
Abstract
Abstract
Introduction:
Laparoscopic liver resection under hemihepatic vascular inflow occlusion has advantages over the conventional Pringle's maneuver, especially in patients with cirrhosis. However, laparoscopic hemihepatic vascular inflow occlusion is technically challenging.
Subjects and Methods:
From March 2013 to August 2013, 8 consecutive patients who underwent laparoscopic liver resection under right hemivascular inflow occlusion using the lowering of the hilar plate approach.
Results:
There were 3 women and 5 men, with a mean age of 52.6 years (range, 44–73 years). The pathologies were hepatocellular carcinoma (n=3), sarcomatoid liver carcinoma (n=1), hepatic vascular epithelial tumor (n=1), hemangioma (n=2), and colorectal liver metastases (n=1). The types of resection included right hepatectomy (n=3), right anterior sectionectomy (n=1), segments 5 and 6 resection (n=1), and segment 6 resection (n=2). All patients underwent right hemivascular inflow occlusion. The mean operation time was 186.2 minutes (range, 100–280 minutes). The mean time taken to prepare for hemivascular inflow occlusion was 17.8 minutes (range, 15–20 minutes). The mean intraoperative blood loss was 218.8 mL (range, 100–300 mL). The mean duration of vascular control was 25.6 minutes (range, 15–40 minutes). No patients developed postoperative liver failure. There was no postoperative morbidity or mortality. The mean hospital stay was 6 days (range, 5–7 days).
Conclusions:
Hemihepatic vascular inflow occlusion using the lowering of the hilar plate approach was safe and feasible. It facilitated laparoscopic liver resection by minimizing blood loss during liver parenchymal transection.
Introduction
T
Laparoscopic liver resection can now be performed with a low mortality rate using new instruments that allow a relatively bloodless field during liver transection. However, the vascular inflow control technique is still often used to decrease intraoperative blood loss, especially in cirrhotic liver resection. To further develop laparoscopic liver resection, safe and efficient vascular control techniques during laparoscopic liver resection are important.1–3
This article described a laparoscopic technique for right hemihepatic vascular inflow control using the lowering of the hilar plate approach.
Subjects and Methods
From March 2013 to August 2013, 8 consecutive patients underwent laparoscopic liver resection under right hemivascular inflow occlusion using the lowering of the hilar plate approach. The patients who were selected for this technique had the following preoperative criteria: (1) no previous hepatobiliary surgery and (2) the tumor was not close to the porta hepatis or hepatic pedicle. The surgical procedures and the postoperative courses were evaluated. The following data were collected prospectively: operating time, time taken to prepare and duration of hemihepatic vascular inflow occlusion, perioperative blood transfusions, postoperative complications, and hospital stay.
Surgical technique
The patient was placed in a supine leg-splitting position in a reverse Trendelenburg position, with the right side tilted up at around 30°. The technique used four or five trocars. A 10-mm trocar was placed below the umbilicus. Pneumoperitoneum was established at a pressure of 13 mm Hg. A 12-mm working trocar was placed below the xiphisternum. Another two or three assistant ports (5 mm or 12 mm) were placed in the right subcostal region according to the site of the liver lesion (Fig. 1). Exploration of the abdominal cavity and intraoperative ultrasound liver examination were performed routinely.

Positions of the ports.
Cholecystectomy was carried out first. The falciform ligament was then divided, followed by the round ligament. The lesser omentum was divided at the undersurface of the liver to enter into the lesser sac. The round ligament was retracted upward and forward to expose the hepaticoduodenal ligament. A small incision was made in Glisson's capsule at its base, similar to the open technique as described by Hepp and Couinaud in 1956 as described by Lau et al. 4 The hilar plate was identified, and the plane between the liver and the hilar plate was dissected using blunt dissection with forceps and a suction catheter (Fig. 2). A similar incision of the peritoneum was made on the peritoneum posterior to the right pedicle to create a tunnel around the right pedicle (Fig. 3). After the confluence and the upper part of the right hilar pedicles were dissected, a right-angle forceps (10 mm) was introduced into the abdominal cavity. The tip of the right angle forceps was then inserted into the space between the liver above and the hilar plate below (Fig. 4). The forceps bluntly dissected around the back of the right pedicle. The forceps was guided to exit at the back of the right hepatic pedicle (Fig. 5). By gently opening the right-angle forceps, the established tunnel was widened. A cotton tape was then passed twice around the right hepatic pedicle. Afterward, the right hepatic pedicle en bloc was isolated and controlled with a cotton tape (Figs. 6 and 7). The cotton tape was tightened and fixed with a vascular lock. After liver transection, the cotton tape was released by breaking the vascular lock with an energy device.
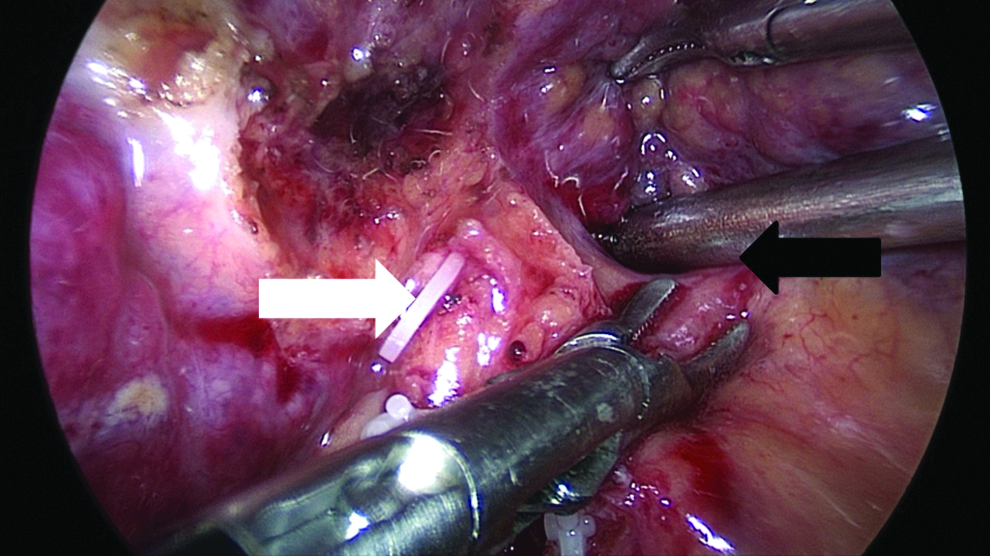
The plane between the liver and the hilar plate was dissected using blunt dissection with forceps and a suction catheter. The white arrow represents the right pedicle; the black arrow represents the hilar plate.
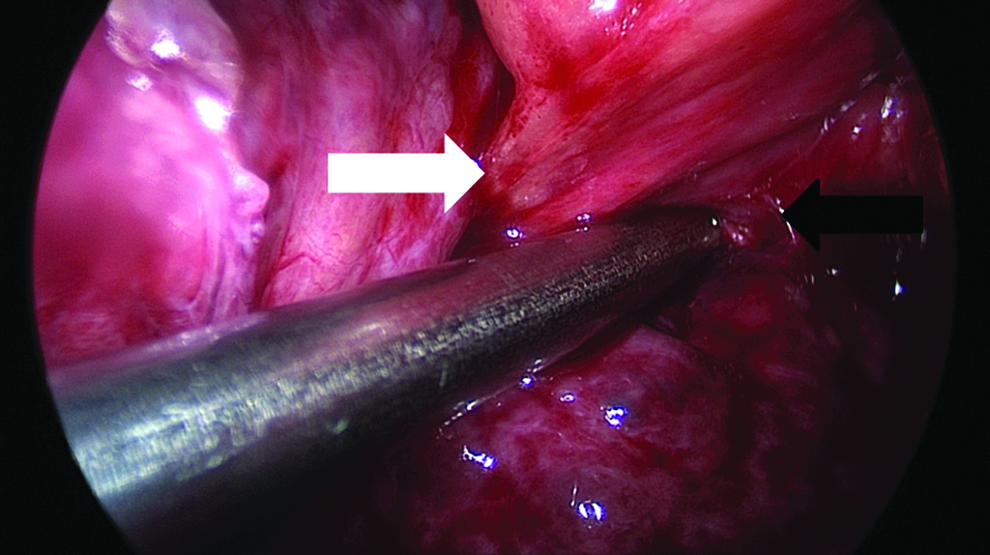
An incision was made on the peritoneum posterior to the right pedicle to create a tunnel around the right pedicle. The white arrow represents the right pedicle; the black arrow represents the hilar plate.
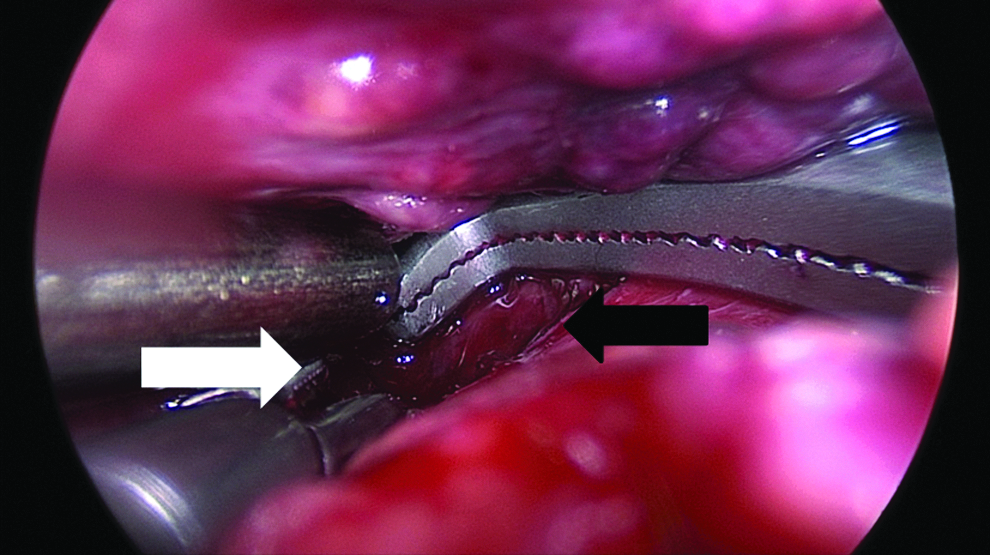
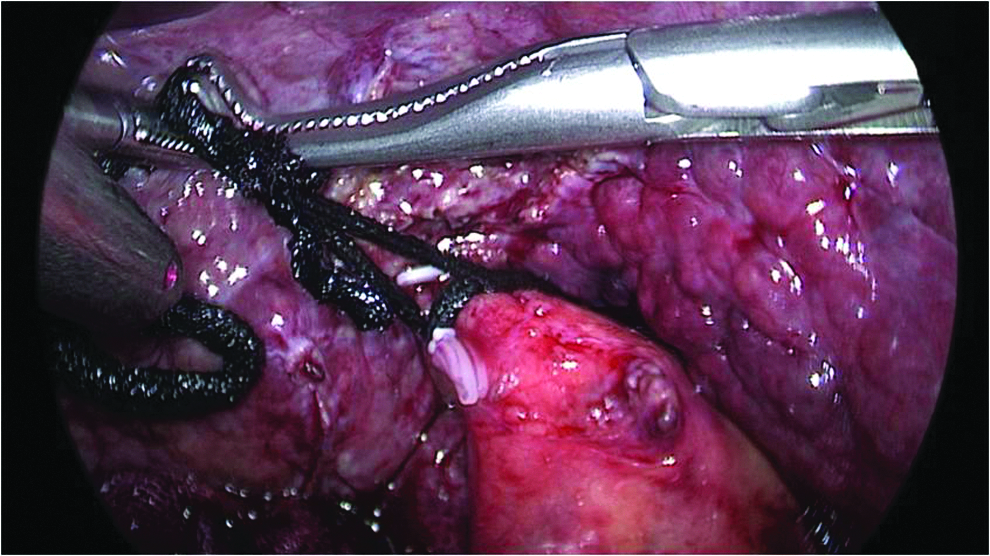
The tip of the right angle forceps was then inserted into the space between the liver above and the hilar plate below. The white arrow represents the right pedicle; the black arrow represents the hilar plate.
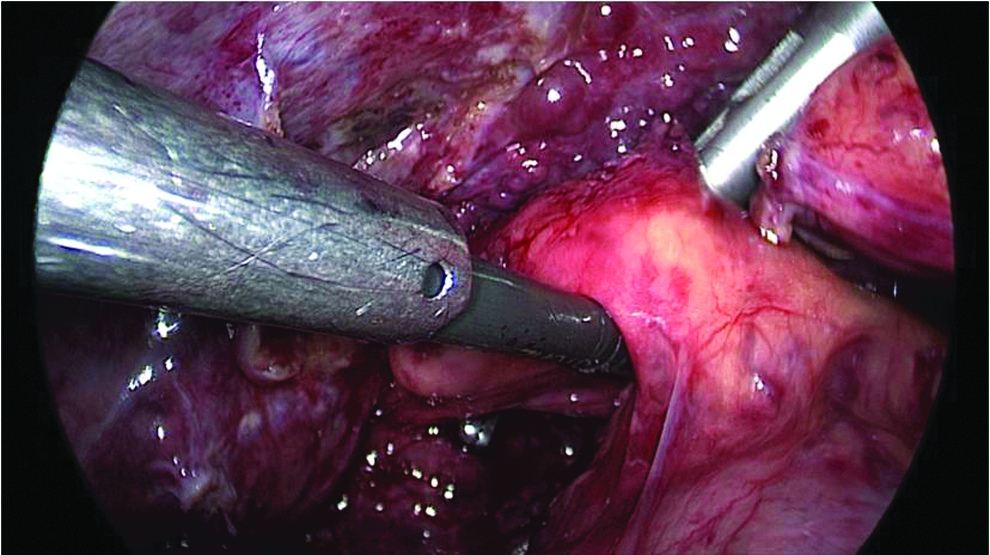
The forceps was guided to exit at the back of the right hepatic pedicle.

A cotton tape was then passed twice around the right hepatic pedicle.
The right hepatic pedicle en bloc was isolated and controlled with a cotton tape.
Liver transection was then carried out using either a Harmonic® scalpel (Ethicon Endo-Surgery, Inc., Cincinnati, OH) or a LigaSure™ (Covidien, Boulder, CO). The intrahepatic vascular branches were controlled with titanium clips, vascular locks, or suturing as appropriate. An endostapler (Endopath®; Ethicon) was used to control the right hepatic pedicle or the right hepatic vein during right hemihepatectomy. The resected specimen was removed by enlarging one of the laparoscopic port wounds.
Results
From March 2013 to August 2013, 8 consecutive patients underwent laparoscopic liver resection under right hemivascular inflow occlusion using the lowering of the hilar plate approach. There were 3 women and 5 men, with a mean age of 52.6 years (range, 44–73 years). The pathologies were hepatocellular carcinoma (n=3), sarcomatoid liver carcinoma (n=1), hepatic vascular epithelial tumor (n=1), hemangioma (n=2), and colorectal liver metastases (n=1). Four patients had cirrhosis. The liver functional status was Child's A (n=6) or Child's B (n=2). The types of resection included right hepatectomy (n=3), right anterior sectionectomy (n=1), segments 5 and 6 resection (n=1), and segment 6 resection (n=2). All patients underwent right hemivascular inflow occlusion. The mean operation time was 186.2 minutes (range, 100–280 minutes). The mean time taken to prepare the hemivascular inflow occlusion was 17.8 minutes (range, 15–20 minutes). The mean intraoperative blood loss was 218.8 mL (range, 100–300 mL). No patients required blood transfusion. The mean duration of vascular control was 25.6 minutes (range, 15–40 minutes). There was no postoperative morbidity or mortality. The mean hospital stay was 6 days (range, 5–7 days).
Discussion
Laparoscopic liver resections are becoming popular, although bleeding remains a major challenge during liver parenchymal transection. To extend the indication and popularity of laparoscopic liver resection, a safe and efficient technique of vascular control is important. Pringle's maneuver (total vascular inflow occlusion) is the traditional and the most commonly used method to decrease blood loss during hepatic parenchymal transection because of its effectiveness and simplicity. However, ischemic-reperfusion injuries can occasionally lead to postoperative liver failure. 4 Hemihepatic vascular inflow occlusion is an alternative; it selectively interrupts the arterial and portal inflow to the ipsilateral hemiliver, which contains the lesion requiring resection. 5 It decreases the amount of liver parenchyma subjected to ischemia-reperfusion damage and offers the advantage of reduced blood loss during liver transparenchymal transection. 6 Four randomized controlled trials showed hemihepatic vascular inflow occlusion to have the advantage of less liver injury after liver resection.7–10 The only drawback of hemihepatic vascular inflow occlusion is although it cuts down the amount of bleeding coming from the occluded hemiliver, there is still bleeding coming from the nonoccluded hemiliver during liver transection.
To achieve hemihepatic vascular inflow occlusion, dissecting the ipsilateral hepatic pedicle to control the ipsilateral hepatic artery and portal vein is an important step before parenchymal transection. The hepatic pedicle can be approached intrahepatically or extrahepatically. Variations in anatomy can hamper the vascular control. The intrahepatic approach avoids these risks by using en masse ligation of the structures of the portal triad without the need to dissect each structure separately. In 1952, Lortat-Jacob and Robert 11 described the first right hemihepatectomy. In their report, they isolated and dissected the related branches of the portal vein, hepatic artery, and the hepatic duct outside the liver parenchyma. An alternative method of hemihepatic vascular inflow control is the “Glissonian” approach. Takasaki 12 described the concept of hepatic segmentation and liver resection by the Glissonian pedicle transection method. The hilar structures can also be approached together without entering into Glisson's sheath. This technique is based on the pioneering works of Launois and Jamiesson 13 and Galperin and Karagiulian, 14 who described the fibrous sheath that envelops the entire portal triad, which extends into the liver. The fusion of Glisson's capsule with the connective tissue sheaths surrounding the hepatic artery branches, portal vein branches, and bile ducts (the portal triad) at the inferior aspect of the liver constitute the plate system. This plate system consists of the hilar plate above the biliary confluence, the cystic plate related and above the gallbladder, the umbilical plate above the umbilical portion of the left portal vein, and the Arantian plate covering the ligamentum venosum. Hepp and Couinaud 15 described a technique to expose the confluence of the right and left hepatic pedicles by lifting the quadrate lobe upward and incising Glisson's capsule at its base. By dissecting between the liver parenchyma superiorly and the hilar plate inferiorly, a space could be developed. This technique is referred to as lowering of the hilar plate, and it can be carried out safely because no vessel branch originates from the anterior margin or the upper surface of the hilar plate. When the hilar plate is pulled down after detaching the liver parenchyma of the quadrate lobe, the right and left Glissonian pedicles can be approached. 16 We make use of this technique to expose the left and the right hepatic pedicles for laparoscopic hemihepatic vascular inflow occlusion. Other authors17–20 have described laparoscopic control of the ipsilateral hepatic pedicles by dissecting into the liver substance just above the confluence of the right/left hepatic pedicles deep to the liver plate, instead of our method of between the liver parenchyma and the liver plate. Our technique does not need to dissect into the liver parenchyma. Previously, we used a bougie with a bending tip, and it was then inserted into the space between the liver above and the hilar plate below. The bougie bluntly dissected the back of confluence of the hilar pedicle. However, the angle of the bougie was not good enough, and the parenchyma of the caudate lobe was occasionally damaged. The technique was modified with a right-angle forceps. The angle of dissection was much improved.
This report showed that hemihepatic vascular inflow occlusion could be safe and simple, and it minimized blood loss and the ischemia time for the liver remnant. This technique can be used for pedicle transection in hemihepatectomy, and it can also be used in selective hemihepatic vascular control in resections of less than a hemihepatectomy. However, this technique should not be used if the tumor lies near the right or left hepatic pedicle. Our study was limited by the small number of patients and the lack of a control arm. More randomized or nonrandomized trials comparing with Pringle's maneuver are needed to evaluate this technique.
Disclosure Statement
No competing financial interests exist.