
Abstract
Abstract
Background:
We aimed to assess the long-term oncologic outcome of hand-assisted laparoscopic radical nephrectomy (HLRN) compared with open radical nephrectomy (ORN) in patients with clinically localized renal cell carcinoma (RCC).
Patients and Methods:
We retrospectively reviewed the data from 1098 patients who underwent radical nephrectomy at five institutions in Korea between 2000 and 2011 for clinically localized RCC. One hundred ninety-seven patients in the HLRN group were compared with 901 patients in the ORN group. Univariate and multivariate analysis assessed the effects of operative method on oncologic outcomes.
Results:
The median duration of follow-up was 69 months for the HLRN group and 63 months for the ORN group. No statistically significant difference was found in the operative time (170.2 minutes versus 168.9 minutes, P=.793) between the HLRN and ORN groups. However, estimated blood loss was significantly lower in the HLRN group than in the ORN group (245.9 mL versus 422.4 mL, P<.001). The pathological T stage was significantly higher in patients in the ORN group: 79.9% of patients in the HLRN group derived from pT1, versus 54.7% of those in the ORN group (P<.001). A statistically significant difference was found in the 5-year disease-free (90.6% versus 79.6%, P<.001), cancer-specific (95.7% versus 91.1%, P=.019), and overall (93.4% versus 85.4%, P<.001) survival between the HLRN and ORN groups. However, multivariate analysis by Cox's proportional hazards model does not retain surgical methods as an independent predictive factor for cancer-related death or recurrence.
Conclusions:
HLRN may be a preferable minimally invasive surgical treatment for clinically localized RCC with comparable long-term oncologic outcomes.
Introduction
L
Subjects and Methods
In total, 2152 patients with clinically localized RCC underwent radical nephrectomy between January 2000 and January 2011 as the primary treatment at five institutions in Korea. Among the patients with follow-up duration of over 6 months, 197 (17.9%) patients were treated with HLRN, and 901 (82.1%) were operated on with ORN. The decision to perform HLRN or ORN was made preoperatively according to the surgeon factors, patient factors, and tumor factors, possibly precluding a patient from a minimally invasive approach. After approval by the Institutional Review Board at Seoul National University Hospital, we reviewed the patient clinical data for gender, age, body mass index (BMI), medical history, Eastern Cooperative Oncology Group (ECOG) performance status, preoperative laboratory findings, conversion rate, operative time, transfusion rate, estimated blood loss, postoperative laboratory findings, pathologic outcomes, morbidity, and mortality. Operative morbidity and mortality were defined as occurring within 30 days after surgery, and operative morbidity was defined and classified according the Clavien–Dindo classification of surgical complications. 9 TNM staging was based on the 7th TNM classification of the Union Internationale Contre le Cancer and the American Joint Committee on Cancer guidelines. 10 Histological subtypes were classified according to the Union Internationale Contre le Cancer/American Joint Committee on Cancer and Heidelberg recommendations, 11 and tumor grades were determined according to the grading system of Fuhrman et al. 12 Follow-up status was evaluated using physical examinations, laboratory tests, chest X-ray, and abdominal computed tomography scans according to the surveillance protocols of each institution. The database of the National Cancer Registration Program of Korea was used to determine patient survival if the patient was lost to follow-up.
Statistical analysis was completed using IBM SPSS software (version 19.0; SPSS Inc., an IBM Company, Chicago, IL). Clinical and pathological variables were analyzed with Student's t test for continuous variables and the chi-squared test for categorical variables. Univariate and multivariate logistic regression analysis were used to evaluate variables associated with major complications (Clavien–Dindo classification 3 or higher). The disease-free, cancer-specific, and overall survival rates were estimated using the Kaplan–Meier method and compared using the log rank test. Prognostic factors for cancer recurrence and cancer-related death were assessed by the Cox proportional hazards regression model in a forward stepwise regression. All P values were two-sided, and P<.05 was considered significant.
Results
Analysis for baseline demographics and surgical outcomes
Characteristics of the patients are listed in Table 1. No significant differences were observed between the two groups regarding age, gender, and BMI. Those selected for HLRN had fewer symptoms at diagnosis (20.3% versus 32.1%, P=.001) and better ECOG performance status with 0 or 1 (74.6% versus 60.2%, P<.001).
BMI, body mass index; ECOG, Eastern Cooperative Oncology Group; HLRN, hand-assisted laparoscopic radical nephrectomy; ORN, open radical nephrectomy.
Surgical outcomes are shown in Table 2. Two patients in the HLRN group ended up being converted to open surgery; conversion was due to dense adhesions and bleeding as a result of previous abdominal surgery in 1 case and to severe bleeding from the inferior vena cava in the other. There was no significant difference in operative time (170.2 minutes versus 168.9 minutes, P=.793). Estimated blood loss and transfusion rate were significantly lower in the HLRN group than in the ORN group, and the percentage decrease in hemoglobin was not significantly different in both groups. Statistically significant differences between patients in both groups were observed in intraoperative and postoperative complications.
Hb, hemoglobin; HLRN, hand-assisted laparoscopic radical nephrectomy; ORN, open radical nephrectomy.
Analysis for intraoperative and postoperative complications
There were four intraoperative complications in 3 patients (1.5%) treated with HLRN and 116 in 104 patients (11.5%) treated with ORN (P<.001). One patient in the HLRN group experienced serosa tearing of the colon, which was managed conservatively, and 2 patients experienced bleeding from the spleen and inferior vena cava, requiring several units of blood transfusion and open conversion. Intraoperative complications of ORN were pleura tearing (n=51, 5.7%), pancreas injury (n=7, 0.8%), spleen injury (n=6, 0.7%), major vessel injury (n=6, 0.7%), colon injury (n=4, 0.4%), and other assorted problems.
There were 11 (5.1%) postoperative complications in the HLRN group and 120 (13.3%) in the ORN group, respectively. The distribution according to the Clavien–Dindo classification and type of complications are shown in Table 3. Complications of grade 3 or higher accounted for 27.3% in the HLRN group and 18.3% in the ORN group of all postoperative complications. On univariate analysis, BMI, mass size, operative time, and estimated blood loss were significantly associated with major complications, and multivariate logistic regression analysis retained BMI and estimated blood loss as independent predictive factors for major complications (Table 4).
BMI, body mass index; CI, confidence interval; HLRN, hand-assisted laparoscopic radical nephrectomy; HR, hazard ratio.
Analysis for pathologic and oncologic outcomes
Table 5 shows pathologic stage, histologic subtype, and Fuhrman's nuclear grade distribution. The pathologic T stage and Fuhrman's nuclear grade were significantly higher in patients in the ORN group. The median duration of postoperative follow-up was 69 months (range, 6–148 months) for the HLRN group and 63 months (range, 6–154 months) for the ORN group. Local recurrence or distant metastasis developed in 19 patients (9.6%) in the HLRN group and in 159 patients (17.6%) in the ORN group (P=.018). Thirteen patients (6.6%) in the HLRN group and 122 (13.5%) in the ORN group died during the follow-up period, which was not a statistically significant difference (P=.058). Figures 1 and 2 show the Kaplan–Meier curves for disease-free survival and cancer-specific survival, respectively. Statistically significant differences were observed in disease-free survival and cancer-specific survival between the HLRN and ORN groups. However, when the patients were stratified based on pathologic T stage, there were no significant differences in disease-free survival and cancer-specific survival between the two groups.
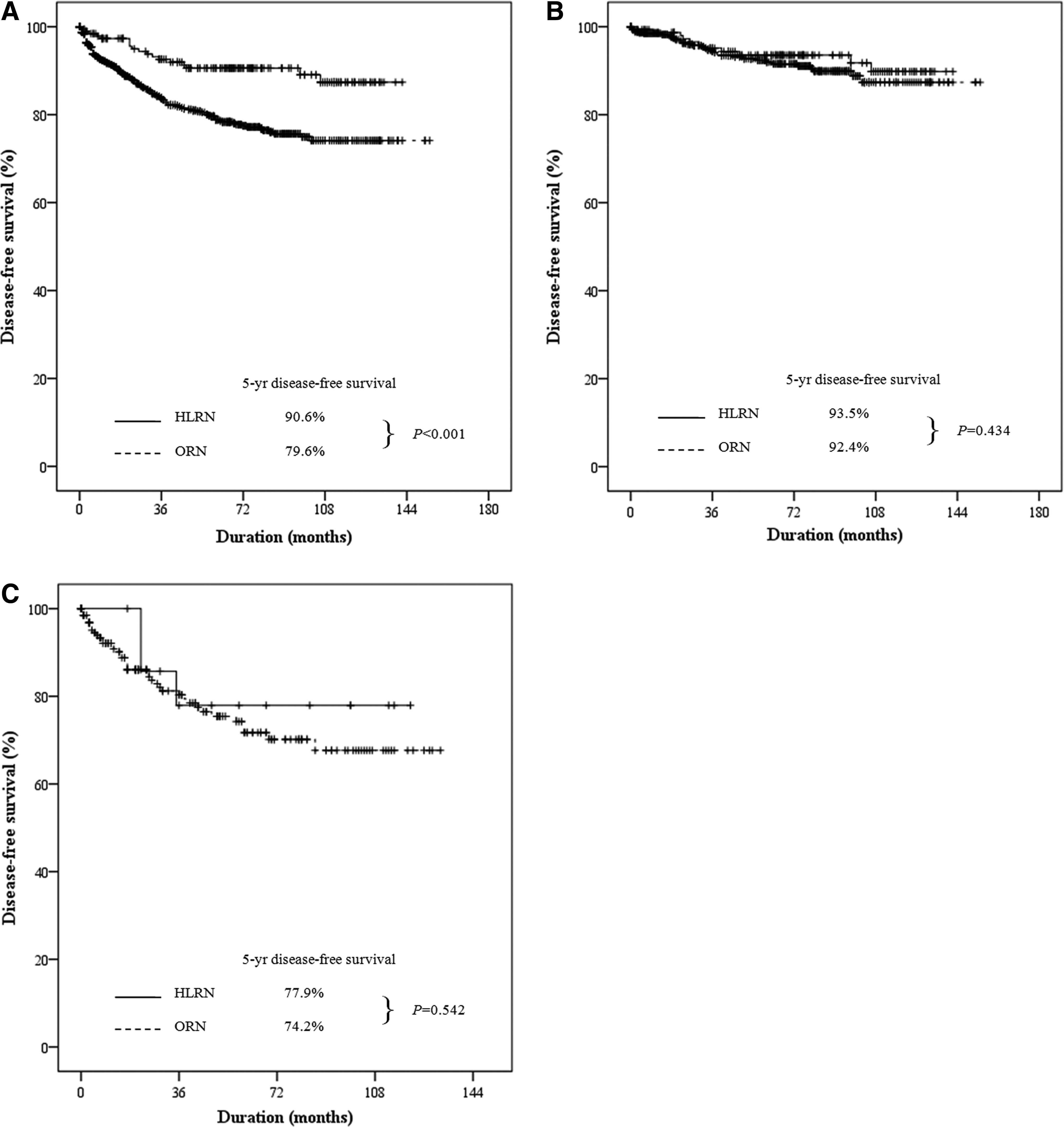
Disease-free survival according to the operative method, hand-assisted laparoscopic radical nephrectomy (HLRN) versus open radical nephrectomy (ORN):
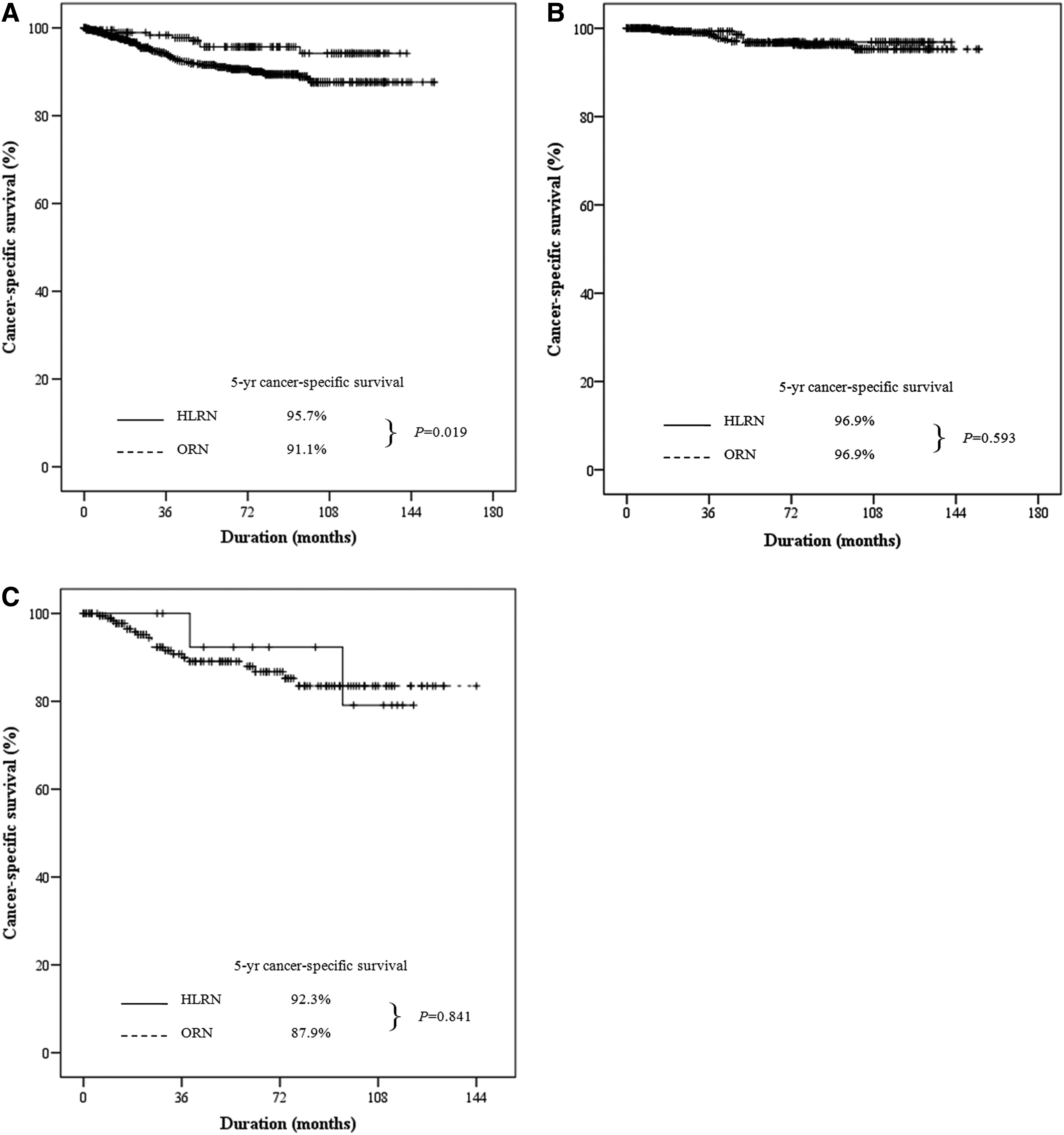
Cancer-specific survival according to the operative method, hand-assisted laparoscopic radical nephrectomy (HLRN) versus open radical nephrectomy (ORN):
Factors significantly influencing disease-free and cancer-specific survival are listed in Table 6. Pathologic T stage, Fuhrman's nuclear grade, and symptoms at diagnosis were statistically significant predictors of disease-free survival. Also, BMI, ECOG performance status, symptoms at diagnosis, and pathologic T stage were independent predictors of cancer-specific survival. The surgical method was not associated with the disease-free survival or cancer-specific survival.
BMI, body mass index; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HLRN, hand-assisted laparoscopic radical nephrectomy; HR, hazard ratio; ORN, open radical nephrectomy.
Discussion
Conventional laparoscopic radical nephrectomy has emerged as the standard of care for clinically localized RCC because of advantages including less blood loss, shorter hospital stay, and faster postoperative recovery, while oncologic outcomes remain comparable.1,7,13 On the other hand, nearly all comparative studies indicated that conventional laparoscopic radical nephrectomy required a significantly longer operative time and was associated with a steep learning curve.13–15 The technical difficulty of conventional laparoscopic radical nephrectomy poses particular challenges of relative lack of tactile sensation and depth perception, frustrating surgeons.
HLRN has been an established alternative to conventional laparoscopic radical nephrectomy for more than 10 years. 5 Compared with open surgery, HLRN provides the benefits of minimally invasive surgery. 16 Wadström et al. 16 reported the largest meta-analysis of hand-assisted laparoscopic renal surgery. In their study, for radical nephrectomy, estimated blood loss and length of stay were significantly less in the HLRN group compared with the ORN group with a statistically significant difference of −232.9 mL (95% confidence interval, −383.6, −82.2), and −2.4 days (95% confidence interval, −3.5, −1.3), respectively. Operative time was longer in the HLRN group with a mean difference of 42.3 minutes (95% confidence interval, 5.8, 78.7), and safety outcomes were not significantly different for these two groups. These findings are consistent with our previous study reporting that operative time was significantly longer (206.8 minutes versus 179.1 minutes, P<.001), and blood loss was significantly lower (311.6 mL versus 372.4 mL, P=.003) in the HLRN group than in the ORN group. 8
In the present study, overall perioperative complication rates were significantly higher in the ORN group (13.3%) than in the HLRN group (5.1%). However, in previous studies, including the meta-analysis, that compared surgical outcomes of HLRN and ORN, there was no statistically significant difference in safety outcomes for these two groups. 16 These discrepancies most likely result from selection bias contributing to the observed differences in rates of complications among institutions. However, many factors that could influence the complication rates were controlled in logistic regression analysis, and it is likely that the different safety outcomes of HLRN and ORN were an artifact of bias.
Survival analysis is of key importance, as it has rarely been studied in patients who underwent HLRN, and the present study showed no significant difference between HLRN and ORN in patients with the same pathologic T stage. Kawauchi et al. 17 evaluated the intermediate oncologic outcome of retroperitoneal HLRN using the data of 123 patients with a mean follow-up period of 41 months. There were no differences in 5-year disease-free survival and cancer-specific survival rate for the HLRN and ORN groups, at 92% and 91% (P=.9700) and 92% and 94% (P=.4295), respectively. Similarly, Bandi et al. 18 reported that of the 65 patients who had a follow-up greater than 36 months (mean, 46 months), 5-year disease-free and cancer-specific survival rates were 90.2% and 94.4%, respectively. To our knowledge, the present study included the largest number of patients who received HLRN with the longest follow-up duration to date.
In the present study, we evaluated the long-term oncologic outcomes of HLRN in 197 patients with a mean follow-up duration of 69 months. Although there are several biases in the present study, there might be no differences in the long-term oncologic efficacy between HLRN and ORN. When the patients were stratified based on pathologic T stage, 5-year disease-free survival and cancer-specific survival rates were not significantly different according to the surgical methods. These findings show that HLRN is able to maintain an excellent long-term oncologic outcome comparable to ORN.
There are several limitations of this study. First of all, it is a retrospective study, and selection bias by surgeons or patients as to which surgical procedure to perform on which patients cannot be completely controlled. Another potential limitation is that the standardization of surgical techniques or follow-up protocols was impossible because of the multi-institutional and retrospective design of the study. However, we tried to control for possible factors that could influence the results by multivariate analysis. Therefore, despite of the limitations of the study, HLRN is certainly comparable, or preferable, to ORN with regard to perioperative surgical outcomes and long-term oncologic outcomes.
In conclusion, the present study shows that HLRN may be a preferable minimally invasive surgical treatment for clinically localized RCC with comparable long-term oncologic outcomes. Although large-scale, multicenter, prospective, randomized trials comparing HLRN with ORN for localized RCC are clearly needed, we anticipate that the same excellent results will be reported.
Footnotes
Disclosure Statement
No competing financial interests exist.