
Abstract
Abstract
Aim:
Natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) is a new approach that allows surgical manipulations and specimen extractions through the natural orifices such as the vagina. There have been limited numbers of cases about the adaptation of NOTES for ventral hernia repairs. Here, we aimed to present two more cases and highlight our technical differences compared with the previously reported instances.
Patients and Methods:
Two patients (43 and 46 years old; body mass index of 29 and 30 kg/m2, respectively) were treated with hybrid transvaginal incisional hernia repairs. Two 5-mm abdominal trocars were used to monitor transvaginal access, adhesiolysis, dissection of the hernia, and tuckering of the mesh. A 15-mm transvaginal trocar was used for scope and mesh introduction into the abdomen. Defects were 3–5 cm in diameter.
Results:
A rigid 5-mm laparoscope was used. The composite synthetic meshes were, respectively, 11 and 13 cm in diameter. These were passed through the vagina without any protection such as a bag or sheath. No conversion or additional port was required. Respective operative times were 120 and 180 minutes, and the patients were discharged uneventfully on the second day. One patient had seroma, which was managed conservatively (aspiration of 20 mL on Day 7). There were no recurrences after 7 and 13 months, respectively.
Conclusions:
Conventional laparoscopic equipment can be used for hybrid transvaginal incisional hernia repair. An anti-adhesive synthetic mesh can be inserted through the vaginal trocar without protective devices. The main advantage of this technique is to avoid 10–15-mm abdominal trocars, which increase the risk of trocar-site hernias themselves.
Introduction
T
Natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) is a new minimally invasive surgery concept. Its potential benefits over conventional laparoscopic surgery are fewer surgical-site complications, less postoperative pain, and faster recovery. Transvaginal access, one of the routes of NOTES, has the general advantages of laparoscopic surgery and also avoids the need for 10–15-mm trocars in the abdominal wall. Despite the theoretical benefits of transvaginal repair of ventral hernias, related studies in the medical literature have so far been very limited,6–9 with only a total of 13 patients published. Here we aimed to present 2 more cases and highlight our technical differences compared with those previously reported.
Patients and Methods
We enrolled 2 female patients with incisional hernias for a transvaginal hernia repair in 2013. The details of this new technique were explained to both patients, and the appropriate consent was obtained. Prophylactic intravenous antibiotics were administered 1 hour prior to the operation and postoperatively for 2 days.
Surgical technique
The patients were placed in the lithotomy position with a 30° head-down tilt, and the abdomen was thoroughly sterilized and draped. A laparoscopic monitor was kept on the left shoulder side of the patient, whereas the other laparoscopic monitor was placed on the right side of the patient. The operating surgeon sat in between the patient's legs or on the left side of patient, while the assistant surgeon and scrub nurse stood on either side. With the patient under general anesthesia, a urinary bladder catheter and a nasogastric tube were also inserted. Pneumoperitoneum was created via a Veress needle in the left upper quadrant. Two transabdominal trocars, both 5 mm in diameter, were inserted in the left and right lumbal areas. Transabdominal exploration was conducted using a 5-mm rigid laparoscope. Sterilization of vaginal cavity was performed with a 10% povidone–iodine solution. The cervix was then sequentially dilated, and a uterine sound was placed to move the uterus anteriorly. After a clear visualization of the cul-de-sac, a 15-mm trocar was placed through the posterior fornix under laparoscopic view (Fig. 1a). The laparoscope was passed to the transvaginal trocar (Fig. 2). Adhesions were then released via both abdominal trocars using scissors or a LigaSure™ vessel sealing system (Covidien, Mansfield, MA) (Fig. 1b). After complete adhesiolysis around the hernia, the defect size was measured with the help of an endoscopic grasper (Fig. 3). A circular-shaped synthetic mesh (Parietex™ composite; Covidien) was prepared; its diameter was designed to add 8 cm to the defect size, and it was rolled for abdominal insertion. The mesh was placed into the abdomen through the vaginal trocar, and no bag was used to transfer the mesh (Fig. 1c). The mesh was fixed over the defect through overlapping by 4 cm using tackers (Fig. 1d). Mesh fixation was completed by contralateral introduction of the tacker (Fig. 1e). No suture fixation was done. The colpotomy incision was closed with a running absorbable suture, and the avoidance of sexual intercourse for 1 month was advised.


Transvaginal view of the abdomen and the hernia defect.
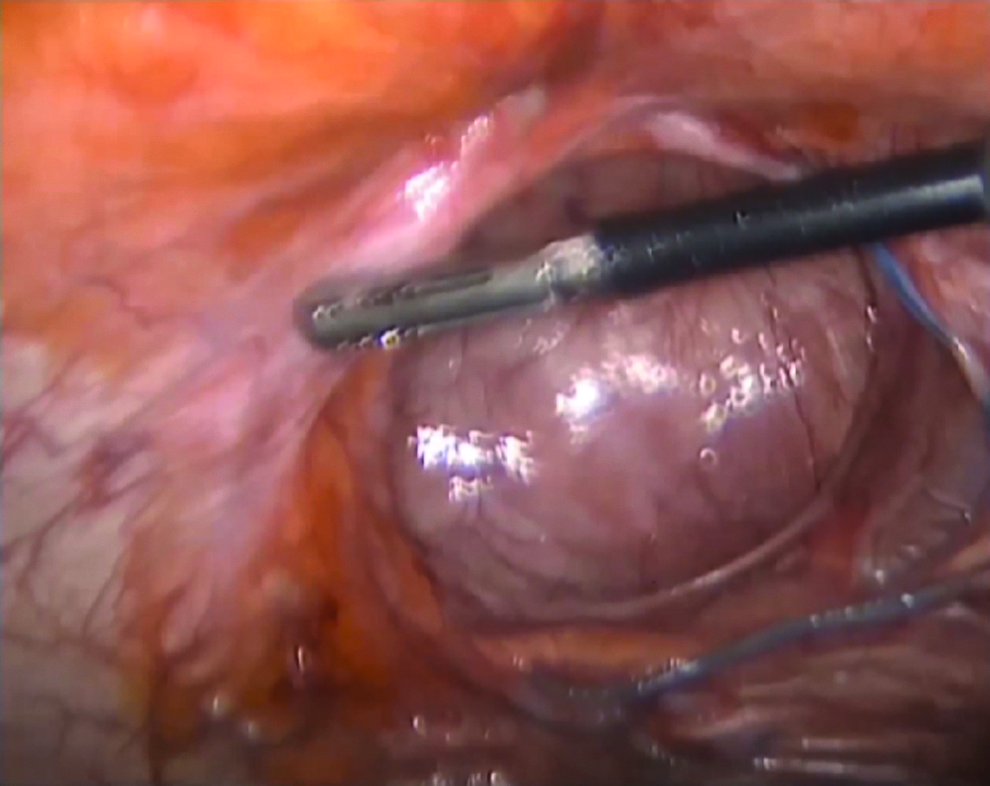
Transvaginal view of the hernia and measurement of the defect size.
Patient 1
A 46-year-old female patient was admitted for an incisional hernia with recurrent abdominal pain. The patient denied any intestinal obstructive signs or symptoms. Her body mass index was 30 kg/m2. Her medical and surgical history included an open Roux-en-Y gastric bypass for obesity 2.5 years ago. She had a 5-cm midline abdominal fascial defect. We used a 13-×13-cm mesh. The operative time was 180 minutes, and 2 days after surgery she was discharged uneventfully. One week after surgery, she had seroma, and 20 mL of serous liquid was aspirated. There was no recurrence after a 13-month follow-up.
Patient 2
A 43-year-old female patient had an open Roux-en-Y gastric bypass and umbilical hernia surgery at the same time 1.5 years ago. Her body mass index was 29 kg/m2 at the time. There were no signs of incarceration of the hernia. Her upper midline hernia was 3 cm in size, and it was repaired using a 11-×11-cm mesh. The operating time was 120 minutes. The postoperative course was uneventful, and she was discharged on Day 2. There was no recurrence after a 7-month follow-up.
Discussion
Here, we described transvaginal hybrid NOTES for two incisional hernia repairs. Unlike the previously reported cases, we did not use biological meshes, flexible endoscopes, sterile sheaths, or bags to protect the mesh during its abdominal introduction. Using a standard composite mesh, a rigid telescope and direct placement of the rolled mesh into the abdominal cavity through the vaginal trocar made the procedure very similar to the well-known laparoscopic ventral hernia repair process. The main advantage of this technique was that it avoids penetration of the abdominal wall with 10–15-mm trocars, which itself carries the increased risk of a trocar-site hernia.
There are concerns regarding infection with transvaginal delivery of the mesh. Although we did not obtain any intraperitoneal cultures after mesh insertion, no clinical infections were encountered in our patients. The bacterial flora of the vaginal canal can vary among individual women, and it is related to their menstrual cycle as well. Lactobacilli are the primary vaginal flora in a healthy woman; however, other normal or pathogenic organisms can also be present. 10 There have been two experimental (porcine) studies about the risk of infections in transvaginal ventral hernia repairs.11,12 Lomanto et al. 11 put the mesh in the abdomen through the vagina using a sterile plastic bag and found no contamination in 5 subjects. Powell et al. 12 placed a mesh without protection in 7 subjects, and 5 animals had positive mesh cultures. The first human case of transvaginal incisional hernia repair was demonstrated by Jacobsen et al. 13 using a biologic mesh, which was a well-established biological material for reconstruction in contaminated areas. 14 They did not use any bag during the passage of the mesh through the transvaginal trocar. After a 12-month follow-up, there was no evidence of mesh infection or recurrence.8,13 Wood et al. 7 reported six transvaginal ventral hernia repairs with synthetic meshes. For sterile insertion of the meshes, the authors placed them in protective bags, and no clinical infections were encountered. Bruna et al. 6 reported a single case of a transvaginal ventral hernia repair with a synthetic mesh, and the authors only protected the transvaginal trocar with a sterile plastic sheath and no bag. The postoperative course was uneventful, and the patient was asymptomatic 1 month later. Recently, an interesting study has demonstrated that a surgically prepped vaginal canal can be a sterile conduit for the insertion of a polypropylene mesh for transvaginal ventral hernia repair without the use of additional mesh protection. 10 Surprisingly, the prepped vaginal conduit in those patients was found to be more sterile than a prepped skin incision. In summary, some authors preferred infection-resistant meshes 13 or synthetic meshes with extra protection such as vaginal trocar protection 6 or sterile bags for meshes. 7 However, there has been no evidence that these precautions are necessary for mesh-related infections. We preferred synthetic meshes rather than biological ones. Moreover, we did not use any sterile sheaths for transvaginal trocar or sterile bags for meshes. Although we had a limited number of cases, there were no infections or recurrences in our experience.
We observed that some authors preferred flexible endoscopes 8 as opposed to other rigid laparoscopes. We believe that flexible endoscopes are not mandatory for all transvaginal surgical approaches. They can be used in certain complicated cases or in cases when the rigid telescope does not provide a sufficient outlook. Some authors reported longer trocars for vaginal access. 6 We used standard-length trocars in both cases for abdominal or vaginal accesses. It is possible that a longer trocar for the vagina provides some comfort, but it is not a rule for transvaginal surgery. There is also a debate about pure or hybrid NOTES procedures. We believe that hybrid transvaginal incisional hernia repairs are superior to the pure transvaginal approach. First of all, the hybrid approach provides a safer trocar insertion through the vagina under direct visualization. Blind access through the vagina for incisional hernia repair may increase the risk of intraabdominal injuries due to previous surgeries. Tables 1 and 2 demonstrate that there was no access injury in the hybrid cases, in contrast to purely transvaginal cases. Wood et al. 7 reported their experience with 6 cases of pure transvaginal incisional hernia repairs, and they found a full-thickness high rectal injury during direct vaginal access without laparoscopic assistance. Second, lysis of the adhesions with unidirected equipment can result in technical difficulties. One or two oppositely placed 5-mm ports can provide retraction and assistance with dissection without adding a significant disadvantage to minimally invasive surgery. Lastly, two 5-mm trocars placed in opposite areas of the abdomen make the mesh fixation easier and more effective by tuckering from one side to the other side of the mesh. Put simply, our procedures were performed using standard laparoscopic instruments without any technical difficulty in both cases.
Data are mean (range) values.
BMI, body mass index; NA, not available; SILS, single-incision laparoscopic surgery.
Data are mean (range) values.
Data are median (range) values.
Conv, conversion to open or conventional laparoscopy; NA, not available; Rec, recurrence.
Patient selection for transvaginal incisional hernia repairs can be necessary, particularly at the beginning of the program. Very large defects or hernias near the pelvis may create difficulties for visualization, dissection, and mesh fixation. Small- or medium-sized defects, particularly those located at the middle or upper part of the abdomen, appear to be more suitable for transvaginal ventral hernia repairs. Obesity alone cannot be a contraindication for transvaginal incisional hernia repairs, but the feasibility and safety of this procedure for morbidly obese patients are not yet clear. Better cosmesis and lower postoperative pain are advocated by supporters of NOTES as benefits compared with conventional laparoscopy. Although we did not conduct any postoperative pain scoring, we can say that our procedures were similarly painful for our patients, who had previously undergone conventional laparoscopic incisional hernia repairs. According to our research, better cosmesis for incisional hernia repair through a transvaginal approach instead of conventional laparoscopic repair has no clear advantage.
As a conclusion, conventional laparoscopic equipment can be used for hybrid transvaginal incisional hernia repairs. An anti-adhesive synthetic mesh can be inserted through the vaginal trocar without protective devices. The main advantage of this technique is that it avoids 10–15-mm abdominal trocars, which increase the risk of trocar-site hernias themselves.
Footnotes
Disclosure Statement
No competing financial interests exist.