
Abstract
Abstract
The approach to inguinal hernia in the pediatric population has historically been via an open technique. Over the last decade there have been numerous reports and descriptions of laparoscopic techniques to repair inguinal hernias in this population. This article highlights different techniques and clearly outlines the currently utilized approach in our institutions.
Introduction
W
For this purpose of this technical review, we will categorize the different repair options as either intracorporeal or extracorporeal/percutaneous.
Intracorporeal Techniques
As a general rule, all intracorporeal techniques involve a total laparoscopic approach to obliterating the patient processus vaginalis. Typically, these repairs necessitate the placement of a minimum of two laparoscopic instruments, plus a site for the laparoscope. The hernia sac may be managed with excision alone, suture ligation of the sac, or a combination of excision and ligation.
The first intracorporeal repair was reported in girls by Felix Schier. 1 He described closure of the ring using one or two Z-stitches, which were placed to bring the edges of the ring together.
The second report of a totally intracorporeal repair came in 2004 and is described as the “laparoscopic flip-flap hernioplasty.” 2 During the approach, the anteriolateral border of the hernia sac, at the level of the internal ring, is divided and brought medially. The lateral edge is then sewn to the medial edge of the internal ring. In theory, this technique not only closes the patent processus vaginalis, but it moves the sac closure site away from the opening in the muscle. 2 Although the authors reported no recurrences at 3 years later, Hassan and Mustafawi 3 reported a very high recurrence rate with this technique.
In 2004, Becmeur et al. 4 described the laparoscopic division and resection of the hernia sac at the level of the internal ring, with subsequent closure of the peritoneal edges with 3-0 polyglactin 910 (Vicryl®; Ethicon Endo-Surgery, Blue Ash, OH) suture. Others have validated the efficacy of this technique. 5
Zallen and Glick 6 described the laparoscopic inversion and ligation technique for girls in 2007. This technique involves grasping the hernia sac at its base through the canal of Nuk. The sac is then inverted into the peritoneal cavity and ligating it with a pretied laparoscopic suture loop.
Extracorporeal/percutaneous techniques
The extracorporeal techniques all involve the placement of a suture circumferentially around the internal ring and tying the knot using percutaneous techniques. Many variations of this approach have been described.
In 2005, Spurbeck et al. 7 described a percutaneous technique in which a curved “awl” (a blunted tip curved instrument with a eyelet hole in the tip) is passed through a tiny stab skin incision in the groin into the retroperitoneum. It is passed laterally around the internal ring, above the cord structures, and out into the peritoneal cavity. Using a laparoscopic instrument through a separate incision, the suture is removed from the tip of the awl. The awl is then passed medially around the internal ring, back into the peritoneal cavity, where the suture is threaded back into the hole in the tip of the awl. The awl is then withdrawn, thus bringing the suture circumferentially around the ring.
This approach has been described in several variations around the world. Oue et al. 8 described a similar technique using a Japanese laparoscopic port suture closure device, and Shalaby et al. 9 reported the same technique using a Reverdin needle.
Ozgediz et al. 10 reported the subcutaneous endoscopically assisted ligation technique. Under laparoscopic guidance, the internal ring is encircled with a braided, nonabsorbable suture on a large needle from one side to the other, skipping over the cord structures in one movement. The tip of the needle is then brought out through the skin on the other side. The needle tip is grasped with a needle driver, and the heel of the needle is backed through the subcutaneous tissue and out of the original stick site. The suture is then tied, thereby closing the ring.
Our current technique—Percutaneous closure with intentional anterior internal ring injury
Our technique for laparoscopic inguinal hernia repair is a percutaneous closure of the internal ring. We use a modification of the technique described by Patkowski et al. 11 Our modification includes three steps. The initial modification includes hydrodissection beneath the peritoneum, to elevate the peritoneum away from the posterior aspect of the abdominal wall and cord structures. The second modification is the utilization of two looped sutures to allow for the exchange of the monofilament suture for a braided suture. The third modification is the intentional peritoneal injury prior to closure of the hernia sac.
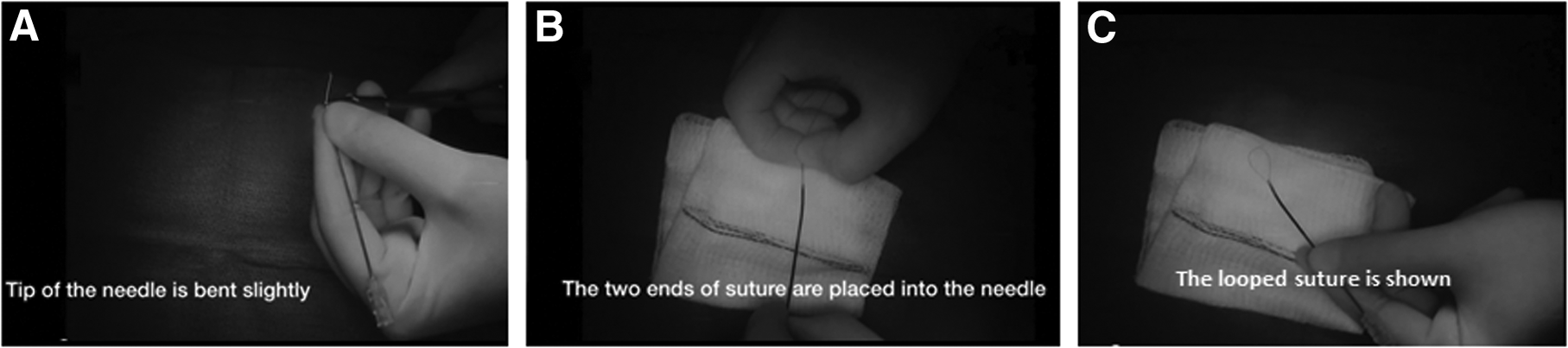
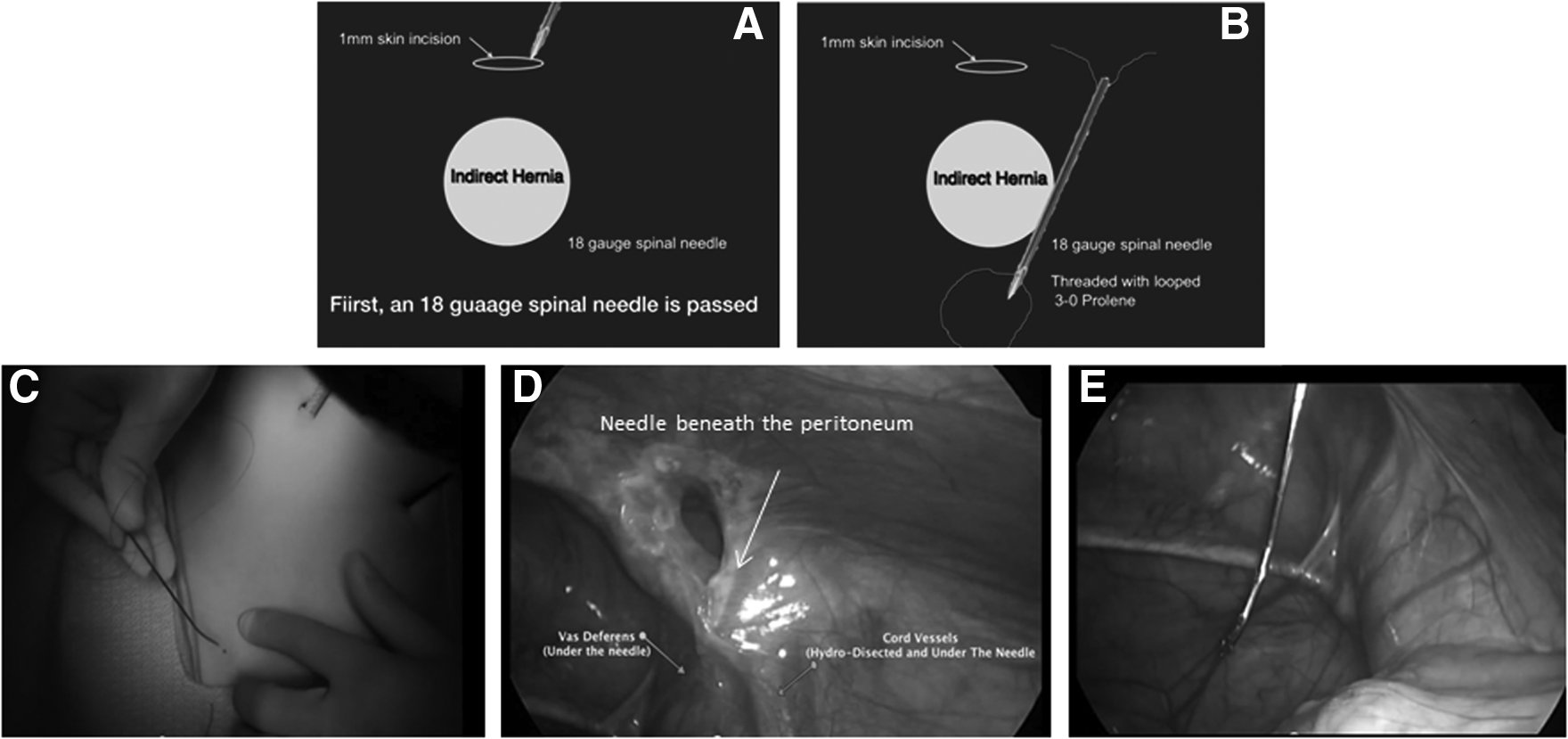
Prior to beginning the operation, an 18-gauge spinal needle is intentionally bent into a gentle curve using two needle drivers and threaded with a looped 3-0 monofilament suture with the loop coming out of the tip of the needle. The loop is pulled just inside the tip of the needle (Fig. 1). The operation is initiated by inserting an umbilical port for the laparoscope and a 3-mm Maryland dissector, which is placed through a stab incision in the lower abdominal wall. The Maryland dissector will be used to cauterize the peritoneum from the 8 o'clock to the 5 o'clock position of the internal ring. Our goal is to cauterize the entire internal ring except for the area overlying the cord structures. This creates a scar, which leads to superior closure, as we have shown in the rabbit model. 12 The peritoneum is then cauterized from approximately the 8 o'clock to 5 o'clock positions, with great attention taken to not encroach on the cord structures (Fig. 2A).
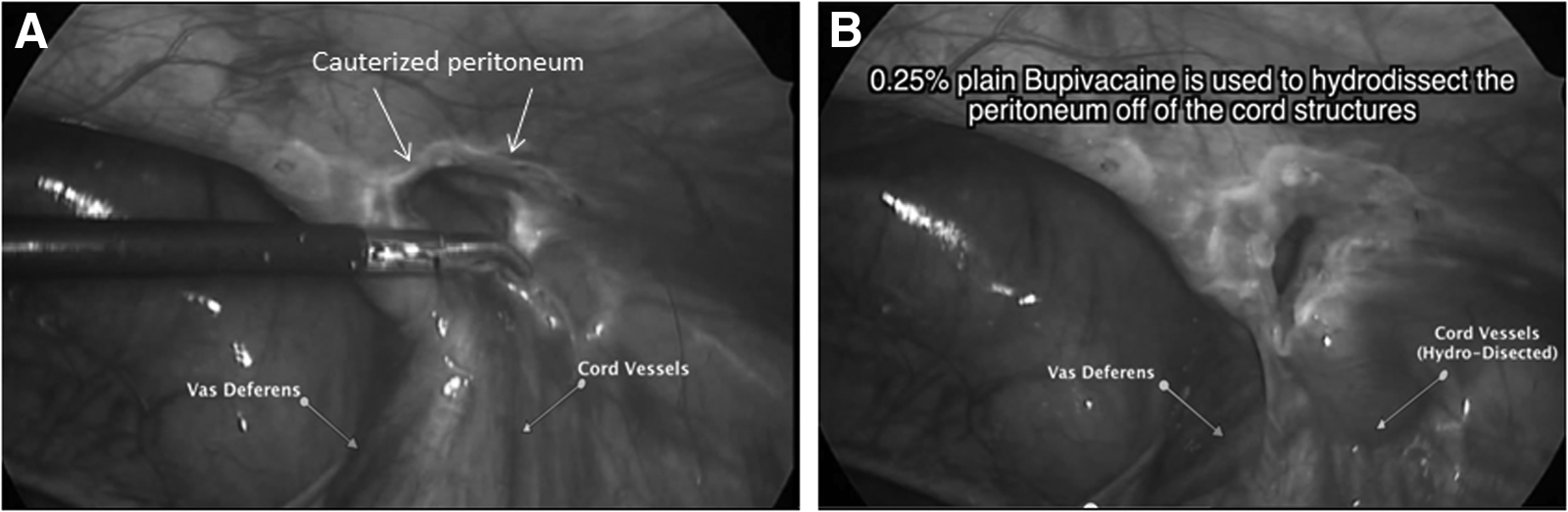
The Maryland dissector has been used to cauterize around the internal ring. The peritoneum is being grasped, and
A 25-gauge finder needle is used to identify the 12 o'clock position of the internal ring at the level of the patent processus vaginalis. A 1-mm incision is made in the skin at this point. Prior to passing the suture, hydrodissection is performed to elevate the peritoneum off of the cord structures (Fig. 2).
The threaded curved spinal needle is inserted through the 1-mm skin incision until it is seen beneath the peritoneum at the 12 o'clock position (Fig. 3C). It is then passed around the internal ring, between the posterior abdominal wall and peritoneum, where the hydrodissection has been performed. We usually proceed from the 12 o'clock position laterally around the ring. The needle is passed beneath the peritoneum over the vessels (and vas if possible) (Fig. 3D). The 3-mm instrument can be used to assist with lifting the peritoneum away from the cord structures at this point if necessary. Once the vessels have been traversed, the needle is pushed through the peritoneum into the peritoneal cavity, and the loop of monofilament suture is pushed out of the needle (Fig. 3E). The needle is removed from the peritoneal cavity, leaving a looped suture in the peritoneum with the tails exiting through the 1-mm skin incision.
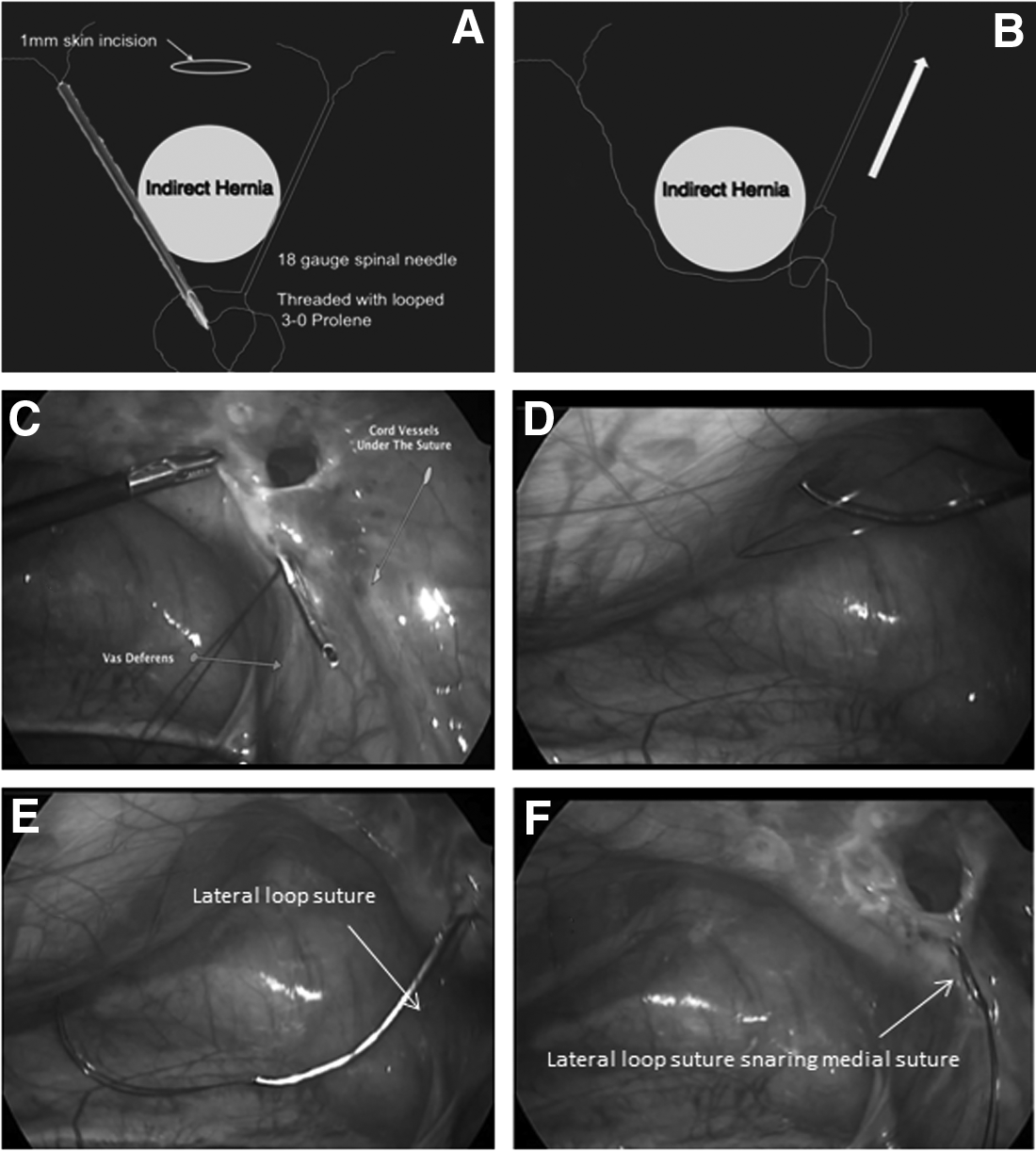
The next step is essentially a repeat of the previous step. The needle, which has been loaded with another looped monofilament suture, is passed from the 12 o'clock position around the ring in a medial fashion. As the vas deferens is approached, every attempt is made to pass this needle between the peritoneum and the vas deferens, with great care taken to not injure the vas. It can be challenging to develop the space between the peritoneum and the vas, even with the use of the 3-mm instrument that was used to incite the injury. If it is not possible to pass the needle safely across the vas, the needle can be passed into the peritoneal cavity just medial to the vas, thereby “skipping out over the peritoneum” at this point (Fig. 4C). The needle is passed through the loop that was initially placed laterally (Fig. 4D). The lateral loop is then pulled snug against the needle, and the threaded suture in the needle is pushed out into the peritoneal cavity (Fig. 4E). The needle is then removed, resulting in the lateral loop snugly securing the medial loop. The lateral loop now functions as a snare or lasso (Fig. 4F). By pulling on the lateral loop, the medial loop is circumferentially brought around the ring and out through the skin. At this point the medial loop could be tied down, closing the peritoneum. However, we prefer to exchange this suture with a braided, nonabsorbable suture, because of its characteristic softer knot.
Therefore, the braided, nonabsorbable suture is passed through the monofilament loop that is currently around the hernia sac, and the free ends of the monofilament are pulled retrograde, pulling the new loop of suture through the same space around the internal ring and out through the skin incision (Fig. 5A–D). The looped braided suture is then cut at the apex of the loop, thereby providing for a double ligation of the ring (Fig. 5E and F). Of note is that the braided suture cannot be used to pass through the spinal needle in the first steps of this procedure because it is not stiff enough to pass through the needle. Therefore it must be exchanged at the end of the case. The sutures are then tied closing the hernia sac (Fig. 6), and the knot is positioned in the subcutaneous tissue. The tiny skin incision is then closed with a Steri-Strip™ (3M, St. Paul, MN) or surgical glue.
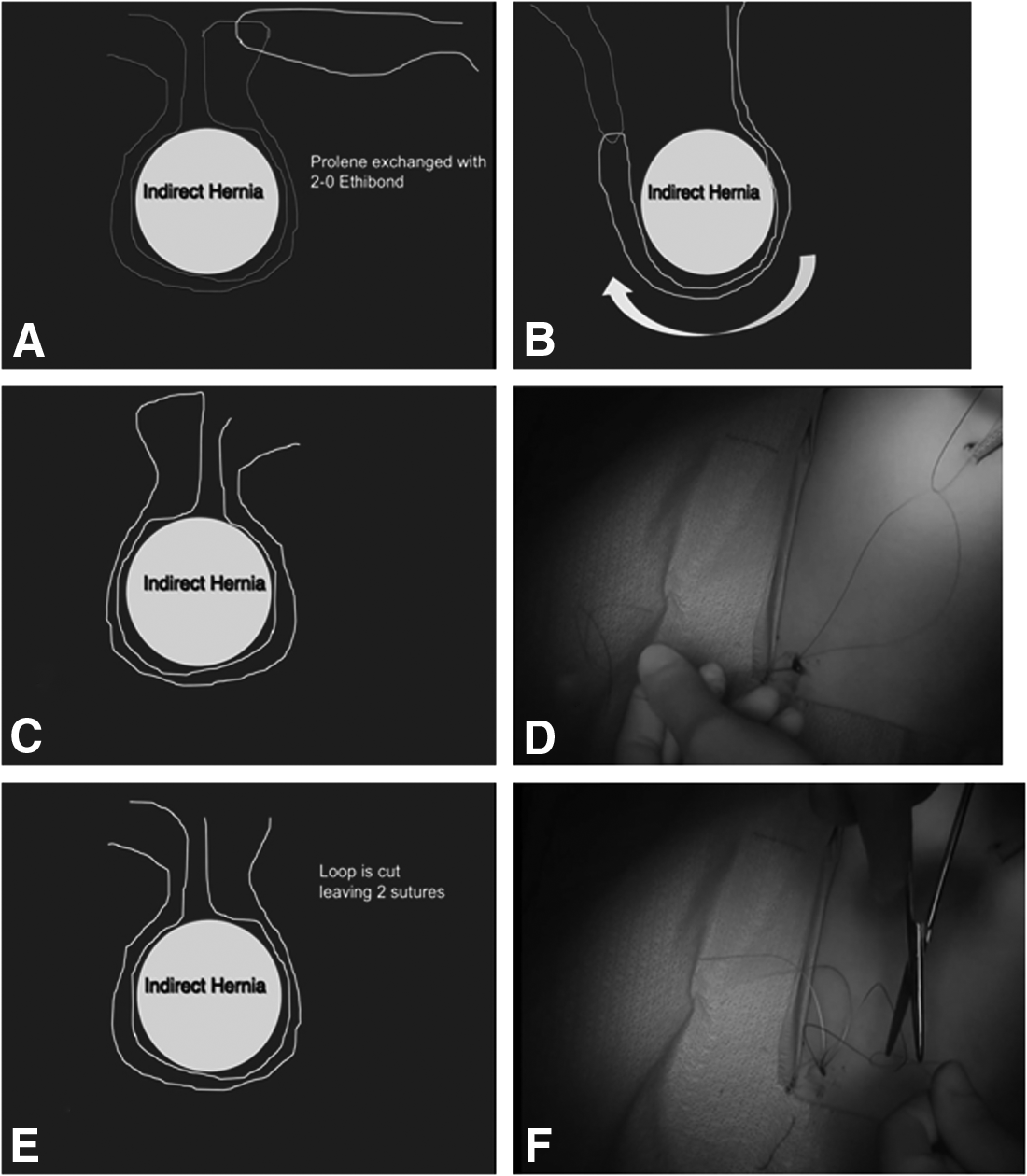
The existing looped suture is exchanged for a braided, nonabsorbable suture, which will be used to ligate the sac. This is shown
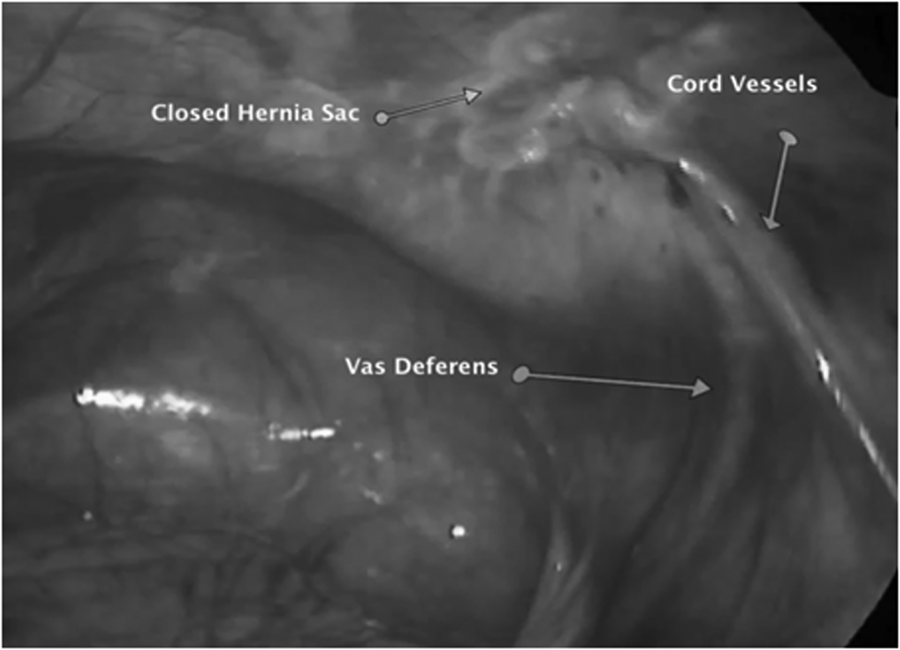
The finished repair is shown with complete closure of the hernia sac at the internal ring.
Conclusions
Although this article provides an overview of the most popular techniques used for laparoscopic pediatric hernia repair, there are several other variations that were not necessarily mentioned here. The key take-home points are that the surgeon can decide between a percutaneous or intracorporeal approach to these repairs. The authors believe that there is not sufficient evidence to support one approach over another. However, there is support that suggests that addition of the peritoneal injury intentionally created at the internal ring does result in a more durable repair. We have described our preferred technique in great detail because we feel is easy to learn, safe, and effective.
Footnotes
Disclosure Statement
No competing financial interests exist.