
Abstract
Abstract
Purpose:
To evaluate characteristics of obstructions of the hepatic veins (HVs) in Chinese patients, technical aspects of puncture of the HVs, short- and mid-term outcomes, and complications of endovascular treatment.
Patients and Methods:
Forty-eight HV patients with different degrees of symptoms and signs of portal hypertension were enrolled in our study. Endovascular treatments with balloon and stents were performed. Catheter-directed thrombolysis (CDT) was performed in patients with thrombosis in the HVs. For patients with lesions of both the HVs and the inferior vena cava (IVC), balloon expansions or stenting were performed at the IVC lesions also.
Results:
Endovascular treatments were successful in 43 patients. The technically success rate was 89.6% (43/48). Fifteen patients underwent solely balloon expansions, 28 patients had balloon expansions and stentings, 5 patients underwent CDT, and 3 patients had implanted stents in the IVC lesions at the same time. The symptoms of portal hypertension were alleviated in 39 patients postoperatively. In the other 4 cases portal hypertension was mildly alleviated at discharge. Thirty-nine of the 43 patients were followed up for an average of 24±1.3 months (range, 6–62 months). Ascites were completely resolved in 32 cases, with a small amount of ascites in 4 patients and moderate to massive amounts in 3 patients. Hepatomegaly and splenomegaly completely disappeared in 30 patients and still could be touched in 6 patients. The HVs were patent in 29 patients. Restenosis and re-occlusion of the HVs appeared in 4 cases. All patients were successfully treated by endovascular treatments.
Conclusions:
Endovascular treatments for patients with obstruction of the HVs have a high technical success rate, fewer complications, and better short- and mid-term clinical outcome. The key to successful endovascular treatment is successful puncture of HVs. For patients who have occlusive lesions of HVs combined with occlusive IVC, recanalization of the lesions of the HVs could achieve good results.
Introduction
B
Patients and Methods
Patients
From June 2003 to June 2012, 48 patients (31 males and 17 females; 17–71 years of age; average age, 42±2.2 years) with HV occlusion were referred to our institution for endovascular treatment. The duration of disease ranged from 2 months to 20 years. The patients' major clinical symptoms and signs included ascites (45 cases), hepatomegaly (47 cases), splenomegaly (43 cases), abdominal distension (44 cases), abdominal varicose veins (21 cases), edema in the lower limbs (15 cases), skin pigmentation in the lower limbs (13 cases), and hematemesis (15 cases). Splenectomies and portoazygous disconnections were performed in 4 patients. There were 12 cases classified as Child–Pugh A, 26 as Child–Pugh B, and 10 as Child–Pugh C (Table 1).
SD, standard deviation.
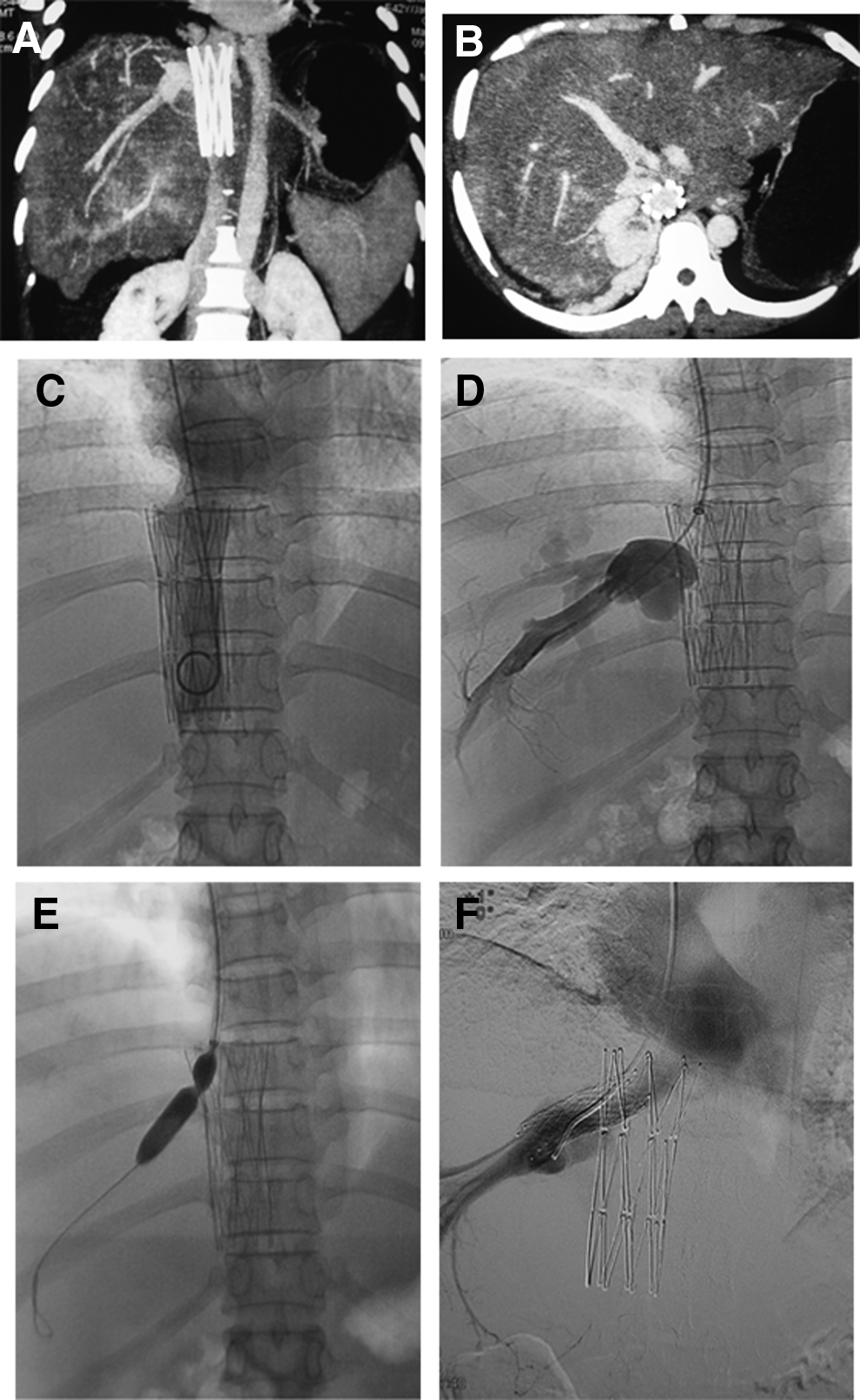
Before any endovascular procedures were performed, the HV and IVC lesions were evaluated by use of color Doppler, computed tomography angiography, magnetic resonance imaging, or venography. As listed in Table 2, all patients had HV occlusions: membranous (n=24) or segmental (n=14) in 38, thrombosis in 8, and HV occlusion caused by IVC stents in 2 (Fig. 1). Five patients had combined HV and IVC lesions: stenosis, membranous occlusion, short-segmental lesions (n=4), and long-segmental (>10 cm) occlusions (n=1) (Table 2).
IVC, inferior vena cava.
Endovascular procedure
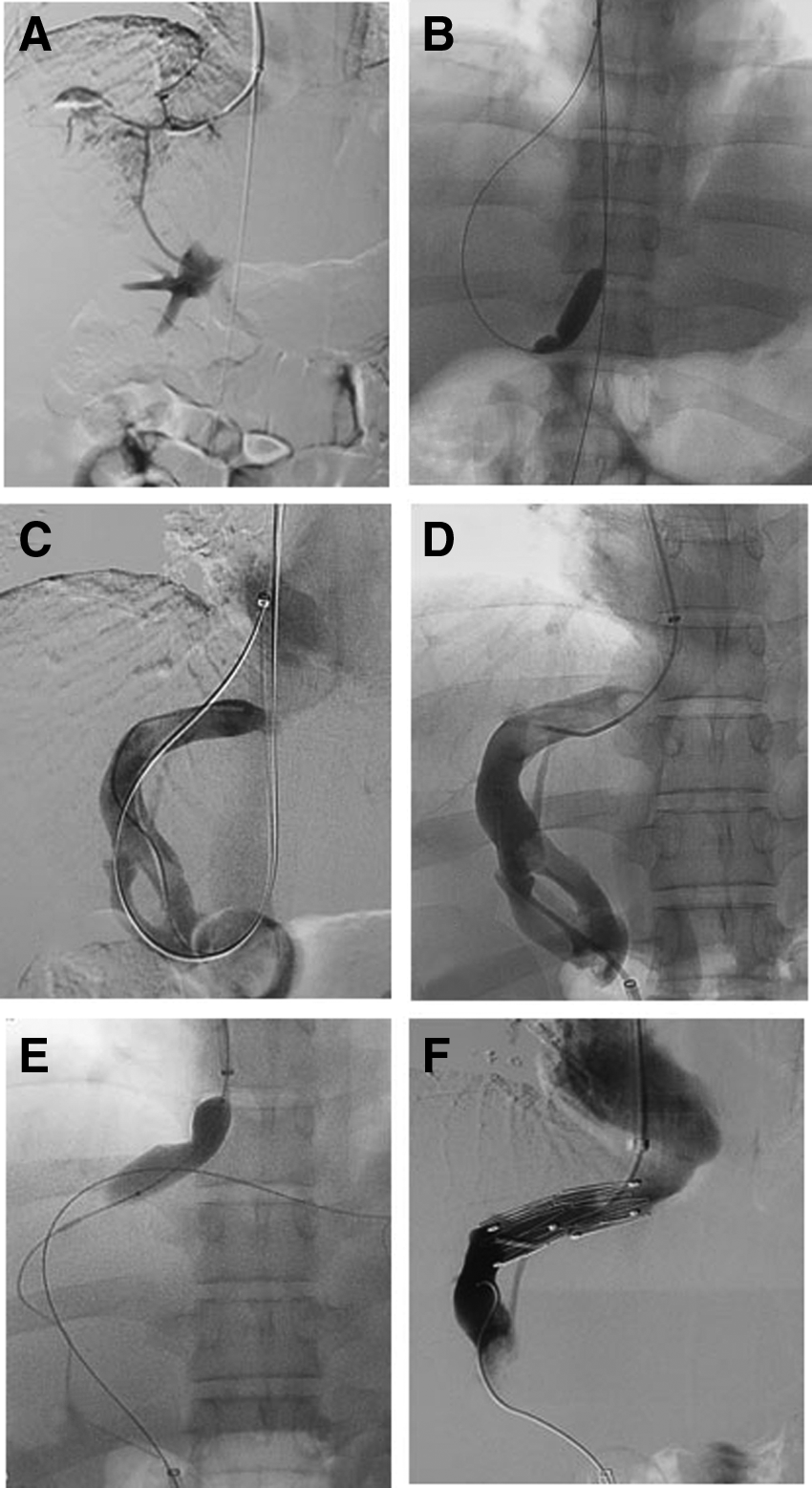
The endovascular procedures were performed in the angiography suite. All patients received local anesthesia, and puncture access of the right jugular vein and femoral vein was used. After the puncturing, a 5 French pigtail catheter was placed in the IVC. Patients were given intravenous heparin (100 units/kg). IVC venography was performed, and the images of the IVC and HVs were examined. HVs were punctured with a RUPS-100 needle (Rösch-Uchida USA; Cook, Bloomington, IN). Based on the preoperative computed tomography angiography or magnetic resonance imaging images, the direction of the needle was adjusted to puncture either the right or the left side of the IVC wall via the jugular vein approach; puncturing was repeated if necessary. If the occluded ostium of HVs could not be located by these measures, a catheter was placed in the accessory HV for venography. Because intrahepatic collateral vessels between the accessory HV and the HVs form and expand in BCS, the distal site of the HV occlusion could be seen clearly. The puncture could be performed through the jugular or the accessory HV approach, according to the finding on venography (Fig. 2).
After HV venography was performed, the lesions of the HVs were then dilated with a balloon catheter of 8–12 mm in diameter. For membranous lesions, if the HVs were well developed without residual stenosis evident by venography, the intrahepatic collateral was significantly reduced or disappeared after balloon expansion. We did not implant stents in patients with membranous lesions unless they had residual stenosis >50% after balloon expansion or had segmental or HV obstructions caused by IVC stents. The diameter of stents used varied from 12 mm to 18 mm, and the length ranged from 3 cm to 6 cm.
For patients with thrombosis in the trunk of the HVs, catheter-directed thrombolysis (CDT) was performed, with placement of a 4 French or 5 French unifuse catheter (AngioDynamics, Latham, NY) in the HVs and the injection of heparin saline and urokinase (300,000 units) at operation, followed by infusion of urokinase (600,000–800,000 units/day continuously). Balloon expansions or stent deployments were done 1–2 days after the catheter was placed, according to when the venography was performed (Fig. 3). For patients with combined HV lesions and IVC lesions, balloon expansions or stent deployments were performed at the same time. If the catheter or guidewire traversed the IVC lesions with difficulty, only the HV lesions through the jugular vein approach were addressed so as to reduce the portal hypertension; the IVC lesions were not treated.
Postoperatively, low-molecular-weight heparin (4000 units) was administered subcutaneously twice a day, and warfarin was taken orally once a day. When the international normalized ratio was stable at 2–2.5, the low-molecular-weight heparin was stopped, and warfarin was continued (for at least 3 months for patients with membranous or segmental occlusions and 6–12 months for patients with thrombosis).
Results
Endovascular treatment
Endovascular procedures were successfully performed in 43 of the 48 patients (89.6%) with HV lesions. In 5 patients (2 with segmental occlusions and 3 with thrombosis), the occlusive HV could not be found, and the procedure was abandoned. Fifteen patients were treated with balloon expansion only; 28 were treated with balloon expansions and stentings. Three of 5 patients diagnosed with both HV and IVC lesions had stents implanted in the IVC concurrently. Five patients underwent CDT (Table 3). There was no preoperative or postoperative mortality or cardiopulmonary complication during a 30-day follow-up. In 17 patients, stasis of intrahepatic contrast caused by the HV puncturing occurred, but in 15, the contrast had disappeared by the end of the treatment. In 2 patients, a right intrahepatic hematoma formed; one was absorbed by 5 days after treatment and the other within 15 days. At the time of discharge, the symptoms of portal hypertension were alleviated in 39 patients and were slightly improved in the other 4. The amount of ascites decreased, with an average abdominal circumference of 81.4±3.3 cm postoperatively compared with 87.3±4.5 cm preoperatively.
CDT, catheter-directed thrombolysis; IVC, inferior vena cava.
Follow-up results
The mean follow-up in the 39 of the 43 patients was 24±1.3 months (range, 6–62 months). Observation indicators included the symptoms and signs of portal hypertension and HV patency assessed by color Doppler. Ascites remained completely resolved in 32 patients, but a small amount persisted in 4 patients, and there were moderate to massive amounts in 3 patients. Hepatomegaly and splenomegaly completely disappeared in 30 patients, but the organs were still palpable in 6 patients.
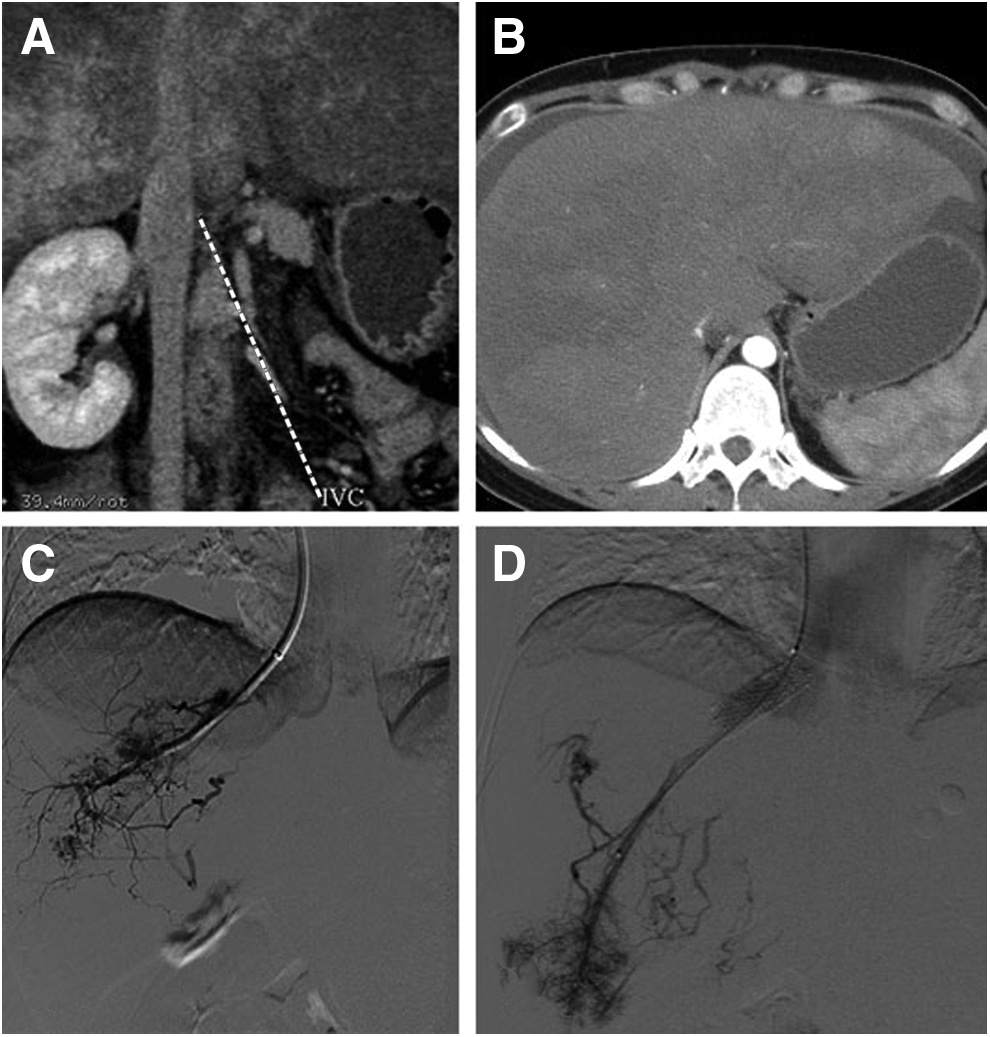
HV patency persisted in 31 patients, but restenosis and re-occlusion occurred in 4 patients. In 3 of the 4 patients, the stenoses were located in the HV's membranous occlusions, where only balloon expansions were performed. In the other patient, who originally had segmental stenosis, restenosis occurred after stenting. All four of the restenoses were successfully treated with balloon expansion and stenting. In 4 cases, the HV occlusions occurred after the initial stentings of the HVs' segmental occlusion. The 3 patients with re-occlusion underwent CDTs to remove the thrombi in the stents and were restented successfully. In the other cases, the occlusive stent was expanded with a balloon catheter (Fig. 4).
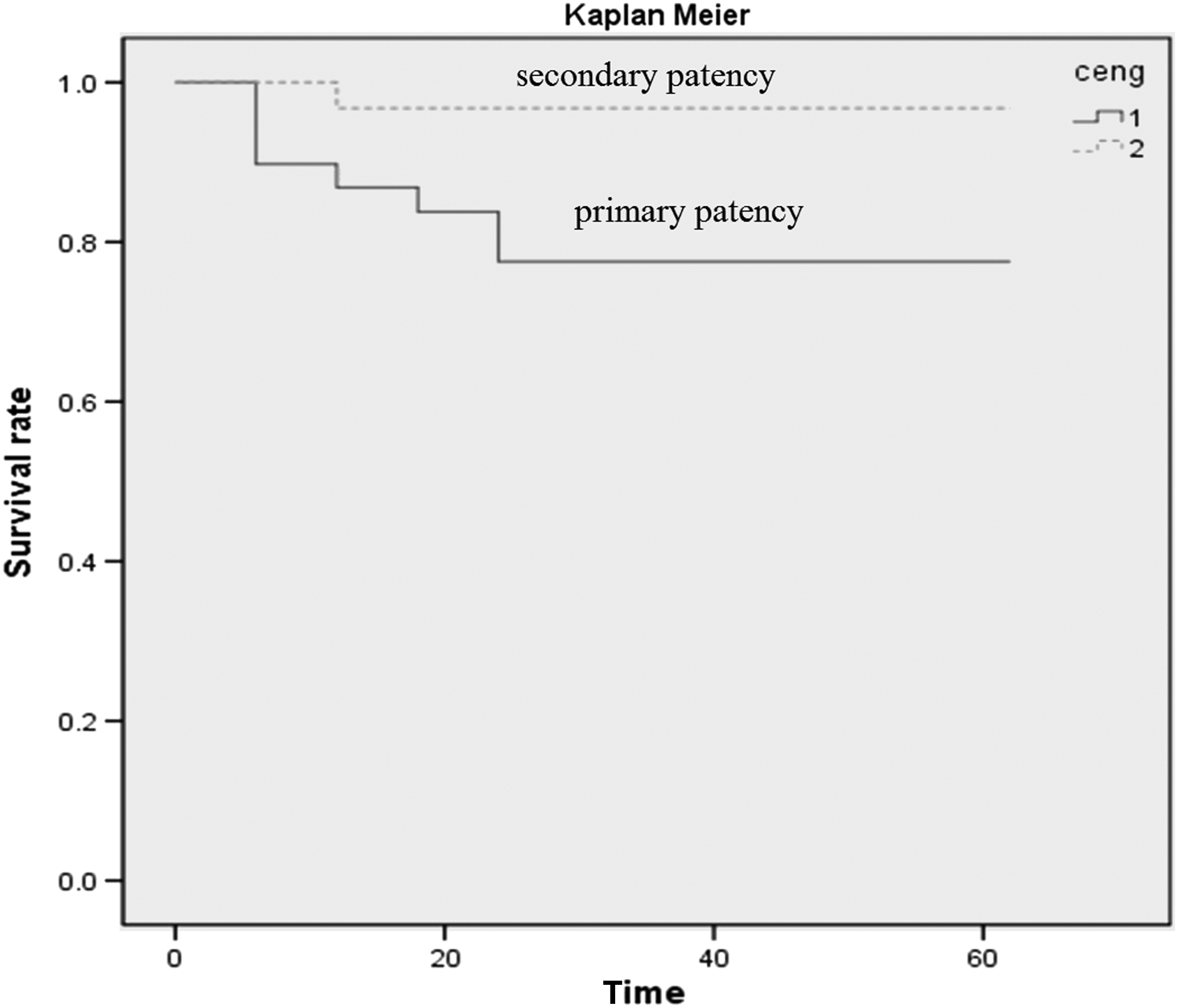
Hepatic vein patency survival curve using Kaplan–Meier analysis.
Discussion
The characteristics of HV occlusions in China
BCS is a rare disease. The cause of BCS is different in western and eastern countries. In the western world, thrombosis of the HVs is the most common cause, and most patients have an underlying condition that predisposes to blood clotting, such as myeloproliferative diseases, gene mutation of factor V Leiden or factor II, lower levels of proteins C or S or antithrombin III, use of oral contraceptives, or paroxysmal nocturnal hemoglobinuria or Behcet's disease.7,8 In contrast, membranous obstruction of the IVC or HVs is more common in the East.6,7 The cause of membranous occlusions is not clear. Some scholars think the condition is congenital in origin, but the others disagree. Zhang et al., 6 for example, considered that membranous occlusions could occur during adulthood. In a retrospective study of 42 BCS cases, they found that almost all patients with membranous lesions were more than 20 years old, with an average age of 33 years. Furthermore, they found 2 recurrent cases of BCS in which newly formed membrane was detected within the IVC, although it had not been observed during surgery 1 year earlier. From these observations, they considered membranous obstruction of the IVC or HVs to be a sequel of thrombosis 6 ; however, other authors considered it to be associated with infection. 9
We have found that the number of cases of obstruction of the HVs in China is increasing, perhaps because of the increased use of imaging examinations. In our experience, the majority of the HV lesions are membranous or segmental obstructions, but the cases of thrombosis of HVs has increased. In contrast to membrane-type BSC, 6 thrombosis-type BSC occurs diffusedly in China without a characteristic geographic distribution. Additionally, BSC in China is different from BSC in the western countries in its etiology, which may present with different disease onset, imaging findings, and therapeutics. For example, the onset of thrombosis in hepatic veins is relatively acute, whereas the onset in membranous or segmental obstruction is subacute or chronic.
Imaging plays an important role both in making the diagnosis as well as in the assessment of related complications of BCS. In contrast to thrombosis in the HVs, in which there is lack of blood flow, the presence of thrombus, and nonvisualization within the HVs, 10 in membranous or segmental occlusions there is enlargement of the far block segments of hepatic veins, blood stasis, and reverse blood flow. Both thrombosis and membranous and segmental occlusions have collateral hepatic venous circulation, enlargement of the caudate lobe, and IVC compression. However, the membranous or fibrous lesions usually are not detectable by computed tomography or Doppler ultrasonography.
Restoring HV blood flow is the most important goal in the treatment of BCS. With the development of interventional technologies, endovascular treatment is used to analyze the occluded HVs and has been considered as a main therapeutic choice.4–6,11 Transjugular intrahepatic portosystemic shunt is now the most common intervention for BCS in European centers 11 because the HV obstruction usually is extensive. Transjugular intrahepatic portosystemic shunt is effective in the majority of cases, except possibly in those with the most severe liver failure. In China, however, balloon dilatation or stent insertion to recanalize the occlusive HVs is still the most common intervention because membranous or segmental occlusion is so common.
HV puncture
The main objective of endovascular treatment for BCS with occlusion of the HVs is to successfully puncture the HVs. When the HVs are occluded, the hepatic venous pressure increases, causing the collateral branches to contract and the anatomical abnormality of collateral branches of intrahepatic vessels. Therefore, it is especially important to evaluate the position and nature of the HV's obstruction and intrahepatic venous drainage with preoperative imaging. In patients with membranous occlusion of HVs, preoperative images often show that the distal HVs are enlarged. On intraoperative images, the membrane may be found to bulge into the lumen of the IVC because of HV hypertension. This feature can be used as the site to puncture the HVs. For segmental occlusions with residual stump of the HV's outflow, the sheath of the RUPS-100 needle is placed in the stump, and the occluded segment can be successfully punctured. For segmental occlusions without a residual stump of the HV, the directions of the HVs could be judged according to the preoperative images. Puncturing the occlusive HVs with a RUPS-100 needle involved withdrawing the needle stylet and adjusting the direction of the needle carefully when it was inserted into the liver parenchyma 1–2 cm.
For patients without opening stump of the HV, it might be difficult to locate the HV in the operation. We attempted to puncture the HV through the liver parenchyma about 1–2 cm below the surface. We determined if the needle was placed within the vessel by pulling the needle out of the sheath. If blood flowed out, we then proved the needle was placed correctly within one branch of HVs. Subsequent contrast imaging helped us adjust the needle to inside of the main trunk of HVs. If there was blood flowing from the sheath, venography was needed to confirm what the needle was in the main trunk of HV or in the branch. A guidewire was exchanged for further balloon expansion or stent when the needle was in the trunk. If the needle was in a branch, we observed the direction of the occlusive trunk of HVs and then adjusted the angle and the direction of the needle for a secondary puncture.
If the accessory HV is patent, the catheter could be placed into it, and then venography could be performed. Because of the intrahepatic collateral vessels expanding between the accessory HV and the HVs, the distal position of the occluded HVs could be identified clearly, after which we could puncture the HVs through the jugular or the accessory HV approach.
In our study, HVs puncture was performed successfully using the methods above in 43 patients but, unfortunately, not in all patients. In 5 patients, endoluminal therapy failed, and a surgical shunt had to be was performed.
Treatment for patients combined with the IVC lesions
In China, BCS with HV obstruction complicated with IVC lesions is common. This situation is difficult to treat, especially if there is long-segmental occlusion in the IVC. For this condition, the major goal of treatment still is to reduce the hepatic or portal hypertension. Although membranous and short-segmental lesions may be treated by endovascular approaches means, consistent with previous reports by other investigators,12,13 we found long-segmental lesions were hard to traverse using endovascular techniques, and even if they can be treated, they may re-occlude soon. We found that most of the patients with combined HV occlusion and IVC occlusion had only membranous or short-segmental occlusive lesions of the HVs. When it was hard to get through the long-segmental lesions, we only treated lesions of the HVs endovascularly in order to alleviate the congestion of the liver, reduce the hypertension of the hepatic and portal veins, and restore the liver function.
Complications and short- and mid-term efficacy
Some reports 6 have shown that the HV pressure could be reduced by about 25%–50% after successful endovascular recanalization of the HVs. The 5-year survival rate in patients with mild disease could reach l00%. For patients with disease, the survival rates at 1 or 5 years were up to 85% (65%–100%) and 77% (53%–100%), respectively.14,15 For patients with two to three HV obstructions, one HV (diameter >10 mm, especially the right HV) was recanalized, which could often result in a better treatment effect. 16 In our study, the immediate HV pressure dropped approximately 37% postoperatively in successful treatment of the 43 cases. We only recanalized one HV (mainly the right hepatic vein), which was successful in all cases. During the follow-up, the symptoms and signs of portal hypertension were alleviated in patients, and there were no deaths.
The reported common complications of endovascular treatment of BCS have included hepatic encephalopathy, bleeding into the abdominal cavity or biliary tract bleeding, hepatic artery injury, and others. The reported overall incidence has been less than 3%, and the mortality rate was about l%. 17 In our series, no serious complications occurred. Two intrahepatic hematomas due to puncture of the HVs were found, but they spontaneously resorbed. The incidences of restenosis after balloon expansion and stenting of the HVs were about 10%–20% and 10%, respectively. 17 Restenosis was more likely to happen in the segmental lesions than in membranous lesions and usually occurred in 3–12 months postoperatively. Most restenoses could be treated by endovascular treatment, such as catheter thrombolysis, iterative balloon expansion, or stenting. If these measures fail, conventional surgery should be considered.
In conclusion, endovascular treatment in BCS with HV obstruction had a high technical success rate, with few complications and favorable short-term and mid-term outcomes. The key to successful endovascular treatment is successful puncture of the HVs.
Footnotes
Disclosure Statement
No competing financial interests exist.
Both authors shared in conception and design, analysis and interpretation, data collection, writing the article, and critical revision of the article.