
Abstract
Abstract
Objectives:
We sought to identify preoperative patient and tumor characteristics that may be useful prognostic indicators of postsurgical outcome in patients undergoing laparoscopic adrenalectomy (LA).
Subjects and Methods:
Data from 92 patients who underwent 93 transabdominal LA procedures between 2006–2012 were retrieved. Patients were stratified based on estimated blood loss (EBL), length of stay (LOS), and perioperative complications. Interdependencies between surgical outcome and patient demographics, tumor characteristics, comorbidities, and Charlson Comorbidity Index (CCI) were statistically analyzed. The predictive capacity of each index was assessed using receiver operating characteristic curves.
Results:
Neither age, gender, tumor laterality, body mass index, American Society of Anesthesiologists (ASA) score, nor CCI predicted the occurrence of perioperative complications. EBL was significantly associated with increased age, tumor size, ASA score, and CCI, whereas prolonged LOS was associated with higher ASA score. Tumor size was related, although not significantly, to LOS and perioperative complications. Tumors ≥7.5 cm in diameter were significantly associated with worse perioperative outcomes.
Conclusions:
LA for adrenal lesions demonstrated reasonable complication rates and perioperative outcomes. Tumor size, CCI, and ASA score are predictive of increased EBL and LOS.
Introduction
T
Increased age and patient comorbidities, including obesity, tumor size, and malignancy, are all potential risk factors for inferior perioperative outcomes following laparoscopic surgery.9–12 As such, it is of interest to assess how these risk factors influence surgical outcomes following LA.
The purpose of the present study was to characterize the influence of each of these factors on perioperative outcomes in patients undergoing LA by examining a large single-center series.
Subjects and Methods
A retrospective analysis was performed using data collected from patients who underwent LA during a 6-year period (January 2006–February 2012). All patients received a standard metabolic workup, including determination of serum electrolytes, plasma metanephrines, adrenocorticotropic hormone, and 24-hour urine cortisol. An endocrinologist provided additional perioperative pharmacologic management for patients with metabolically active tumors. All adrenalectomies were performed using a previously described standardized transperitoneal laparoscopic approach. 13 The laparoscopic port-site placement preferred at our institution is illustrated in Figure 1.
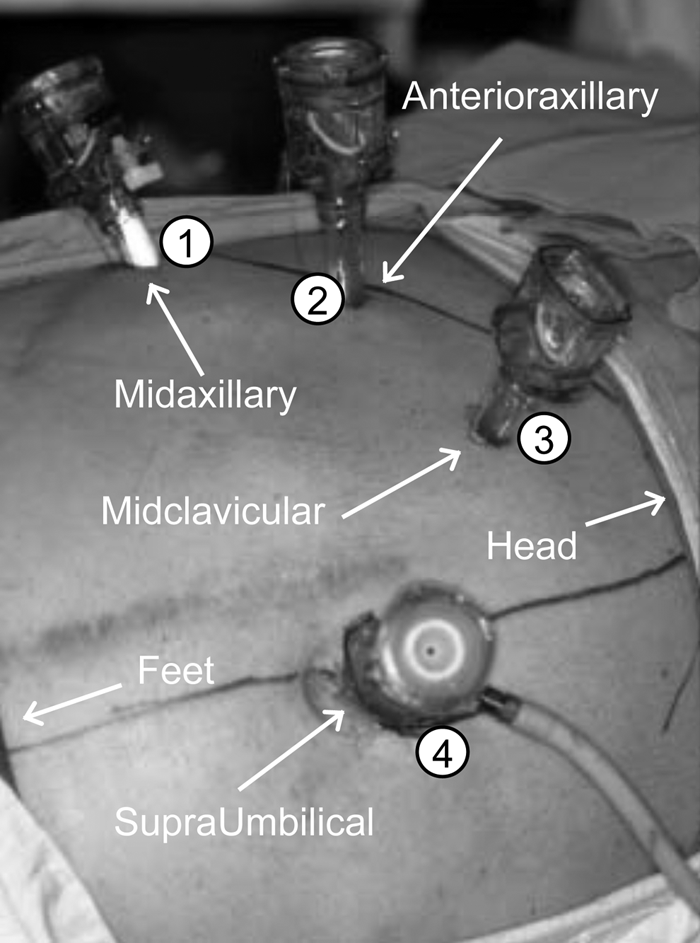
Laparoscopic port placement for right-sided adrenalectomy: (1) left-hand working port; (2) right-hand working port; (3) camera port; and (4) assistant retractor port.
Patient demographics (e.g., age, gender, body mass index [BMI]) and comorbidities (scored using the Charlson Comorbidity Index [CCI] and American Society of Anesthesiologists [ASA] score) were extracted from an institutional Institutional Review Board–approved database. Tumor laterality and size was determined from cross-sectional imaging studies. Data describing patient estimated blood loss (EBL), length of hospital stay (LOS), perioperative complications, and surgical margin status were dichotomized (EBL ≥200 mL versus EBL <200 mL, LOS ≥3 days versus LOS <3 days, and presence/absence of perioperative complications) and used as indices of perioperative outcome. Postoperative complications were graded according to the 2004 Clavien–Dindo grading system 14 (Table 1).
Where appropriate, patient demographics (age, gender, laterality, BMI, tumor size, ASA score, perioperative outcomes, and complications that occurred during surgery and within a 30-day postsurgical follow-up period) were compared using t tests, Mann–Whitney U tests, and chi-squared tests.
Receiver operating characteristic (ROC) analysis was used to assess the relationship between a continuous variable (tumor size) and perioperative outcomes. The highest diagnostic accuracy (i.e., the tumor size value with the highest sum of the true positive and true negative results over study group) or discriminative capacity of preoperative tumor size (to estimate the outcome condition of interest for the entire study group) was calculated. The continuous variables that significantly influenced perioperative outcome were incorporated into ROC analysis.
Statistical analyses were performed using SPSS version 17.0 software (SPSS, Inc., Chicago, IL).
Results
Patient demographics
The preoperative patient diagnoses are summarized in Table 2. Data were included from 93 consecutive LA procedures performed in 92 patients with a mean age of 52±13 years. Thirty-nine (42%) patients were male. Right-sided lesions accounted for 33 (35%) of the procedures. A single patient with an unresectable adrenal tumor was excluded from the analysis. In addition, 1 patient had metachronous bilateral adrenal lesions resected. Twenty-four patients had a history of prior abdominal surgery, most commonly cholecystectomies, appendectomies, and umbilical hernia repairs. Only 3 patients required lysis of adhesions during LA.
Twenty-two of 26 tumors were >4 cm. One was rapidly growing, two were suspicious for renal cell carcinoma metastasis, and one was suspicious for lung cancer metastasis.
One patient presented with clitoromegaly.
Clinical presentation, surgical indication, and histopathology data are detailed in Tables 2 and 3. Mean BMI was 31±7 kg/m2. Mean and median ASA scores were 1.5 and 1.0, respectively. Mean CCI was 3.1. The mean size of the adrenal tumors resected was 4±3 cm. Mean tumor sizes in males and females were 4±3 cm and 5±3 cm, respectively (P=.13), whereas the mean sizes of the right- and left-sided tumors were 5±3 cm and 4±3 cm, respectively (P=.5). Patient demographics were compared as a function of outcome group and are summarized in Table 4.
Data are mean±SD values or number of patients as indicated.
Statistically significant difference (P<.05).
ASA, American Society of Anesthesiologists; BMI, body mass index; CCI, Charlson Comorbidity Index; L, left; R, right.
Perioperative outcomes
There were, in total, 11 intraoperative and early postoperative (within 30 days) complications recorded within the patient cohort. Two patients (2/93; 2%) had major (Clavien grade ≥3) complications, and 3 patients (3/93; 3%) required a blood transfusion. There were three positive surgical margins (one pheochromocytoma, one adrenocortical carcinoma with invasion to the ipsilateral kidney requiring radical nephrectomy, and a single epithelioid angiosarcoma with invasion to the abdominal wall and adjacent musculature). Mean EBL was 109 mL (±232 mL; range, 5–1,300 mL). Mean postoperative LOS was 2.2 days (±2.2 days; range, 1–15 days). All patients with a positive surgical margin had an extended hospital stay (LOS ≥3 days). Two out of three of these patients had perioperative complications and an EBL of ≥200 mL. The incidence and description of each intraoperative and postoperative event are detailed in Table 5.
Although patient age was associated with EBL during surgery, there was no clear association with LOS or perioperative complications. Tumor size was positively correlated with EBL but not with either LOS or the incidence of perioperative complications. Although there was a trend for increasing tumor size to be associated with an increased incidence of perioperative complications and prolonged LOS, neither achieved statistical significance (P=.09 and P=.05, respectively). A greater proportion of patients with higher ASA status (ASA 3) exhibited a tendency toward EBL ≥200 mL and LOS ≥3 days. There was no significant association between ASA score and perioperative complications. CCI was significantly elevated in patients with EBL >200 mL. However, hospital LOS and perioperative complications were not significantly associated with CCI.
ROC curves were constructed to determine the association between perioperative outcomes and tumor size (Fig. 2). In patients who experienced perioperative complications, a tumor cutoff size of 7.5 cm had the highest predictive accuracy (Fig. 2A): positive predictive value, 26%; negative predictive value, 92%; sensitivity, 45%; specificity, 83%, with an accuracy of 78%; area under the ROC curve=0.6; 95% confidence interval, 0.4–0.8. When outcomes of EBL >200 mL and LOS >3 days were measured as a function of tumor size, a tumor cutoff size of 7.5 cm also exhibited the highest accuracy rate (Fig. 2B and C, respectively): positive predictive value, negative predictive value, sensitivity, and specificity of 58%, 93%, 54%, and 94%, respectively, with an accuracy rate of 88%, area under the ROC curve=0.8, 95% confidence interval, 0.7–0.9 for EBL >200 mL; and 42%, 85%, 42%, and 85%, respectively, with an accuracy rate of 76%, area under the ROC curve=0.6, 95% confidence interval, 0.5–0.8 for LOS.
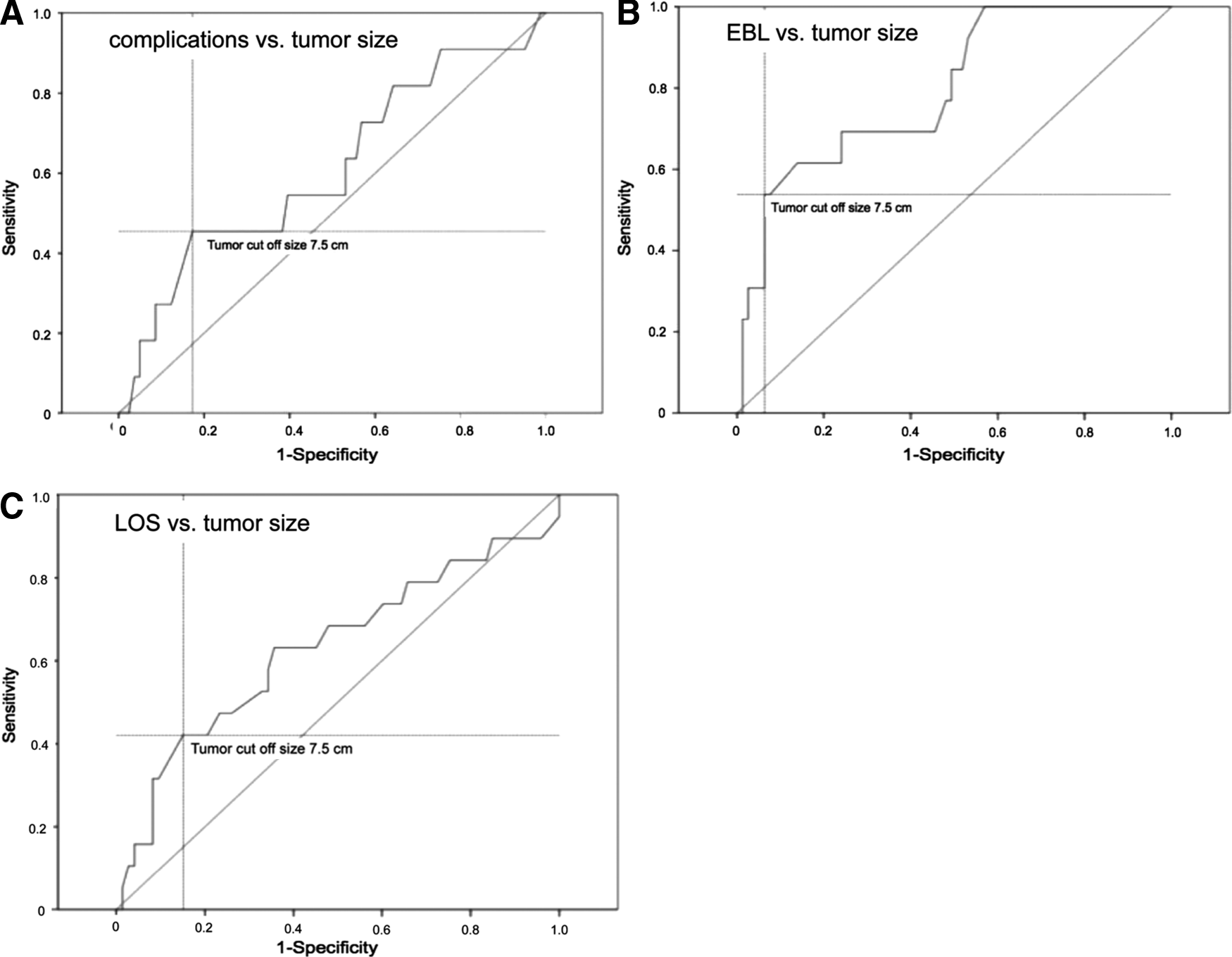
Receiver operating characteristic curves for
In patients with EBL ≥200 mL, 54 % of patients had tumors ≥7.5 cm. Similarly, 42% and 4% of patients who experienced prolonged LOS and perioperative complications had tumors ≥7.5 cm.
Discussion
We undertook a retrospective analysis of LA procedures performed at a single center to identify preoperative patient and tumor characteristics that are useful prognostic indicators of postsurgical outcomes. In the cohort of patients studied, greater tumor size, higher ASA score, and older age were all significantly associated with an increased EBL. Higher ASA scores were also associated with longer LOS. However, neither gender, BMI, nor tumor laterality was associated with increased EBL, and higher BMI values were not predictive of adverse perioperative outcomes or complications. Patients who experienced higher blood loss also exhibited higher CCI scores.
Surgery for adrenal tumors can be performed using various surgical approaches. Minimally invasive techniques have been associated with decreased postoperative pain as evidenced by decreased narcotic requirement, shorter hospital stays, and improved cosmesis. 15 Laparoscopic adrenal surgery can be performed both transperitoneally and retroperitoneally. More recently, a few centers have reported robotic adrenalectomy. However, this approach has yet to be effectively compared with the non-robotic laparoscopic surgery for potential merits.
A recently published meta-analysis illustrated that both retroperitoneal and transperitoneal LA procedures are associated with very low complication rates and similar surgical outcomes. 16
There are several published studies that have described factors influencing postoperative outcome and complications in LA. Kulis et al. 17 previously reported a study of 306 patients who underwent 326 LA procedures. In this cohort, patients had mean EBL of 60 mL, mean LOS of 4 days, and a mean tumor size of 5 cm. Conversion rate was 0.6% (n=2), and the postoperative complication rate was 1% (n=3). Bilateral adrenalectomy was the only procedure that was associated with a significantly prolonged LOS (P=.004). Similarly, Gupta et al. 8 reported that totally dependent functional status (measured using the criteria of the American College of Surgeons National Surgical Quality Improvement Program) and peripheral vascular disease were associated with increased 30-day morbidity.18,19 Impaired sensorium (7.8 days), preoperative pneumonia (5.4 days), hemiplegia (3.4 days), prior operation within 30 days (3.1 days), history of transient ischemic attack (1.4 days), disseminated cancer (1.3 days), and severe chronic obstructive pulmonary disease and National Surgical Quality Improvement Program-dependent functional status (9.5 days for totally dependent status and 3.8 days for partially independent) were associated with increased hospital LOS in the multivariate regression model. Bergamini et al. 20 compared the outcomes and complication rates of LA procedures between referral and nonreferral centers in a retrospective study. They reported that BMI, tumor size, and age were all significantly elevated in patients who experienced complications. Moreover, pheochromocytoma histology and large mass dimension were significant risk factors for perioperative complications. A summary of published perioperative outcomes in patients undergoing LA is detailed in Table 6.
Kwak et al. 25 was a comparative study with conventional transperitoneal laparoscopy versus single-port laparoscopy; the conventional transperitoneal laparoscopy subgroup was considered. Berber et al. 26 and Dickson et al. 28 were comparative studies with conventional transperitoneal laparoscopy versus posterior retroperitoneoscopy; the conventional transperitoneal laparoscopy subgroup was considered.
With or without elevated serum and/or urine metanephrines.
Stated as “negligible as no case required transfusion” in the original article.
Required a perioperative 400-mL blood transfusion.
BMI, body mass index; EBL, estimated blood loss; F, female; LOS, length of stay; M, male; NA, not applicable.
With regard to tumor size, a greater risk of complications was noted in the present study for patients undergoing LA for larger tumors compared with patients with smaller tumors. However, given that the current study does not contain data for patients undergoing open adrenalectomy, similar data related to complications in this group of patients are not available for comparison. This is a limitation of the current study, and conceivably patients with larger tumors undergoing open adrenalectomy may also be at higher risk of experiencing complications. Nonetheless, data related to tumor size for patients undergoing laparoscopic adrenalectomy can be used to counsel patients prospectively.
Another important impact of tumor size in patients undergoing adrenal surgery is the risk of malignancy for larger tumors. A higher rate of malignancy has been noted in patents with adrenal tumors >5 cm. 21 Given these data and case reports suggesting a higher recurrence risk associated with LA, open surgery is often recommended for patients with large tumors.22–24 Although our experience with LA for properly selected large tumors has yielded generally favorable results, open surgery should be considered for large tumors at high risk for malignancy. Nevertheless, our series does not include enough large tumors with sufficient follow-up to evaluate the oncologic efficacy of LA. Further studies are needed to define the oncologic efficacy of LA in comparison with other approaches.
In a previously published study we reported on a patient group with similar clinical presentations and histopathology. 13 Operative outcomes and complications were improved when compared with open adrenalectomies, with a mean EBL of 178 mL, hospital LOS of 3.1 days, and a postoperative complication rate of 5% (5/100). Data from the current study illustrate that postoperative LA outcome has generally improved at our center, which may partially be related to increasing surgical experience during the intervening 6 years. 13 When the patient characteristics and tumor histology are compared with those in previously published studies, mean patient age, tumor size, EBL, and hospital LOS were comparable. The total number of reported complications was slightly higher in our study group; however, nearly all were minor (Clavien grade ≤2) complications.
We used ROC analysis to determine that a tumor size >7.5 cm is associated with adverse perioperative outcomes. It should be noted that a limitation of our study is that the patient cohort consisted predominantly of individuals who presented with tumors ≤5 cm (70%) (minimum–maximum, 0.6–15 cm), with an uneven distribution of tumor size. Although the tumor size cutoff of 7.5 cm may be useful for patient counseling and preoperative preparation, a larger cohort with a more normal distribution in tumor size would likely allow for greater fidelity in defining a clinically relevant tumor size cutoff for estimating perioperative outcomes. A larger study would also provide greater statistical power for studying the effects of other risk factors for adverse perioperative outcomes. An additional limitation of our analysis is that this was a retrospective study, with complications graded in a retrospective fashion. A prospective study would inherently report complications more accurately.
In this study, LA was an effective and safe surgical approach for the removal of adrenal masses. Higher ASA score, increasing patient age, and a tumor size of >7.5 cm may be useful predictors of adverse perioperative outcomes in patients undergoing LA.
Footnotes
Acknowledgments
We wish to thank Peter Haddock, PhD, for his assistance in the preparation of this manuscript.
Disclosure Statement
No competing financial interests exist.