaluation was eliminated. 19 In the current climate of trying to contain healthcare costs, this is an example of poorly allocated healthcare resources.
Conclusions
The majority of IPEG respondents, including those who always send inguinal hernia sacs for histology review, do not believe it is necessary after routine inguinal hernia repair. The value of sending the inguinal hernia sac in the pediatric population needs to be validated if it is to remain a state or institutional requirement.
Footnotes
Disclosure Statement
No competing financial interests exist.