
Abstract
Abstract
Objective:
To determine the efficacy and safety of the Memokath 051™ (PNN Medical, Glostrup, Denmark) and UVENTA™ (Taewoong Medical, Seoul, Korea) metal stents, we reviewed our experience with these two metallic ureteral stents for treating benign and malignant ureteral obstructions.
Subjects and Methods:
Twenty-seven patients who received treatment with metallic ureteral stents (Memokath 051, 10 patients; UVENTA, 17 patients) from November 2011 to May 2013 at our institution were identified and analyzed. We conducted a comparative analysis of the causes of obstruction, technical/clinical success rate, cause of failure, and complications.
Results:
No difference was observed between the two metallic stents for the causes of benign and malignant ureteral obstructions (P=.073). The Memokath 051 and the UVENTA were inserted successfully in all ureters using a retrograde technique. The mean follow-up was 13.6 months for Memokath 051 and 12 months for UVENTA (P=.244). The clinical success rate of the UVENTA was higher than that of Memokath 051 (82.4% versus 42.9%; P=.031). The causes of failure were obstruction by tumor progression (n=2) and stent migration (n=6) in cases that received Memokath 051 and stent migration (n=1) and obstruction by mucosal hyperplasia (n=2) in UVENTA. The complications caused by Memokath 051 were intermittent flank pain (n=1) and acute pyelonephritis (n=1), whereas those of UVENTA were intermittent flank pain (n=1), gross hematuria (n=1), and acute pyelonephritis (n=1).
Conclusions:
The UVENTA achieved a higher clinical success rate than the Memokath 051. Our study demonstrated that the UVENTA is safe and effective in the management of benign and malignant ureteral obstruction. The complications were similar between the two metallic stents.
Introduction
U
Various kinds of new stents have been developed to remedy the shortcomings of double J stents, PCN, and surgical reconstruction: coiled metal wire stents (Resonance®; Cook Urological, Cook, IN), metal coil-reinforced double J stents (Silhouette®; Applied Medical, Cleveland, OH), segmental thermo-expandable metal alloy stents (Memokath 051™; PNN Medical, Glostrup, Denmark), and self-expandable covered metallic stents (UVENTA™; Taewoong Medical, Seoul, Korea).
This is the first report of clinical experience comparing the efficacy, safety, and complications of Memokath 051 with those of UVENTA. This study will present our institutional experience comparing the Memokath 051 and UVENTA stents.
Subjects and Methods
Twenty-seven patients (Memokath 051, 10 patients, 14 ureter units; UVENTA, 17 patients, 17 ureter units) received two metallic ureteral stents (Fig. 1) at our institution from November 2011 to May 2013 and were included. Data were retrospectively identified and analyzed from all electronic medical records of patients who underwent placement with two metallic ureteral stents. This study was approved by the institutional review board of our hospital (Institutional Review Board protocol number KCBRISI0681). All procedures were conducted according to the ethical guidelines of the Declaration of Helsinki.
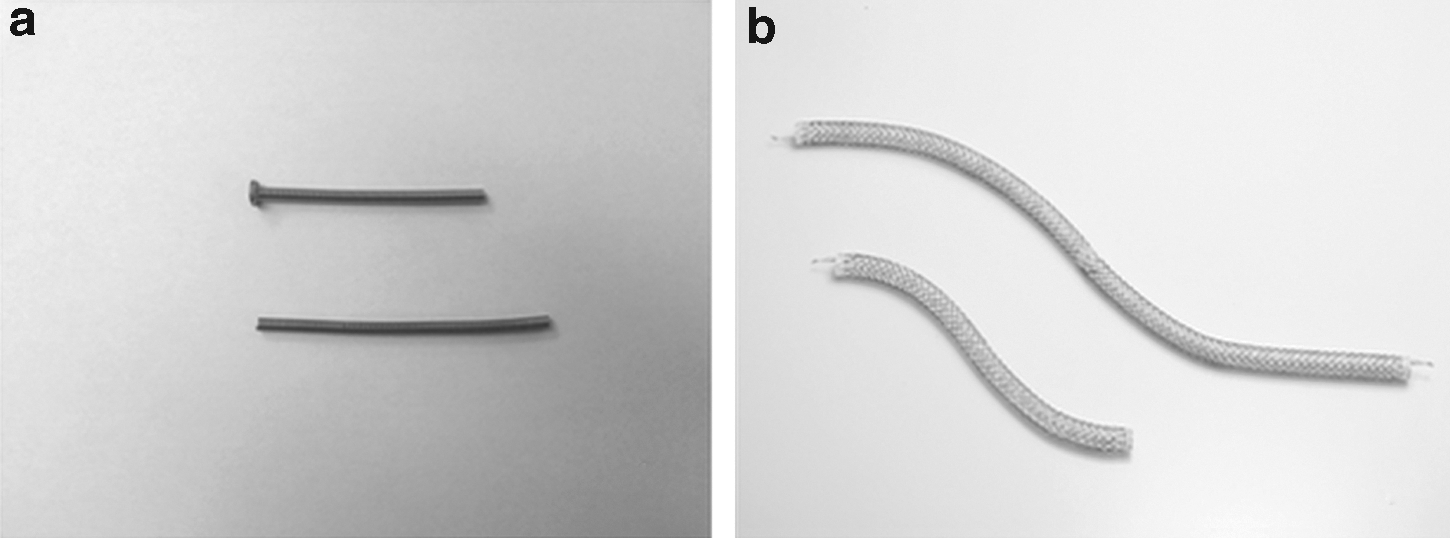
Pictures of
All patients were initially treated with a double J stent. Ureteral obstructions occurred at single or multiple sites. All patients provided informed consent before undergoing a procedure. The content of the informed consent form was that metallic stents could be changed less frequently and result in fewer irritative lower urinary symptoms. Two metallic stents were inserted by one of two experienced endourological surgeons (H.J.C. or S.-H.H.) at our institution. The details of the techniques used have been described previously.6–9 In brief, after the length and location of the stricture sites were identified by retrograde pyelography, they were marked on the anterior abdominal wall with a metallic probe to maintain accurate stent placement across the stricture site before insertion of the Memokath 051. The stricture site was dilated, the dilator sheath was passed beyond the proximal site of the stricture, and the stent assembly was inserted into the dilator sheath. After the dilator sheath and guidewire were removed, 5–10 mL of heated 50°C sterile water was injected into the stent sheath for expansion. Prior to inserting the UVENTA, we performed a retrograde pyelography to identify the stricture site. A rigid guidewire was inserted to maintain strength during balloon dilation and stent placement. This stent was expanded spontaneously by its own radial force. If the stent diameter was insufficient, additional ureteral dilation was performed with the stent using a ureteral balloon catheter. In the case of a long ureteral stricture, additional stents were inserted with an approximate 2 cm overlap.
All patients underwent radiography of the kidneys, ureters, and bladder (Fig. 2) after two metallic stents were placed to confirm their position. After the procedure was completed, all patients were scheduled for follow-up at our outpatient clinic at 1 week and at 3, 6, and 12 months after stent insertion. Urinalysis, urine culture, serum creatinine level, intravenous urography, and computed tomography were performed, and, if necessary, diuretic renography was performed at the follow-up examination in relevant patients. All patients were told to visit the hospital if they experienced flank pain, severe hematuria, dysuria, or fever. To assess the efficacy of these two metallic stents, we used the terms of technical and clinical success and failure. Technical success was defined as successful stenting of the ureteral stricture and was confirmed by intraoperative fluoroscopy and perioperative kidneys, ureters, and bladder. Clinical success was defined as improved renal function and no obstruction on intravenous urography, computed tomography, or diuretic renography. Failure was defined as deteriorating renal function with an increasing serum creatinine level or stent-related complications such as migration, premature removal, re-insertion of the same or another stent, and intolerance to severe stent-related symptoms.
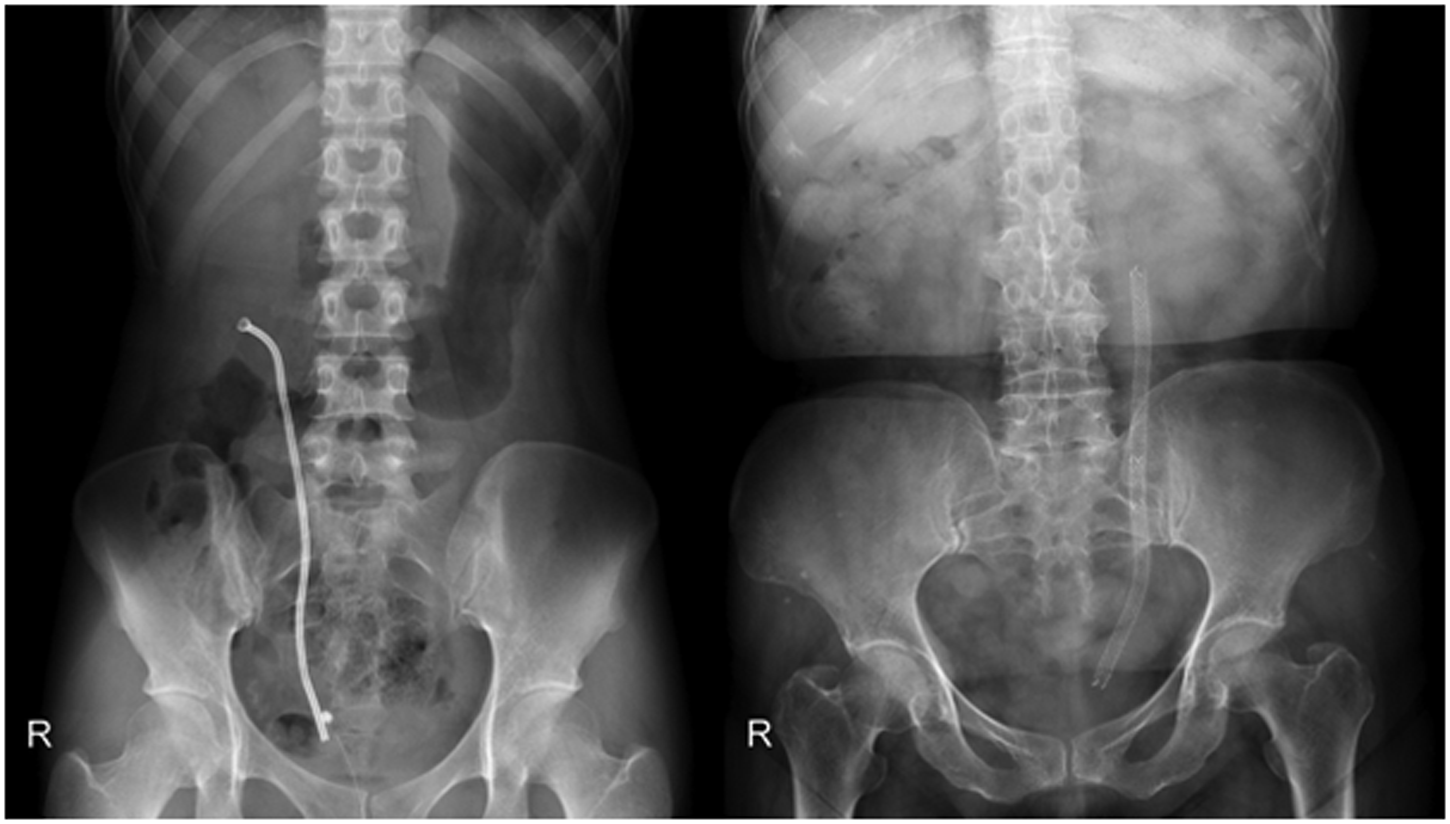
Kidneys, ureters, and bladder
Statistical comparisons of continuous data were performed with Student's t test. The chi-squared test was used to compare the categorical data. Values of P<.05 were considered significant. The statistical analysis was performed using SPSS software (SPSS Inc., Chicago, IL).
Results
Demographics including gender, mean age, side and site of obstruction, and disease characteristics are shown in Table 1. Thirty-one metallic stents were inserted in 11 male and 16 female patients. Mean patient age was 60±19 years in the Memokath 051 group and 56±15.9 years in the UVENTA group. Both metallic stents were inserted using a retrograde approach under cystoscopy and fluoroscopy in all patients, and no intraoperative or immediate postoperative complications were observed. Four patients had bilateral ureteral obstructions; thus, 14 Memokath 051 ureter units were inserted in 10 patients (benign strictures, eight ureter units; malignant strictures, six ureter units). Seventeen UVENTA ureter units were inserted in 17 patients (benign strictures, 5 ureter units; malignant strictures, 12 ureter units). The most common malignant cancer diagnoses were gastrointestinal and gynecological cancers. Two ureters with the UVENTA had vesicoureteral anastomosis strictures after kidney transplantation. The indications for the inserted metallic stents are described at Table 2. Short-term regular change of a double J stent, severe irritative lower urinary tract symptoms, and gross hematuria caused by a double J stent were the main causes for inserting two metallic stents.
More than a two-site obstruction.
SD, standard deviation.
Table 3 describes the comparative analysis results. The mean indwelling times of the Memokath 051 and UVENTA were 13.6 months (range, 7–21 months) and 12 months (range, 9–16 months), respectively (P=.244). The clinical success rates of the Memokath051 and UVENTA were 57.1% (6/14 ureter units) and 87.5% (14/17 ureter units), respectively (P=.031). Success rates of the Memokath051 and UVENTA in a benign ureteral obstruction was similar (50% versus 60%; P=1.000), but success rates in the malignant obstruction were significantly different (33% versus 92%; P=.022). Success rate of the two metallic stents except for stent migration was similar (85.7% versus 88.2%; P=.835) in the benign and malignant obstruction. Three months after insertion of the Memokath 051, the postoperative serum creatinine level decreased compared with the preoperative serum creatinine level (1.66±1.11 mL/minute versus 1.47±1.04 mL/minute; P=.038). The postoperative serum creatinine level 3 months after insertion the UVENTA was similar to that of the preoperative creatinine level (1.22±0.52 mL/minute versus 1.01±0.42 mL/minute; P=.041).
APN, acute pyelonephritis; SD, standard deviation.
The reason for failure of the metallic stents included obstruction by tumor progression in two ureters and stent migration in six ureters after insertion of the Memokath 051 and obstruction by mucosal hyperplasia in two ureters after insertion of the UVENTA. The Memokath 051 that migrated to the kidney from one ureter was removed via an anterograde percutaneous approach, whereas the stents that migrated anterogradely were removed cystoscopically. Two cases of obstruction by tumor progression were managed by PCN, and six cases of migration were managed by substituting other metallic stents (UVENTA, Resonance) or by re-inserting a Memokath 051. After re-insertion of a metallic stent, there was no need to insert additional stents. Two cases of obstruction by mucosal hyperplasia in the UVENTA group were managed by additionally inserting an UVENTA. No severe complications were observed during follow-up. The complications for the Memokath 051 were intermittent flank pain in 1 patient and acute pyelonephritis in another patient, whereas those for the UVENTA were intermittent flank pain in 1 patient, intermittent gross hematuria in 1 patient, and acute pyelonephritis in 1 patient. Flank pain and acute pyelonephrititis were managed with oral analgesics and oral antibiotics, respectively. The patient with intermittent gross hematuria from the UVENTA was close to follow-up without any additional intervention. Two patients (Memokath 051, 1 patient; UVENTA, 1 patient) died because of their original malignancy, and no ureteral obstruction was observed at their last follow-up. The rest of the patients are alive with functioning metallic stents except for 2 cases of PCN.
Discussion
There is a demand for minimally invasive techniques and stents that last longer without having to change them out to manage ureteral obstruction. The ideal stent should be easily inserted, maintain patency with no additional interventions, create longer durations between stent changes, and be easily eliminated.
Metallic stents are used in the cardiovascular and hepatobiliary field. After the first adoption of metallic stents for treating urethral strictures in the urologic field, 10 metallic stents for managing ureteral obstructions were introduced to resolve problems and limitations encountered with the use of double J stents or PCN.
The Memokath 051 is a thermo-expandable stent made from nickel–titanium alloy that has a propensity to close in a tight spiral structure that prevents urothelial ingrowth, preserves peristalsis, and reduces the risk of secondary ischemic damage to the ureteric wall. 11 The UVENTA is made of an inner mesh-polytetrafluoroethylene (PTFE) membrane, and the outer mesh has a feature that prevents tissue ingrowth and reduces the risk of urothelial hyperplasia. The middle PTPE membrane and inner mesh prevent tissue ingrowth and reinforce the overall radial force of the stent to maintain patency, and the biocompatible PTPE reduces irritation and encrustation. The outer mesh prevents stent migration by holding the ureteral urothelium. 12 All of these features indicate that these stents will be adopted for long-term use as an attractive treatment option instead of double J stents or PCN.
The most important aspect of a metallic stent is maintaining patency of the ureter without severe complications. Agrawal et al. 13 recently reported on a long-term (11-year) follow-up of Memokath 051 with an 89.3% success rate (25 of 28 patients) in treating malignant ureteral obstructions. Another study of the Memokath 051 stent reported on 73 patients with ureteral strictures during 11 months of follow-up, and the overall success rate was 93% (66 of 73 patients); they concluded that the Memokath 051 stent is a safe, efficient treatment modality for minimally invasive management of ureteral strictures. 14 We showed a lower clinical success rate (42.9%) compared with those of recent studies. We consider that the cause of a lower clinical success rate for the Memokath 051 is stent migration. Migration rates from published series vary from 12% to 45%.7,13–15 The stent migration rate (43%) in the present study was similar but a little high compared with the published series. Some studies elucidated the causes of stent migration and reported that nonanchorage of the coated stents to the ureteral wall and anterograde peristalsis of ureters were the main causes.16,17 Six Memokath 051 stents migrated, including 5 cases of benign ureteral stricture and 1 case of gynecological cancer that underwent ureteral dilatation. In contrast, one study reported that malignant strictures are associated with increased risk for stent migration. 14 Arya et al. 18 showed no significant difference in benign and malignant strictures in terms of stent migration. Although we had a small number of cases, we hypothesize that stent migration occurs because of ureteral dilatation over the maximum stent diameter before insertion of the stents regardless of the benign or malignant nature of the obstruction. One study recommended that balloon dilation to enlarge the width of the ureter wider than that of the Memokath 051 should be avoided to prevent stent migration. Because both groups did not have a large number of patients, it was difficult to determine the factors of success and failure of each stent, but in situations when the stricture region was not long or severe, or when there was severe ureteral dilatation of the upper part of the stricture that led to frequent migration of the Memokath 051, the UVENTA stent would be more efficacious.
Self-expandable metallic stents have been used in gastroenterology, particularly for gastric outlet obstructions. 19 However, clinical experience with the use of the UVENTA for ureteral obstructions has been limited. The clinical effectiveness of the UVENTA for managing ureteral obstruction has been evaluated in three studies.8,9,20 Kim et al. 9 reported on the UVENTA for managing malignant ureteral obstructions of 20 ureters with a patency rate of 100% after a mean follow-up of 7 months. A large volume, mid-term (3-year) study recently reported the efficacy and safety of the UVENTA for treating malignant ureteral obstructions, and the overall success rate was 82% (58/71 ureters); they concluded that the UVENTA is an effective and safe treatment modality for palliative treatment of malignant ureteral obstructions. 8 The UVENTA success rate in our study was 82.4% (14/17 ureters), which is comparable with the three recently published studies. One patient who had undergone a kidney transplant had a stent inserted in the ureter, but stent migration occurred. The migrated stent was removed, and a new one was re-inserted. The new stent had good patency shown at follow-up. There were also 2 patients who had complications of mucosal hyperplasia after the ureter stenting procedure. One of the patients had a new stent exchanged for the old one, and good patency was maintained. The other patient had an additional stent added to the site where mucosal hyperplasia occurred, and the stent has been maintained good patency.
It is difficult to compare these two metallic stents because of various causes of ureteral obstruction. However, we were able to compare these two metallic stents because the cause and nature of the ureteral obstructions were similar in our study. This is the first study that compared the efficacy and safety of the Memokath 051 with those of the UVENTA. Thus, we think that this study provides important information about the role of both metallic stents in the management of ureteral obstruction. Although technical insertion of both metallic stents was successful in all cases, the clinical success rate was clearly different between the two stents. The cause of the different clinical success rates was frequent stent migration by the Memokath 051. However, the clinical success rate except stent migration was similar between the two metallic stents. This result suggests that careful patient selection and the delicate insertion procedure are important to accomplish better outcomes with use of the Memokath 051.
All cases of ureteral obstruction or stent migration after insertion of two metallic stents were managed, and patency was maintained, except in two ureters with intractable obstructions due to tumor progression in the Memokath 051 group that were managed by PCN. This means that even if problems after insertion of metallic stents occur, they can be resolved easily using the same or different metallic stents. The complications related to both metallic stents were few and minor. These two metallic stents have a lower incidence of irritative voiding symptoms as well, although we did not evaluate this using validated questionnaires. The complications were treated on an outpatient basis without additional admissions. We performed diuretic renography in some clinically successful patients to confirm the absence of ureteral obstruction, and no obstructions were found. This result supports the effectiveness of the two metallic stents. Our results provide a clear place for these metallic stents in the management of patients with benign or malignant ureteral obstructions without severe complications.
This study has several limitations. First, this was a retrospective study, and the enrolled number of patients was small. Because there is a significant expense and a cost difference between the Memokath 051 and the UVENTA ($2938 versus $923, respectively) in Korea and because one of the two metallic stents was inserted into the patients who selected two metallic stents after informed consent was obtained, it was difficult to execute a prospective, randomized study and enroll a large number of patients. Second, the duration of follow-up was relatively short in the present study. A long-term follow-up will be needed to confirm the efficacy and safety of the two metallic stents. Consequently, we will execute a long-term comparative study to evaluate efficacy and safety of both metallic stents, including an assessment of quality of life and lower urinary tract symptoms using a validated questionnaire.
Conclusions
The outcome of our study showed that the UVENTA stent had a higher success rate than the Memokath 051 and that patients with benign and malignant ureteral obstruction can be treated safely and effectively with the UVENTA. In addition, because the Memokath 051 stent migrated frequently, it would be better used in selected patients. The complications in both groups were few, minor, and similar. We recommend that further long-term, multicenter studies be conducted to evaluate the long-term efficacy and safety of both metallic stents.
Footnotes
Disclosure Statement
No competing financial interests exist.