
Abstract
Abstract
Laparoscopic surgery combined with natural orifice specimen extraction (NOSE) avoids extra incisions to the abdominal wall and causes less pain and fewer wound complications, together with a shorter recovery and reduced time off from work. However, the size of the specimen is a limiting factor for NOSE. We describe a novel method for natural orifice colorectal specimen extraction that reduces the diameter of the specimen and provides an easier extraction through the vagina. A totally laparoscopic right hemicolectomy for a cecal adenocarcinoma 5 cm in diameter was performed on a 62-year-old woman. Ileocolic anastomosis was done intracorporeally. Before transvaginal extraction, the largest width of the specimen was measured as 12 cm. The bulky mesentery of the cecum that limited the NOSE was divided partially along the bowel with a LigaSure™ (Covidien, Boulder, CO) device. The largest width of the specimen was reduced to 9 cm, and the specimen was extracted without difficulty through the vagina in a bag. The stage of the tumor was pT3pN1. There was no recurrence with a 7-month follow-up. Transvaginal specimen extraction may fail because of the size of the specimen. Reduction of the width of the specimen by partial division of the mesocolon provides a high success rate for NOSE. This novel technique should be in the repertoire of laparoscopic colorectal surgeons.
Introduction
L
Although NOSE benefits from the minimal invasiveness of laparoscopic colorectal surgery, all natural orifices (anus, vagina, and mouth) have anatomic limitations, and the procedure can be aborted because of specimen size. This challenge especially occurs for specimens that include larger mesenteries. We describe a novel method for natural orifice colorectal specimen extraction that reduces the diameter of the specimen and provides an easier extraction through the vagina.
Case Report
A 62-year-old woman was admitted for hypochromic microcytic anemia. Medical history was significant for cerebrovascular accident, diabetes mellitus, and hypertension that were controlled by oral antidiabetic, antiaggregant, and antihypertensive agents. Her body mass index was 31 kg/m2, and the American Society of Anesthesiologists score was III. Physical examination revealed a palpable mass in the lower right quadrant. Her biochemical parameters were in the normal range. Colonoscopy showed a 5-cm ulcerous cecal mass with a histological diagnosis of adenocarcinoma. Computed tomography of the abdomen and pelvis was negative for metastatic disease (Fig. 1). The preoperative carcinoembryonic antigen level was 2.7 ng/mL (normal, <5 ng/mL).

Cecal mass at computed tomography.
We planned a minimally invasive approach with a totally laparoscopic right hemicolectomy. The patient fully consented to the operation and also signed a detailed informed consent form. Mechanical bowel preparations were performed before hospitalization, and broad-spectrum intravenous antibiotics were administered 30 minutes before the skin incision and postoperatively for 3 days.
Surgical Technique
The patient was placed supine on the operating table, in the modified lithotomy position, with legs abducted and slightly flexed at the knees. The abdomen was insufflated to 12–15 mm Hg using a Veress technique from the umbilicus. In total, four abdominal trocars (12-mm in the umbilicus, 5-mm in the epigastrium, 12-mm in the suprapubical region, and 12-mm in the left lower quadrant [optic trocar]) were used. Total mesocolic dissection was carried out by identifying the ileocolic and right colic vessels from medial to lateral. The vessels were ligated separately with a LigaSure™ device (ForceTriad™; Covidien, Boulder, CO). Division of the transverse colon was performed with a 60-mm endoscopic stapling device (Endo GIA™; Covidien, Mansfield, MA). The colon was then separated from the lateral peritoneal attachments and from top to bottom until the cecum and terminal ileum were completely free. The terminal ileum was transected using the same endoscopic 60-mm linear stapler. The ileal limb and the transverse colon were aligned in an isoperistalsic side-to-side fashion by a 60-mm endoscopic stapler intracorporeally. The remaining enterotomy was closed in two layers with a running intracorporeal suture, and the mesenteric defect was closed.
Intracorporeal examination of the specimen revealed that the mesentery was too large for transvaginal extraction. The largest width of the specimen was 12 cm. To provide transvaginal specimen extraction, we planned to divide the bulky mesentery partially from the colon by the LigaSure (Fig. 2). Division was done along the mesentery parallel to the bowel lumen. It started from the transverse colon mesentery and was released when the terminal ileum was reached. The omentum on the colon was also divided by the LigaSure. The colonic specimen and the partially divided mesentery resembled a kite and its tail. The vagina was prepared with a povidone–iodine solution, and a speculum was used to expose the posterior vaginal wall. The patient was placed in a steep Trendelenburg position, and her uterus was grasped laparoscopically for better visualization of the pelvis. A 3-cm-long transverse transvaginal posterior colpotomy was performed under laparoscopic control, and the colpotomy incision was enlarged bluntly with fingers. A homemade sterile plastic bag was grasped with an ovary clamp through the vaginal incision, the specimen was placed longitudinally to avoid a bulky mass, and it was pulled into the vagina. The bag orifice was then opened inside the vaginal canal, using the rest of the bag as a wound protector. The specimen was delivered through the vagina without any difficulty. When the specimen was reconstructed on the back table, its largest width was 12 cm, and the length was 30 cm. After mesenteric partial division, its largest width was 9 cm (Fig. 3). The vagina was irrigated with a povidone–iodine solution. The colpotomy was closed with a running absorbable suture. A povidone–iodine-soaked vaginal pack was placed into the vagina for 12 hours. No drain was used. The nasogastric tube was removed at the end of the operation. The operating time was 120 minutes. The blood loss was 50 mL.
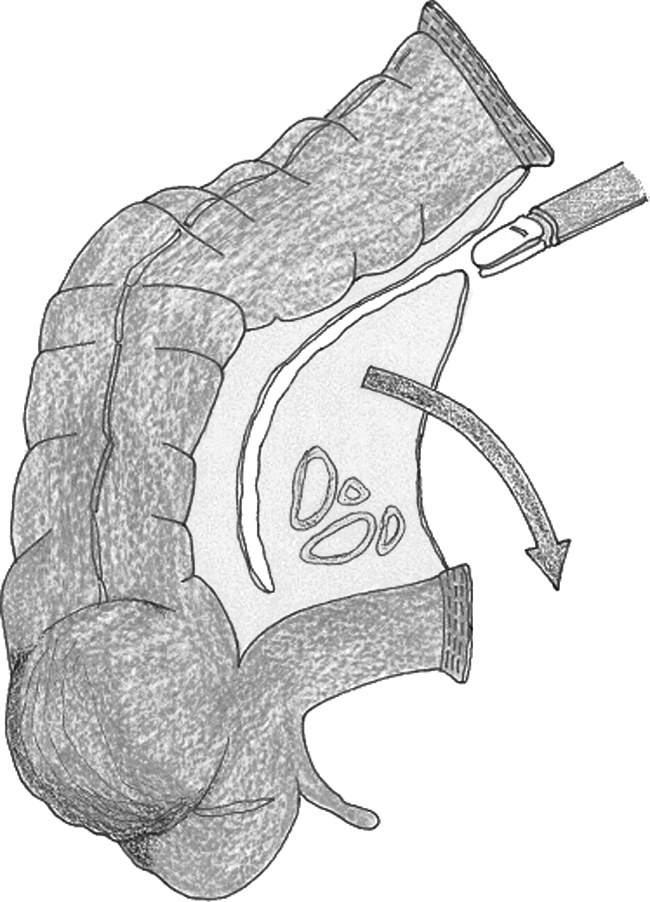
Division of the mesentery.
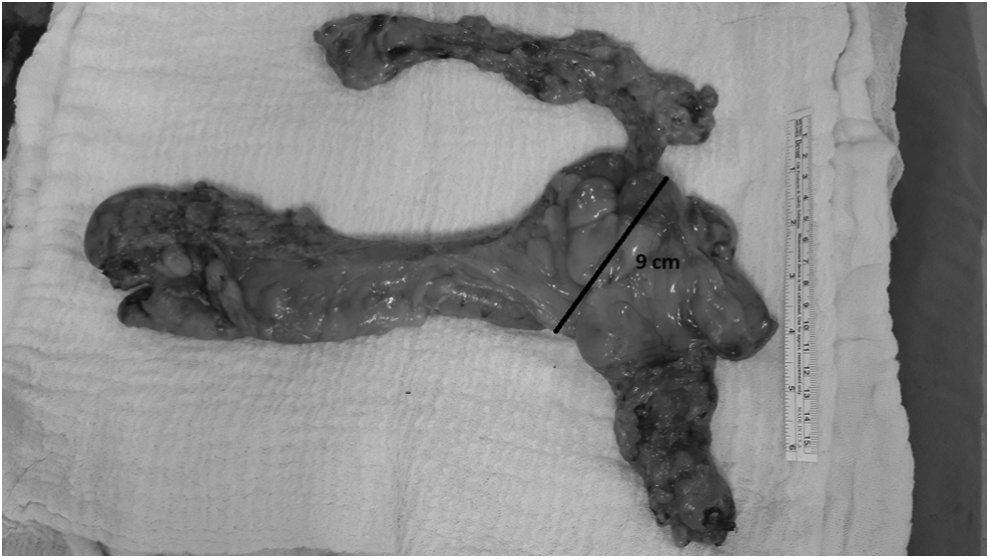
Reduced size of the specimen for natural orifice specimen extraction.
The patient was followed up in the intensive care unit on the first postoperative day. She was allowed to drink fluids and to consume a soft oral diet on the second day postoperatively. Postoperative complications were not observed, and she was discharged on postoperative Day 6. Avoidance of sexual intercourse for 1 month was advised. The histological analysis showed a pT3pN1 lesion (in total, 10 lymph nodes were retrieved), and a referral was made to a medical oncologist. There was no recurrence with a 7-month follow-up.
Discussion
Here, we described a laparoscopic right hemicolectomy, intracorporeal ileocolic anastomosis, and transvaginal extraction technique for a bulky specimen. The impact of specimen size on the success rate of transvaginal specimen extraction has not yet been determined. However, we know that the vagina has a flexible nature, and masses larger than the colpotomy incision can usually be removed transvaginally. The technique is not only for a standard right hemicolectomy; some authors have demonstrated that even extended right colectomy specimens could be removed from the vagina successfully.4,5 In 2008, Palanivelu et al. 6 described a series of 7 patients who underwent a totally laparoscopic proctocolectomy with specimen extraction through the vagina. So, the length of the specimen does not seem a challenge for transvaginal specimen extraction.
A transverse incision is made to the posterior vaginal fornix. The maximum incision size may be 3–4 cm due to anatomic limitations. Clearly, this colpotomy is not always enough for the large tumors. Large, bulky (5 cm in smaller dimension) tumors in patients were accepted as an exclusion criterion by Park et al. 4 In a similar study including 14 patients by Awad et al., 5 a tumor size below 6 cm was used as a selection criterion for transvaginal extraction. In the literature, maximum tumor size for laparoscopic right colectomy with transvaginal specimen extraction has been reported as 8 cm in diameter.7,8 However, there are no data about the largest width of the specimen. In our case, the width of the mass was 5 cm, but it had a large and fatty mesentery, and so the width of the specimen was 12 cm without mesenteric division. After downsizing by partial division of the mesocolon, its largest width was reduced to 9 cm, and it was removed through the vagina uneventfully.
Preoperative radiological evaluation for measurement of tumor size is important for patient selection. Despite the preoperative selection of the patients, radiological evaluations are not always precise, and sometimes an intraoperative decision is needed for transvaginal extraction. Park et al. 4 reported 2 patients who planned vaginal extractions after radiological examinations, but both procedures were aborted because of inconsistencies of the posterior colpotomy and specimen dimensions during surgery. Similarly, Awad et al. 5 indicated that the lesion in a patient was found to be larger during surgery than at the preoperative evaluation. We think that, especially in malignant cases, the width of the whole specimen is more important than the tumor size for transvaginal extraction. So, the presence of a large mesocolon leads to failure of transvaginal specimen extraction, and dividing the mesocolon can reduce the width of the specimen.
Division of a specimen intracorporeally can have a drawback, particularly for the oncological principles, if the intracorporeal division was not done in a bag, or the surgical area was not washed out with povidone–iodine. We partially divided the mesenteric fatty tissue by a sealing device away from the tumor and the enlarged lymph nodes. There was no deformation with the tumor and mesentery. Although it is too early to say, there was no local recurrence after 7 months, although a longer follow-up is necessary.
As a conclusion, despite the widest possible vaginal incision and dilatation, transvaginal specimen extraction may fail because of the size of the specimen. We think that reduction of the width of the specimen by partial division of the mesocolon provides a high success rate for transvaginal specimen extraction.
Footnotes
Disclosure Statement
No competing financial interests exist.