
Abstract
Abstract
Objective:
To investigate the effects and technical points of laparoscopic splenectomy and esophagogastric devascularization (LS+ED) for portal hypertension (PH) due to liver cirrhosis.
Subjects and
Results:
LS+ED was successfully carried out on 188 patients. The mean duration of surgery was 232±59 minutes, the mean intraoperative blood loss was 189±137 mL, the rate of blood transfusion was 19.6% (40/204), and no deaths occurred during surgery. The mean postoperative interval to passing of flatus was 3.5±0.9 days, and the mean postoperative hospital stay was 8.7±2.2 days. Operative complications occurred in 100 patients, of whom 78 had portal vein system thrombosis (PVST). During a postoperative follow-up period of 2–65 months, 15 cases were lost to follow-up, esophagogastric variceal bleeding re-occurred in 7 patients, encephalopathy occurred in 2 patients, and secondary liver cancer occurred in 3 patients. Five patients died during this period.
Conclusions:
The technical points of LS+ED include a combined surgical approach, a reasonable surgical procedure, and an appropriate laparoscopic operating plane. LS+ED is a safe and effective treatment for minimal trauma and rapid recovery. PVST is a common and potentially life-threatening complication after LS+ED, and anticoagulation therapy should be given early.
Introduction
T
We used “laparoscopic splenectomy and esophagogastric devascularization,” “laparoscopic splenectomy and gastric devascularization,” “laparoscopic splenectomy and azygosportal disconnection,” or “laparoscopic splenectomy and pericardial devascularization” as the search terms to review the PubMed database. The beginning date for the search was January 1, 1990, and the ending date was February 28, 2013. In total, six relevant articles and 116 cases were retrieved. However, one of the articles dealt only with children and adolescents 8–17 years of age and therefore was not included in our analysis, whereas our study was focused on adults (18–75 years old). Therefore, finally only five articles were examined in our literature analysis, among which 110 cases were focused on laparoscopic surgery. In addition, there have been no consistent technical programs reported as references, and there has been no analysis of a large number of cases treated with LS+ED. This study retrospectively analyzed clinical data of 204 patients with PH due to cirrhosis who underwent LS+ED from January 2008 to April 2013 in Southwest Hospital of the Third Military Medical University, Chongqing, China. We discuss the surgical technique's highlights and clinical efficacy.
Subjects and Methods
Clinical data
From January 2008 to April 2013, LS+ED was performed on 204 patients with PH due to cirrhosis (161 men and 43 women). The mean age was 47 years (range, 20–73 years). There were 179 cases of hepatitis B virus–related cirrhosis, 10 cases of alcoholic cirrhosis, 6 cases of hepatitis C virus–related cirrhosis, 5 cases of autoimmune cirrhosis, and 4 cases of idiopathic cirrhosis. The numbers of patients who received LS+ED in 2008–2012 were 3, 12, 26, 39, and 79, respectively. The operative indications were as follows: (1) repeated EGVB history, ineffective results with conservative treatment, endoscopic variceal ligation or sclerotherapy, and radiological interventional treatment; (2) severe gastroesophageal varices (according to the endoscopic records and grading standard of esophageal varices by the Chinese Digestive Endoscopy Society 3 in Kunming on March 1, 2000); (3) ultrasound or computed tomography scan confirming cirrhosis with PH, splenomegaly, splenic hilum, and gastroesophageal varices; (4) hypersplenism and severe thrombocytopenia and/or leukopenia (white blood cell count of <2.0×109/L, platelet count of <30×109/L); and (5) 18–80 years of age, liver function in Child–Pugh A or B class, general condition and important organ functions satisfying the need for surgery, and tolerating CO2 pneumoperitoneum. The exclusion criteria included combination with liver cancer, thrombosis already existing in the portal vein system before the operation, and acute bleeding with emergency surgery. However, there were no limitations on the size of the spleen. Patients and their families were told about the surgical procedures and risks. All participants provided written informed consent for surgery, and this study was approved by the Third Military Medical University ethics committee. All operations were performed by the same surgical team.
Operative method
All patients received general anesthesia with tracheal intubation, the establishment of CO2 pneumoperitoneum, and maintenance of 12–14 mm Hg (1 mm Hg=0.133 kPa) intraabdominal pressure. LS+ED surgery was performed by placing the patient in a right lateral semidecubitus position and tilting the operating table slightly to the reverse Trendelenburg position. The surgeon operated from the right side of the operating table. Five operative ports were used, and the placement of the trocars was dependent on the volume of the spleen (Fig. 1). A comprehensive peritoneal and pelvic cavity exploration was performed by laparoscopy (1) to observe the liver, spleen, stomach, gallbladder, and other adjacent organs and (2) to focus on understanding the spleen size and the surrounding adhesions, accessory spleen, splenic hilum and gastroesophageal variceal degree, liver cirrhotic degree, ascites trait, and volume.
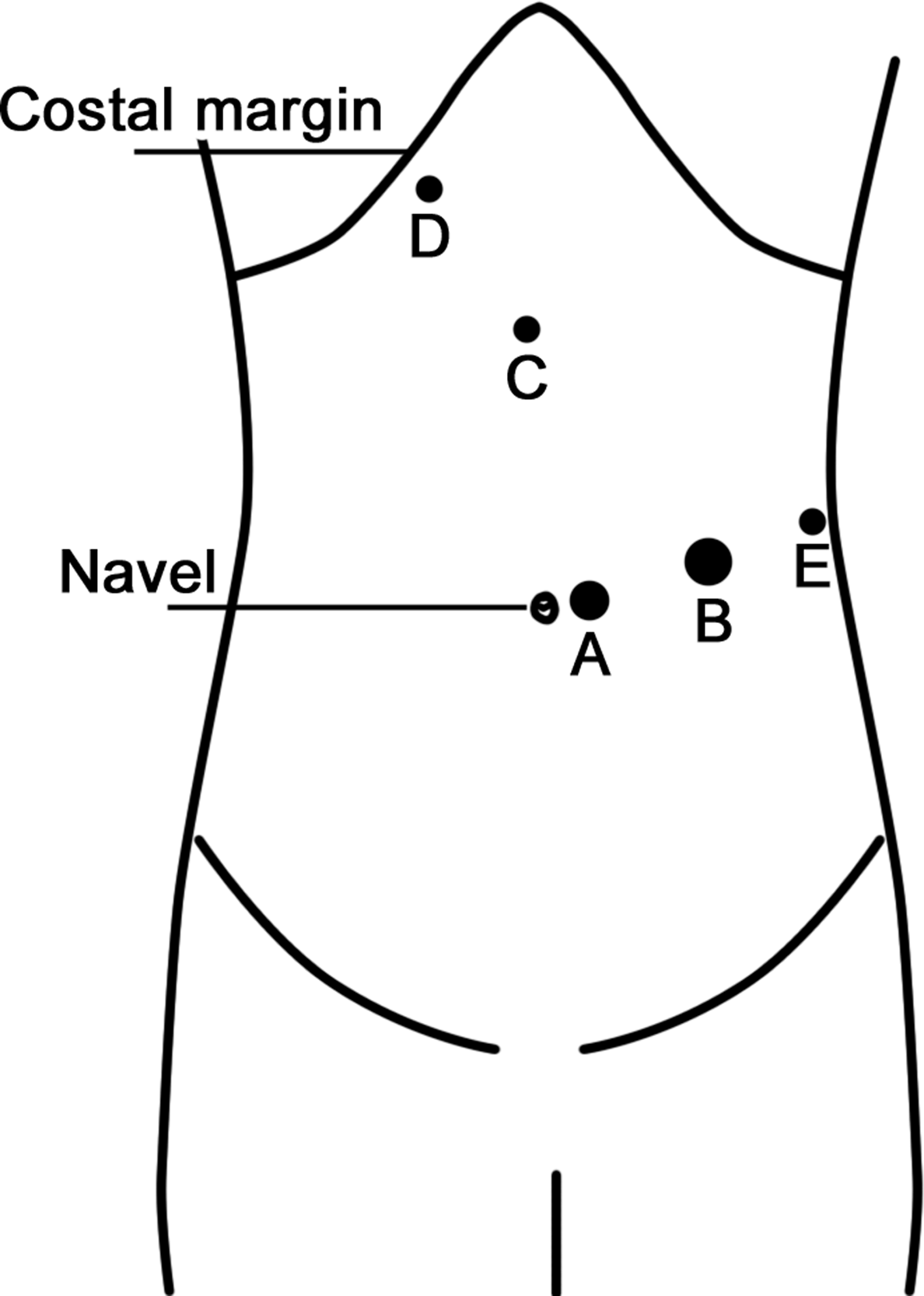
Trocar placement for laparoscopic splenectomy and esophagogastric devascularization. For trocar A, a 10-mm trocar was placed beside the umbilicus for establishing pneumoperitoneum and introducing a 10-mm 30° scope. For trocar B, a 12-mm trocar was placed in the left midclavicular line just below the border of the spleen for passing an endolinear cutter or Harmonic scalpel (main operating hole). For trocar C, a 5-mm trocar was placed in the medioventral line halfway between the xiphoid and the umbilicus. For trocar D, a 5-mm trocar was placed in the right midclavicular line subcostal space. For trocar E, a 5-mm trocar was placed in the left anterior auxiliary line halfway between the costal margin and the iliac crest (below the border of the spleen). Trocars C, D, and E were for the retractor, the grasper, and other supplementary instruments. The spleen was placed in a specimen bag, morcelated, and then extracted through trocar B. An abdominal drainage tube was placed in the splenic fossa and then extracted through trocar E.
The procedure began with division of the splenocolic attachments and gastrocolic ligament for entrance to the lesser sac. Whenever possible, the splenic artery was dissected and tied at the upper border of the pancreas. The splenogastric ligament (including short gastric vessels) and the splenorenal ligament were divided with a Harmonic® scalpel (Ethicon Endo-Surgery, Cincinnati, OH). The splenic hilum was dissected cautiously, and the splenic artery and vein were transected en bloc with the application of an Endo linear cutter (Ethicon Endo-Surgery) or an Endo GIA™ (Covidien, Mansfield, MA) surgical stapler. The remaining splenodiaphragmatic attachments were divided with a Harmonic scalpel, completing the splenectomy. The spleen was placed in a large specimen bag, morcelated, and then extracted through trocar B, followed by exact hemostasis in the spleen bed and peritoneal washing. Meanwhile, esophagogastric devascularization proceeded, and the patient was turned to the supine position. Starting at the middle of the greater curvature of the stomach, devascularization was performed in an inferior-to-superior manner between the gastric serosa and dilated veins with the use of a Harmonic scalpel. The main branch of the stomach coronary vein (including the stomach branches, esophageal branches, and the high esophageal branches) was found and divided with a Hem-o-lok® clip (Weck Surgical Instruments, Teleflex Medical, Durham, NC) and Harmonic scalpel at the side of the lesser curvature of the stomach. Additionally, the esophagus was pulled downward, and vessels were divided superior to a point about 7 cm away from the gastric fundus. Finally, a rubber tube was placed in the splenic fossa as an informative drain, which was then extracted through trocar E. The fascia was closed at each trocar site 10 mm or larger.
Therapeutic effects and follow-up results
Clinical data, including duration of surgery, intraoperative blood loss and the rate of transfusion, postoperative passing of flatus and hospital stay, operative complications, and the incidence and severity of portal vein system thrombosis (PVST), were analyzed. All patients were followed up by telephone or clinical service, and the follow-up results were collected by one specially assigned person.
Results
Literature review
In April 1998, Hashizume et al. 4 reported 10 patients who had undergone laparoscopic splenectomy combiend with pericardial devascularization. In March 2007, Hong et al. 5 reported 23 cases. In February 2008, Wang et al. 6 reported 25 cases. In July 2009, Jiang et al. 7 reported 28 cases in their controlled study. In February 2013, Zheng et al. 8 reported 24 cases in their controlled study. Therefore, in total, 110 cases were retrieved (Table 1).
Data are mean±standard deviation or median (range) values as indicated.
EGVB, esophagogastric variceal bleeding; NM, not mentioned; PVST, portal vein system thrombosis.
Operative results
Total LS+ED was successfully implemented in 188 of 204 cases. Sixteen cases were converted to laparotomy (the rate of conversion to laparotomy was 7.8%) because of severe inflammation or dense adhesion around the spleen hindering separation in 7 cases and uncontrollable bleeding of the surgical site in 9 cases. All 16 patients were included in this study. The mean duration of surgery was 232±59 minutes, the mean intraoperative blood loss was 189±137 mL, the rate of blood transfusion was 19.6% (40/204), and no operative deaths occurred. The mean postoperative passing of flatus was 3.5±0.9 days, and the mean postoperative hospital stay was 8.7±2.2 days.
Perioperative complications
No perioperative deaths occurred in the group with laparoscopic surgery. There were 100 cases of postoperative complications during hospitalization, and the incidence rate was 49.0%. Among them, 78 cases had PVST (upper abdominal ultrasound and computed tomography scan confirmed). The incidence of PVST was 38.2% (78/204), and PVST accounted for 78% of the postoperative complications (78/100). In accordance with PVST Yerdel classifications, 9 73 cases were Grades I and II, 4 cases were Grade III, and 1 case was Grade IV. Twenty-six cases of branch mural thrombosis were successfully dissolved after energetic anticoagulant and thrombolytic therapy, and in the rest of the cases with thrombosis there was no further increase during the follow-up period. Platelet counts of 16 patients exceeded 1000×109/L within 2 weeks after the operation, and these patients gradually recovered with platelet filtration treatment.
In addition, other postoperative complications occurred in 22 patients: 1 patient had a temporary pancreatic fistula, 3 patients had pulmonary infections, 4 patients had intraabdominal bleeding, 5 patients had pleural effusion, 3 patients had EGVB for rapidly increased portal pressure due to postoperative PVST, 1 patient had an internal jugular vein thrombosis, and 5 patients had refractory ascites. Of all patients with postoperative complications, in 1 patient, abdominal bloody drainage increased rapidly with ongoing declining hemoglobin level on Day 2 after the operation, and hemodynamic stability was difficult to maintain even with rehydration. We considered this to be intraabdominal active bleeding, and a second laparotomy surgery was immediately performed to confirm bleeding from the left subphrenic and lesser curvature veins, accurately stop the bleeding, and then provide dephlogisticate, hemostatic, and symptomatic treatment. Twenty-one patients were cured or improved by conservative treatment.
Follow-up results
All patients were followed up until June 2013, and the follow-up period was 2–65 months. Fifteen of the 204 patients (7.4%) were lost to the study. In 189 cases of the closely followed patients, EGVB re-occurred in 7 patients, encephalopathy occurred in 2 patients, and secondary liver cancer occurred in 3 patients. Five patients died, yielding a 2.5% mortality rate, including acute upper gastrointestinal re-bleeding in 2 patients, subarachnoid hemorrhage in 1 patient, secondary liver cancer in 1 patient, and an unknown cause of death in 1 patient.
Discussion
Many cirrhotic patients in China have PH due to chronic hepatitis B. Some patients have PH combined with recurrent upper gastrointestinal bleeding, which is life threatening. Most of the patients could not receive liver transplantation. As an effective treatment for EGVB and hypersplenism due to PH, splenectomy and esophagogastric devascularization have been implemented clinically for many years.
In recent years, advances in endoscopic technology provided a new treatment for such patients. The technical difficulties in LS+ED include the following: (1) The spleen is an organ for blood storage located in the deep part of the left upper peritoneal cavity. (2) PH causes swelling and congestion of the spleen, which makes it crisp and soft with high tension, so it can easily rupture with unmanageable bleeding. (3) Liver function is damaged because of anemia, hypoalbuminemia, thrombocytopenia, and coagulation disorders. (4) Varices in the splenic hilum and increasing and thickening of the perisplenic collateral vessels make it difficult to free and flip the spleen to expose and dissect the splenic hilum for total laparoscopic LS+ED. Small injuries in this domain most likely cause life-threatening bleeding. Therefore, laparotomy instruments should be routinely prepared with LS+ED in order for an exploratory laparotomy to be promptly and quickly performed when endoscopic uncontrollable bleeding occurs.
The technical highlights of LS+ED are as follows: (1) It includes a combined surgical approach (i.e., an anterior approach combined with a posterolateral approach). With an anterior approach, the splenic front can be clearly exposed in favor of handling the front vessels of the splenic pedicle. However, during freeing of the perisplenic ligament, it is difficult to flip the spleen in the ventromedial direction. In addition, splenomegaly or adhesions often affect vision because of poke holes located by the umbilicus. It is therefore difficult to reveal the spleen posterolaterally. With a posterolateral approach, a telescope can obtain a good viewing angle during freeing of the perisplenic ligament, especially with splenomegaly. In addition, the rear of the splenic hilum is primarily exposed by splenic gravity, which simplifies the main operation and decreases the risk of splenic bleeding. Moreover, gastrointestinal subdamage is reduced because the main operation occurs away from the stomach and intestine. It is more difficult to expose the splenic hilum front, and the accessory spleen is easier to be missed, with a posterolateral approach than with an anterior approach. A combined surgical approach is safer and more reliable. (2) Reasonable procedures are used (i.e., splenic artery ligation followed by splenic hilum dissection). Splenic artery ligation can shrink and soften the spleen, give more surgical space in favor of endoscopic surgical handling, and decrease the risk of intraoperative bleeding. Therefore, this is the key point whether or not LS+ED is completed successfully. For anatomic variations, it is difficult to search and dissect the splenic artery in about one-third of the patients, and dissection by force can injure splenic vessels and cause hemorrhea. At this time, nonanatomic splenic hilum splenectomy can be adopted, which separates and ligates the branch of the splenic artery near the splenic hilum, or suturing with 3-0 polypropylene (Prolene®; Ethicon Endo-Surgery) at the distribution of splenic artery can be performed. (3) There is an appropriate endoscopic operating plane with combined use of laparoscopic instruments, such as an ultrasonic scalpel and ligature and endoscopic linear cutter. (4) Operators have developed skillful techniques for liver, biliary, pancreatic, splenic, and laparoscopic surgeries. Preoperative imaging examinations and accurate assessments of varices are very important for LS+ED, although the operator's surgical skill level and degree of proficiency cannot be ignored regarding reduction of the numbers of conversions to laparotomy.
The laparoscopic technique generally has many advantages. For example, the three to five times magnified image makes vision clear, the converted perspective makes it easier to expose narrow spaces, the operative trauma and impact on the internal environment is less, and the operative incision is more esthetic than with laparotomy. With switchable perspectives and enlargeable views in laparoscopy, LS+ED can fully expose the splenopancreatic ligament, avoid intraoperative injury to the pancreas tail, decrease the rate of conversion to laparotomy, and reduce blood loss. Harmonic shears or LigaSure™ (Covidien) devices can fully occlude varicose blood vessels around the esophagus and gastric fundus, which avoids postoperative bleeding in open surgery due to ligature slipping. In addition, the removed spleen is placed in a specimen bag, morcelated, and then extracted through an operating hole. There is no incision in LS+ED, so it is minimally invasive and cosmetology is better. Our previous study 10 showed that there are better short-term effects of minor trauma, quicker recovery, and less complications in LS+ED, and the medium- or long-term effects of controlling EGVB, eliminating hypersplenism, and improving liver function were similar between the two surgical methods. In our institute, the numbers of patients with liver cirrhosis and PH who chose LS+ED in the most recent 5 years have increased year by year. (The numbers of patients in 2008–2012 were 3, 12, 26, 39, and 7, respectively, and 45 in March 1–4, 2013).
PVST was first described by Delatour in 1885 as reported by Ratner et al. 11 It is a common and potentially life-threatening complication of splenectomy.12,13 In serious cases, PSVT can significantly affect the patient's life expectancy. 14 Patients with PH who receive splenectomy have a higher incidence of PVST because portal vein pressure increases, blood flow may be in stasis, and this is combined with portal venous system vascular tortuosity and dilatation.15,16 The role of open splenectomy and esophagogastric devascularization or LS+ED in the development of PVST is not yet clear. However, a laparoscopic approach has been reported to influence the formation of PVST by the operative technique of the pneumoperitoneum and ligation of splenic hilar vessels. In the open surgery group, splenic hilar vessels were ligated conventionally, whereas these vessels were divided with an endoscopic vascular stapler in the laparoscopic surgery group.17,18 Kinjo et al. 19 showed that the incidence of PVST in cirrhotic patients with PH who received splenectomy was 24% (17/70). In our institute, it seems that the incidence of PVST in cirrhotic patients with PH who received LS+ED was 38.2% (78/204), but only 5 patients had severe PVST (Yerdel Grades III and IV). That is to say, most of the thromboses in the laparoscopic group were in the intrahepatic portal vein branch and/or the splenic vein stump. Three patients with severe PVST had re-occurring EGVB during hospitalization, and the bleeding stopped after conservative treatment. In the follow-up period, partial recanalization of thrombus was observed in 3 cases.
In conclusion, LS+ED for cirrhosis and PH results in minimal trauma, rapid recovery, and an esthetic incision and can yield satisfying medium- or long-term results. However, postoperative PVST should be noted as a possiblity. Platelets and coagulation function should be routinely monitored, and imaging examinations should be performed. Anticoagulation therapy should be given early. Reports on LS+ED have been mostly retrospective studies. Multicenter, clinical, prospective randomized studies with a greater number of cases are needed to confirm the long-term effects. In addition, the mechanism of postoperative PVST and an effective anticoagulation plan require further research and validation.
Footnotes
Disclosure Statement
No competing financial interests exist.