
Abstract
Abstract
Purpose:
The aim of the current study was to directly investigate whether active gas suction reduces intraperitoneal residual carbon dioxide and to analyze the effect of active gas suction on postoperative pain after laparoscopic cholecystectomy.
Subjects and Methods:
This prospective, randomized clinical study included patients between 19 and 65 years of age with gallbladder disease who were eligible for elective laparoscopic cholecystectomy. Patients were allocated into either the natural evacuation group (NE group) or the active suction group (AS group). In the AS group, active suction was applied by inserting the laparoscopic suction irrigation device through a 5-mm trocar for 60 seconds at the end of surgery. A chest X-ray was taken at postoperative Day 1, and the residual intraabdominal gas volume was measured. Perioperative data including pain score and analgesic requirement were collected.
Results:
Thirty-nine patients were allocated to the NE group, and 36 were allocated to the AS group. There was no statistically significant difference between the two groups in terms of demographic data and operative findings. However, a significant difference was observed in the residual intraperitoneal gas volume, with 15.9±6.8 mL in the NE group and 6.7±4.0 mL in the AS group (P<.001). Significant differences were also observed in the pain scores measured 6 hours after surgery, on postoperative Day 1, and on postoperative Day 2.
Conclusions:
Active gas suction is a very simple procedure that is safe and feasible. Performing this procedure significantly decreases the residual intraperitoneal gas volume and postoperative pain after laparoscopic surgery.
Introduction
L
A correlation was reported between residual intraperitoneal carbon dioxide and postoperative pain after laparoscopic surgery. 6 Based on these results, several authors have suggested a method of active gas suction.7–9 In these studies, the amount of residual intraperitoneal carbon dioxide after gas suction was not measured, and only the pain scores of the patients were compared. The aim of the current study was to directly investigate whether active gas suction reduces intraperitoneal residual carbon dioxide and to analyze the effect of active gas suction on postoperative pain.
Subjects and Methods
Study design
This prospective, randomized clinical study was approved by the institutional review board of our hospital before initiation of data collection (Institutional Review Board protocol number KC13EISI0451). Patient recruitment was begun on August 8, 2013, and was completed on November 7. Patients between 19 and 65 years of age with symptomatic cholelithiasis, chronic cholecystitis, gallbladder polyp, adenomyomatosis, or porcelain gallbladder who were eligible for LC were included in the study. Exclusion criteria were acute cholecystitis, a history of upper abdominal surgery, visible adhesions in the operating field due to perihepatitis, cases in which additional procedures such as endoscopic retrograde cholangiopancreatography were necessary postoperatively, and serious comorbidities such as coronary vessel disease or an immunosuppressed state.
The details of the study were explained to each patient, and written informed consent was obtained. Random number tables were used to allocate patients into either the natural evacuation (NE) group or the active suction (AS) group. The patients were blinded to the allocated group. The surgeon was also blinded to the allocated group until beginning the surgery. Data collection was performed by an independent research member with no knowledge of patient allocation. All operations were performed by two surgeons. Both surgeons had extensive LC experience, with more than 500 cases each.
In total, 83 patients were recruited. Forty-two patients were allocated to the NE group, and 41 were allocated to the AS group. After enrollment, 3 patients in the NE group and 5 patients in the AS group were eventually excluded. In the NE group, 2 patients were excluded because of findings of gallbladder empyema found intraoperatively, and 1 patient was excluded because of severe morbid obesity. In the AS group, 2 patients were excluded because of severe adhesions found in the perihepatic area intraoperatively, 1 patient was excluded because of findings of acute cholecystitis, 1 patient was excluded because of variant angina discovered postoperatively, and 1 patient was excluded because of unroofing of a hepatic cyst at the time of surgery. Thus 39 patients in the NE group and 36 patients in the AS group were included in analysis.
Surgical technique
The general anesthesia technique was identical in both groups. Premedication was not performed, and induction of general anesthesia was performed with intravenous fentanyl (0.15 mL/kg) and propofol (2.0–2.5 mg/kg). To facilitate orotracheal intubation, rocuronium (0.4–0.6 mg/kg) was given intravenously. Anesthesia was maintained with oxygen in air (1:1 by volume), remifentanyl (0.05–0.1 mg/kg), and sevoflurane (1–2%). Ventilation was controlled to maintain end-tidal pressure of CO2 at 4.5–5.5 kPa.
After general anesthesia, a vertical intraumbilical incision was made in the umbilicus. A 10-mm trocar was placed, and the abdomen was insufflated to 12 mm Hg. A second trocar was placed about 5 cm below the xiphoid process, and a third trocar was placed in the right anterior axillary line, at a level slightly above the umbilicus. The three-trocar method was routinely used. An additional trocar was used in cases with a difficult operating field, such as patients with a high body mass index. After a grasper was inserted in the third trocar, the infundibulum was grasped and retracted laterally and upward to expose Calot's triangle. The cystic duct and cystic artery were dissected, ligated using 5-mm clips, and divided using laparoscopic scissors. The gallbladder was then dissected off the liver bed in a retrograde fashion. The gallbladder was removed through the 10-mm intraumbilical incision using a vinyl bag.
The methods of gas evacuation after completion of cholecystectomy were as follows. In the NE group, the gas valves of all three trocars were left open until the abdomen was completely deflated and no more gas was heard or felt escaping the gas valves. In the AS group, active suction was applied by inserting the laparoscopic suction irrigation device (Surgiwand™; Covidien, Mansfield, MA) through a 5-mm trocar. To avoid organ damage or omental herniation, the trocar was pointed toward the subdiaphragmatic space. Continuous suction was applied for 60 seconds. In both groups, the trocar wounds were closed in the standard manner after gas evacuation.
Outcome measurement
Perioperative data, such as operation time, number of trocars, residual intraperitoneal gas volume, pain score, analgesic requirement, return to diet, postoperative hospital stay, postoperative nausea and vomiting (PONV), and postoperative complications, were collected. Analgesic requirement was measured by calculating the total amount of parenteral analgesics (intravenous tramadol) requested by the patient. The total residual intraabdominal gas volume was measured by the method described by Jackson et al. 6 A chest X-ray was taken on postoperative Day 1, and the gas volume was calculated using the formulas shown in Figure 1, under the assumption that the bubble formed part of a sphere.
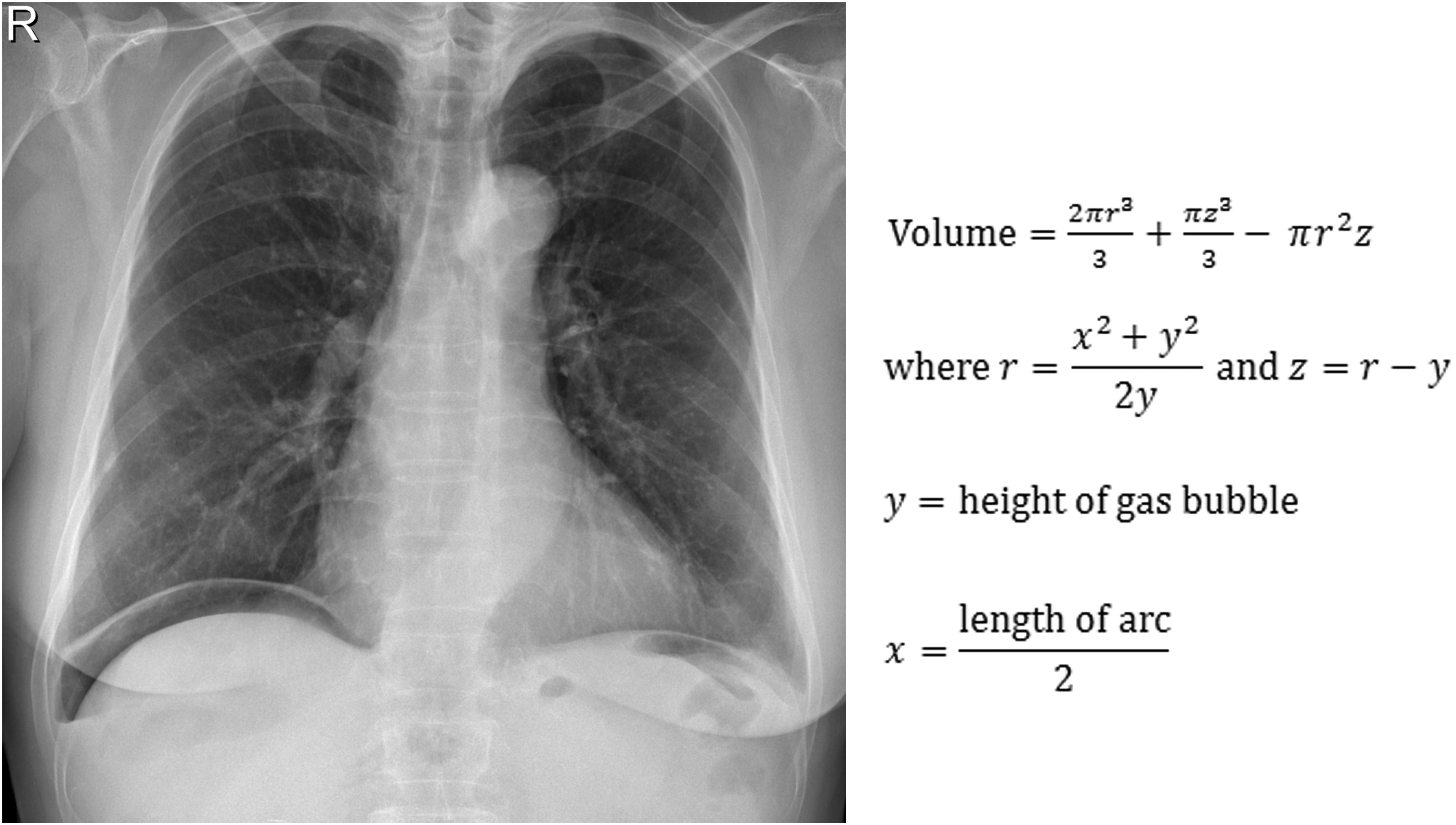
The gas volume was calculated using these formulas, under the assumption that the right subdiaphragmatic bubble formed part of a sphere.
A visual analog scale score of from 0 to 10 was used as the pain score, with 0 meaning “no pain” and 10 meaning “worst possible pain.” The pain score was measured three times: 6 hours after surgery, in the morning on postoperative Day 1, and in the morning on postoperative Day 2. PONV was assessed by the nursing staff on postoperative Day 1. If the patient had vomited or if the patient wanted anti-emetic medication, the patient was marked positive for PONV.
Statistical analysis
The collected data were analyzed using SPSS statistical package software (version 20.0 for Windows; SPSS, Inc., Chicago, IL). Continuous variables were compared using Student's t test. Categorical variables were compared with the chi-squared test or Fisher's exact test. All tests were two-sided, and a P value of≤.05 was regarded as significant.
Results
Eighty-three patients were enrolled, and 8 were excluded. In total, 75 patients were analyzed. Thirty-nine patients were allocated to the NE group, and 36 were allocated to the AS group. Patient demographics are shown in Table 1. There were no differences in age, gender, body mass index, or comorbidities.
Data are mean±standard deviation values unless indicated otherwise.
AS group, active suction group; NE, natural evacuation group.
Perioperative data are shown in Table 2. Average operation time was 16.5±8.4 minutes in the NE group and 15.6±6.7 minutes in the AS group, with no significant difference. All operations were completed using the three-trocar method except for 1 patient in the AS group, who needed an additional 5-mm trocar. A significant difference was observed in the residual intraperitoneal gas volume: 15.9±6.8 mL in the NE group and 6.7±4.0 mL in the AS group (P<.001). Significant differences were observed in the pain scores measured 6 hours after surgery, on postoperative Day 1, and on postoperative Day 2. The respective pain scores of the NE group and the AS group were 5.2±1.2 and 4.1±1.2 at 6 hours after surgery, 3.2±1.1 and 2.3±1.4 on postoperative Day 1, and 1.9±0.8 and 1.3±0.9 on postoperative Day 2. There was no difference in the amount of analgesic required: 43.6±16.9 mg in the NE group and 36.1±22.7 mg in the AS group. Return to diet was 1.0 day for the NE group and 1.0±0.2 days for the AS group, with no significant difference. Postoperative hospital stay was 2.0±0.2 days for both groups, with no significant difference. There were no significant complications in either group. Two patients (5.1%) in the NE group and 3 patients (8.3%) in the AS group were positive for PONV, which was not significantly different. All patients recovered completely within 3 days.
Data are mean±standard deviation values unless indicated otherwise.
AS group, active suction group; NE, natural evacuation group; PONV, postoperative nausea and vomiting.
The relationship between residual gas volume and pain score, both measured at postoperative Day 1, was analyzed (Fig. 2) and revealed a positive correlation with statistical significance (r=0.444, P<.001).

Correlation analysis between gas volume and pain score: r=0.444, P<.001.
Discussion
LC has become one of the most commonly performed operations in the field of general surgery. Although LC has many proven advantages over open surgery, pneumoperitoneum-related complications have been reported. Serious complications such as pneumothorax or gas embolism are rare10,11; however, shoulder pain, which is thought to result from stimulation of the phrenic nerve, is very common after laparoscopic surgery. 12 Various methods have been investigated with the aim of decreasing shoulder pain.4,5,7–9,12–14
One of the methods that has been studied is active gas suction. Jorgensen et al. 8 studied the effect of applying suction on the suprahepatic drain after LC and concluded that this procedure significantly reduced shoulder pain as reported by the patient. Jackson et al. 6 studied 20 patients who received gynecological laparoscopic surgery and reported that there was a correlation between residual intraperitoneal gas volume and pain score. Based on these findings, Atak et al. 7 investigated the effect of active gas suction after LC. After completion of cholecystectomy, a cannula was placed in the subdiaphragmatic space, and active suction was performed to decrease residual gas. The pain scores of the patients and the analgesic requirements were significantly decreased. Das et al. 9 performed a similar study and also reported decreased pain scores.
Pain scores are a subjective parameter. Because the amount of residual intraperitoneal air is an objective parameter, the present study was designed to directly investigate whether active suction decreases residual intraperitoneal gas, with the secondary aim of investigating whether active suction decreases pain score. No previous studies have investigated whether residual gas decreases after active suction.
The active suction procedure was very easy to perform. There were no special instruments required, and suction was applied for only 60 seconds. As a result of this procedure, the residual gas volume of the AS group decreased to less than half that of the NE group. The results of this study show that this procedure did not influence operation time or complication rates. Leaving a suprahepatic drain or placing a cannula in the subdiaphragmatic space to apply active suction may be unnecessary, as the results of this study show that using a laparoscopic suction–irrigation device is sufficient to decrease residual intraperitoneal gas. Moreover, pain scores were significantly decreased after this procedure. Correlation analysis showed that there was a correlation between gas volume and pain score, which is in line with previous findings in the literature. 6
In conclusion, active gas suction is a very simple procedure that is safe and feasible. Performing this procedure significantly decreases the residual intraperitoneal gas volume and postoperative pain after laparoscopic surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.