
Abstract
Abstract
Objective:
Natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) has generated excitement among surgeons as potentially scar-free surgery. We developed this technique while taking into consideration that it could also be applied to transoral thyroid surgery.
Patient and Methods:
We report the case of a 35-year-old woman with a 0.5×0.5-cm papillary thyroid microcarcinoma. We implemented a modified approach for the removal of the thyroid by using a frenotomy incision of the mouth, accompanied by an endoscope system.
Results:
A modified approach for the removal of the thyroid was used on the patient. The total operating time was 120 minutes, and there were no specific complications. The patient continues to be free of any diseases 12 months after the excision.
Conclusions:
Thyroidectomy can be performed by a transoral endoscope-assisted approach through a frenotomy incision of the mouth. We describe the detailed procedures for an endoscope-assisted transoral thyroidectomy using a frenotomy incision.
Introduction
T
Considering that most patients who undergo surgical resection are women, it is desirable to develop a surgical technique for the removal of papillary thyroid microcarcinoma (PTMC) without producing external scarring of the neck. Thanks to advancements in medical technology, we were able to develop a modified approach in which a frenotomy incision of the mouth was endoscope-assisted.17–21 This modified method allowed for the reduction of risks of damaging the mouth floor structures (mental nerve, salivary gland, etc.) because we used an anatomical dehiscence from the frenotomy incision.17–21
Recently, natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) has generated excitement among surgeons as potentially scar-free surgery. We developed this technique and applied it to several surgeries.17–21 In this report, we describe this new technique in detail, as well as the surgical outcomes.
Patient and Methods
A 35-year-old female patient was admitted with PTMC, which had been detected 2 months earlier during a regular health checkup and by aspiration cytology. The PTMC was 0.5×0.5 cm in diameter under ultrasonography and located in the right thyroid gland (Fig. 1). The medical history of the patient was unremarkable, and she had no history of thyroid disease. The thyroid function tested normal. The patient was a young woman, and she did not want a surgical scar to remain in the neck area. Therefore, the surgery was performed through a transoral approach using an endoscope.
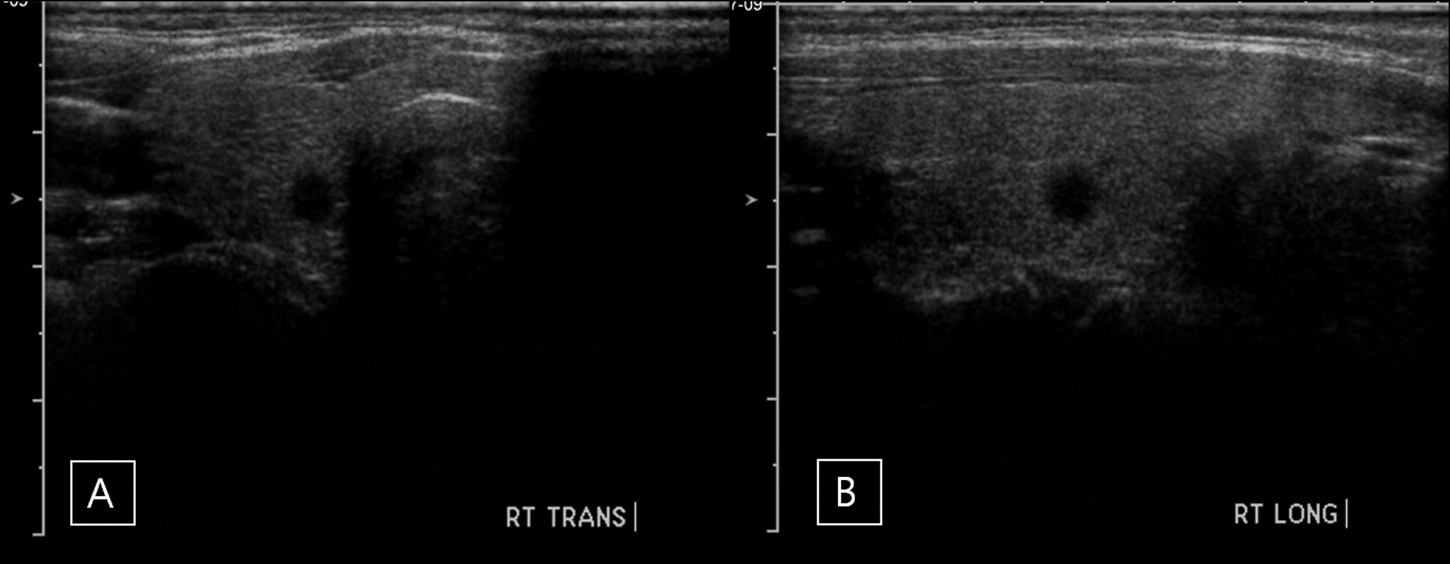
The papillary thyroid microcarcinoma was 0.5×0.5 cm in diameter under ultrasonography, located in the right thyroid gland:
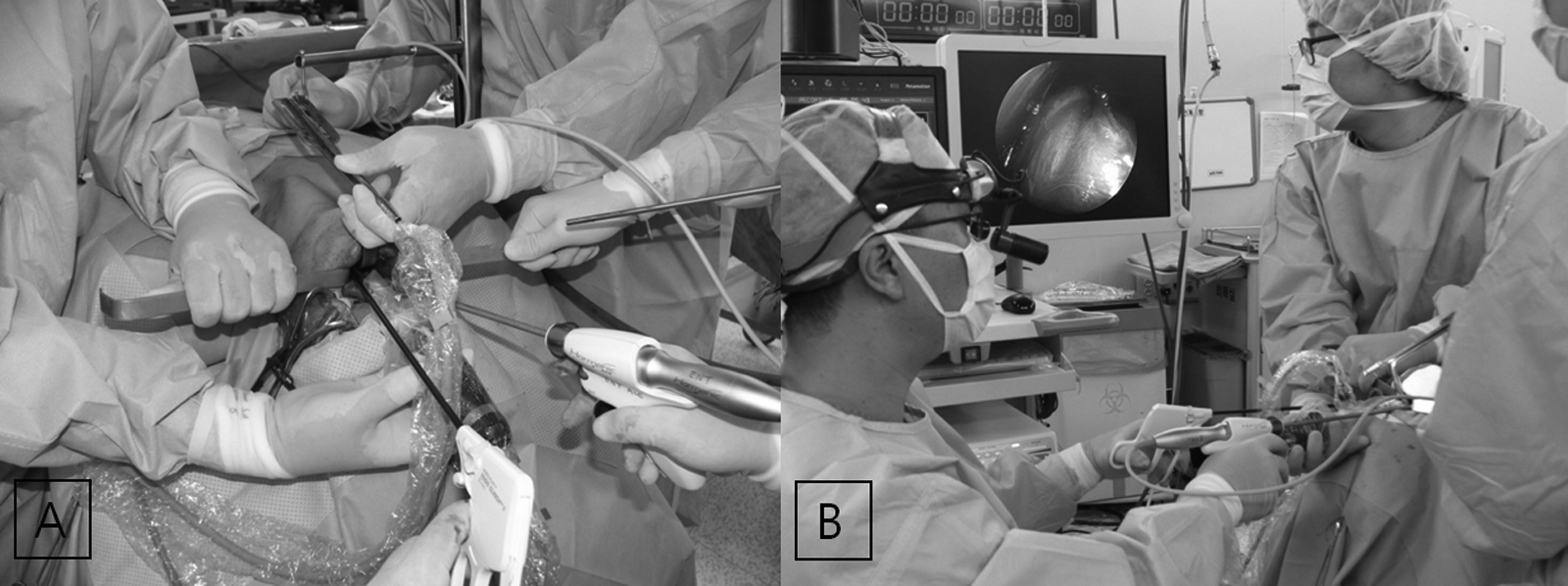
With the patient under general anesthesia, the mouth was opened, and the tongue was held in the upper position. An incision approximately 3 cm long was made in the oral mucosa, which included the frenulum. After careful dissection of the soft tissue at the floor of the mouth, we found the genioglossus muscles. We separated the muscles at the midline and retracted them bilaterally. These procedures were performed with the aid of a videoscope (HD EndoEYE laparothoracic videoscope; Olympus, Tokyo, Japan), two Sofield retractors (Zimmer, Inc., Minneapolis, MN), one self-retractor, and three assist operators (Fig. 2).
After the retraction of the genioglossus muscles, we found the hyoid bone. We transected the hyoid bone with an Osteo Punch Rongeur (1 mm, 40°; Koros USA, Inc., Moorpark, CA). Then, the hyoid bone was retracted bilaterally, and from there we went downward and were able to identify the thyroid (Fig. 3A).
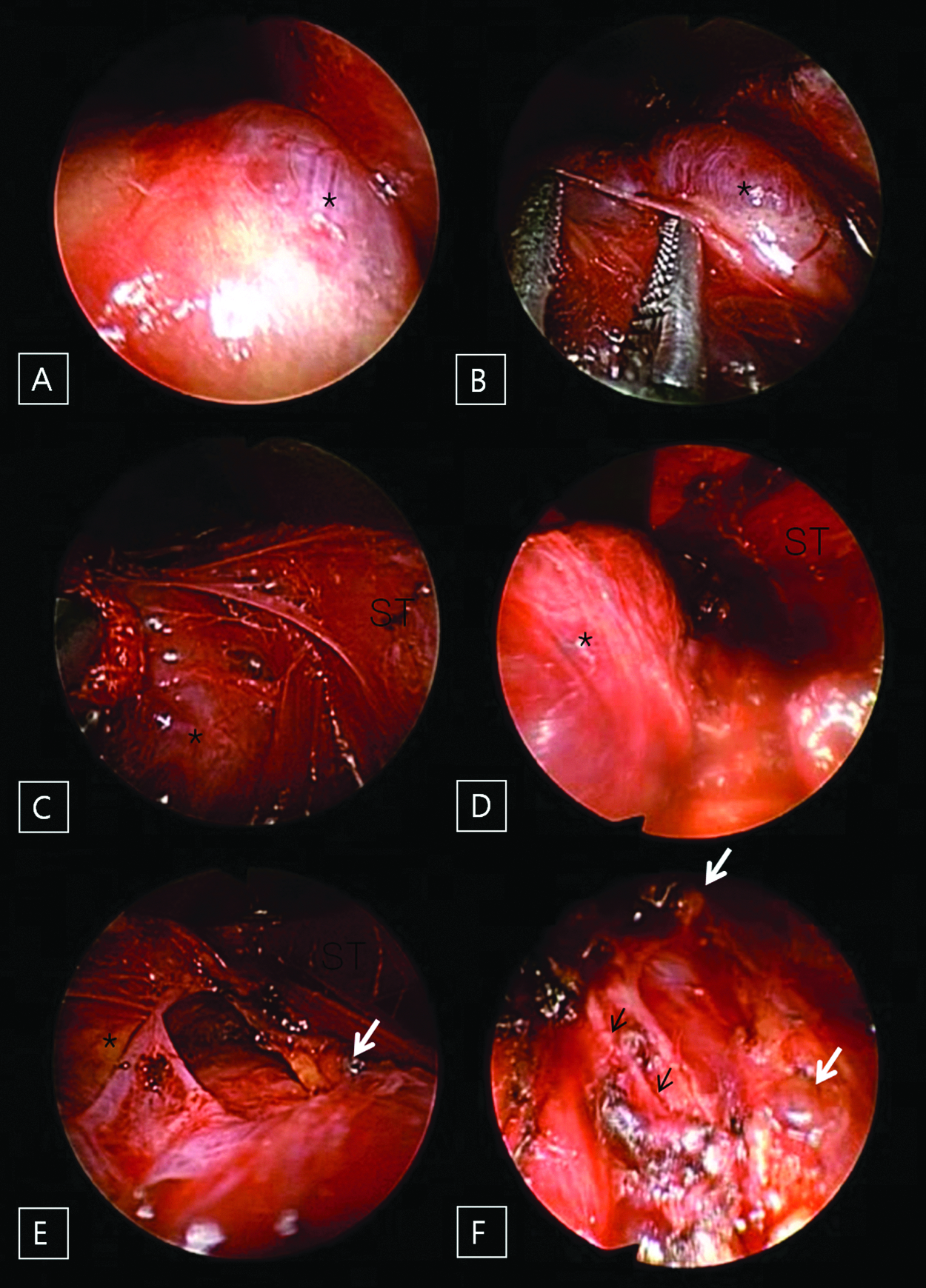
After these procedures, the right thyroid was found, and the upper pole was easily dissected from the trachea with an endoscopic dissector (Aesculap, Inc., Center Valley, PA) and ultrasonic scissors (Harmonic® scalpel 300; Ethicon, a Johnson & Johnson Company, Cincinnati, OH) (Fig. 3B). After that, the lateral portion of the thyroid was dissected from the strap muscle with a peanut dissector (a cotton ball was grasped by the endoscopic dissector) and full exposure of the upper and lateral thyroid (Fig. 3C and D). The inferior thyroid vessel was identified and dissected with the Harmonic scalpel (Fig. 3E). Finally, the right thyroid was dissected, the upper and lower parathyroids were saved, the inferior thyroid artery was sealed, and the recurrent laryngeal nerve was left intact (Fig. 3F).
In the operating room, we checked the frozen biopsy specimen, and the results indicated a thyroid papillary carcinoma with no capsular invasion. Afterward, the operation field was irrigated. A drain was inserted through the floor of the mouth, and it was sutured to the edge of the lower teeth (Fig. 4A). Then, the genioglossus muscles were sutured with 4-0 polyglactin 910 (Vicryl™; Ethicon), followed by suturing of the opened oral mucosa. The total operation time was approximately 120 minutes. After surgery, the drain was checked by chest X-ray (Fig. 4B). The drain was removed on postoperative Day 3 (Fig. 4C). We encouraged frequent oral gargling with 0.02% chlorhexidine and allowed for a normal diet on postoperative Day 3. The patient was discharged on postoperative Day 7.
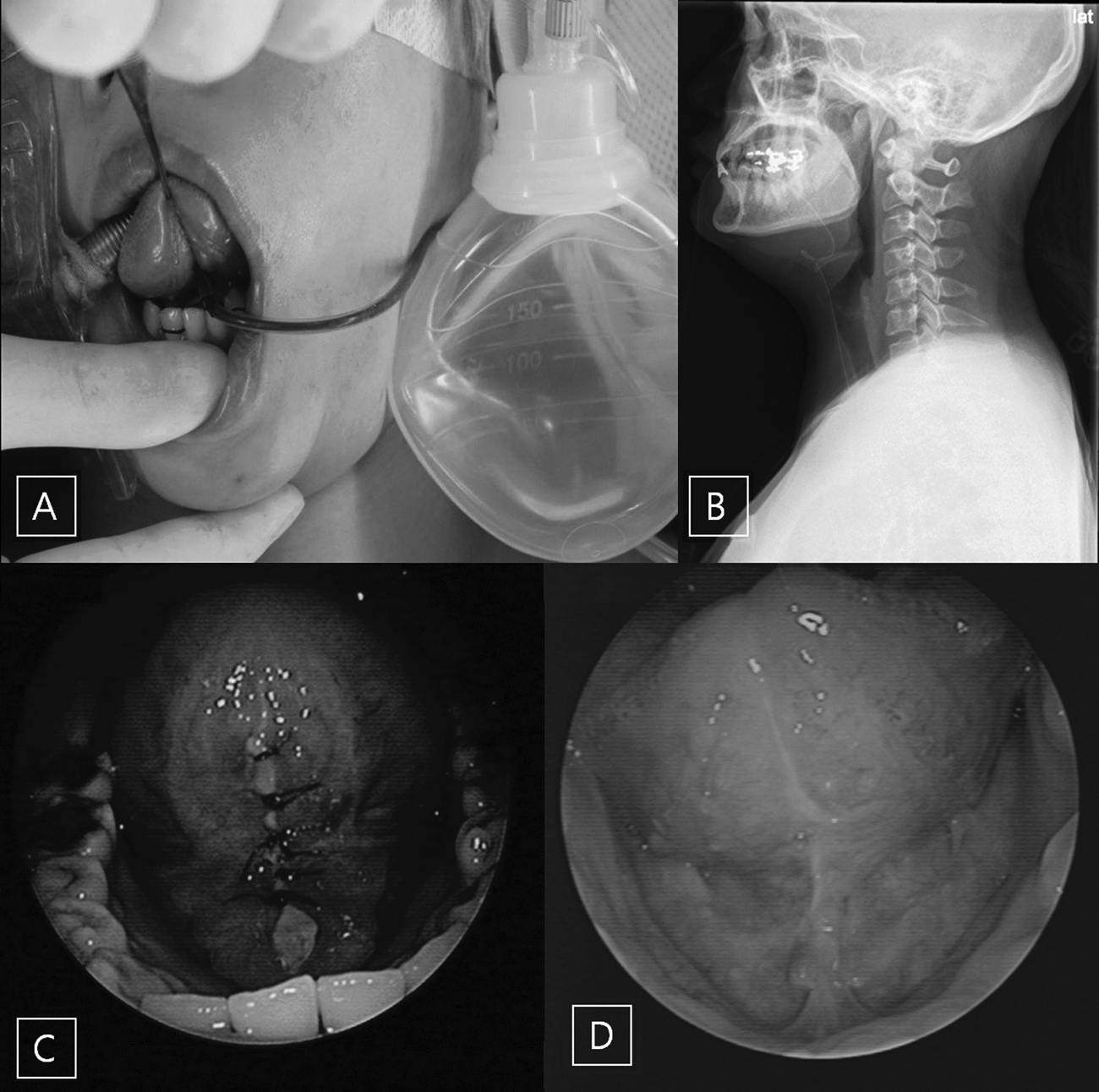
Twelve months have passed since the operation, and there have been no special findings of complications in thyroid function, vocal cord function, articulation, or tongue movement. The operation wound is clear (Fig. 4D). The patient is currently under follow-up observations at our outpatient clinic. She was quite satisfied with the surgical outcome.
Discussion
NOTES is considered a refinement of minimally invasive procedures, and this new technique is gaining increasing interest because it allows surgical treatment without any incision of the skin.22–24 NOTES has attracted the attention of many study groups from different scientific and medical fields. 24
Traditional thyroid surgery requires a transcervical approach, which results in external scarring of the neck.17–21,24 Considering the embryological development of the thyroid, it seemed obvious to us that an entirely transoral access to the thyroid region could be available.22,24 During its descent, the thyroid gland, which originates from the bottom of the tongue, is connected to the tongue through the thyroglossal duct. The thyroglossal duct is located behind the strap muscles of the neck and the hyoid bone and may either persist postpartum or result in the so-called pyramidal lobe in up to 30% of cases.24–26
Following this naturally predetermined access alongside the thyroglossal duct, we were able to develop a new surgical approach to the thyroid region. In previous studies, we reported the safe excision of dermoid cysts, thyroglossal duct cysts, and ectopic thyroid tissues through a transoral approach with a frenotomy incision.17–21 This approach showed that a transoral approach with a frenotomy incision was technically feasible, which allowed us to reach the upper thyroid gland without major tissue damage or bleeding.
This surgical approach passed through a midline incision at the floor of the mouth and used the natural midline dehiscence present between the genioglossus muscles.17–21 This area has been shown to be a relatively avascular dissection plane. When the space between the genioglossus muscles was spread out using a tractor, the mylohyoid muscle was reached. When we traced the posterior line of the mylohyoid muscle, the hyoid bone was reached.
When we reached the hyoid bone, we resected the middle portion of the hyoid bone (0.5 cm in width). We then went downward and were able to identify the thyroid isthmus and both thyroid lobes. After identification, we were able to find the thyroid and resect the thyroid. The patient was quite satisfied with the surgical outcome.
The satisfaction level of our patient, after the operation, was good, and significant swelling or bleeding was not observed. Because neck exploration creates the possibility of turning an aseptic operation into a potentially infectious surgical intervention through the spread of pathogenic germs from the oral microflora, infections following any operation must be managed carefully. However, one experimental report found that the microbiologic swab analysis of each operative field showed no signs of bacterial contamination and no signs of infection. 22 Therefore, we used antibiotics and an oral gargle, and the drain was removed 2 days after the operation. Follow-up observations were carried out for 12 months after the operation, and there were no recurrences or complication patterns observed.
This report suggests a new surgical method to approach the thyroid through the floor of the mouth. Therefore, it allows for the possibility of thyroidectomy through an intraoral approach.
Footnotes
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Science, ICT, and Future Planning (grant 2013R1A1A1012542).
Disclosure Statement
No competing financial interests exist.