
Abstract
Abstract
Background:
The impact of preoperative chemoradiation treatment (CRT) on outcomes after esophagectomy is still debated. The choice of surgical approach can also be influenced by this treatment modality, including the performance of minimally invasive esophagectomy (MIE), a technically demanding procedure. We sought to examine the outcomes of MIE after CRT.
Materials and Methods:
We conducted a retrospective analysis of consecutive MIEs performed at two institutions from June 2004 to January 2010. We analyzed the effect of CRT on perioperative results, including pulmonary complications, oncological outcomes, length of stay, and mortality.
Results:
In total, 126 patients were eligible for the study. Six patients (4.8%) were converted from MIE to an open approach and were excluded from the analysis. Of the 120 patients, 98 were male (82%), mean age was 62±13 years (range, 22–88 years), and 58 underwent CRT (48%) (Group 1). Comparing both groups, the incidence of pneumonia (9 versus 11), recurrent laryngeal nerve injury (3 versus 5), anastomotic leaks (4 versus 9), number of harvested lymph nodes (16±9 versus 18±9), and R0 resection margins (53/58 versus 61/62) was comparable (Group 1 versus Group 2, respectively; P=not significant). There was a trend toward more pleural effusions in Group 1 (10 versus 4, P=.09). Median length of stay was comparable between both groups (10±11 versus 11±7 days). There were three operative deaths, exclusively in Group 1 (P=.11).
Conclusions:
MIE can be safely performed after CRT in the management of esophageal cancer, with a low conversion rate. Outcomes seem comparable regardless of preoperative CRT.
Introduction
T
Materials and Methods
We conducted a retrospective review of all the MIEs performed from June 2004 until January 2010 at two institutions: the Hospital of Saint Raphael (New Haven, CT) (Institution A), a 511-bed community teaching hospital (four thoracic surgeons); and Beth Israel Deaconess Medical Center (Boston, MA) (Institution B), a 621-bed university teaching hospital (four thoracic surgeons and one general surgeon). We only included esophagectomies performed for a malignant indication, whether the patient received CRT or not. The indications for CRT were tumors ≥T2 and lymph node involvement ≥N1.
The study was approved by institutional review boards in both institutions, where a minimally invasive approach was adopted in March 2005 in Institution A and June 2004 in Institution B. The conversion to the minimally invasive approach occurred in a gradual fashion in both institutions. Our surgical technique has been previously described. 8 In brief, the stomach is mobilized during the laparoscopic part of the procedure, and the conduit is fashioned while preserving the right gastroepiploic arcade. The pylorus is injected with 200 units of Botulinum toxin A as a draining procedure, and a feeding jejunostomy tube is invariably placed. Esophageal mobilization is achieved thoracoscopically with en bloc lymph node dissection. Intrathoracic anastomoses were created using a circular EEA™ stapler (Covidien, Norwalk, CT), and cervical anastomoses were hand-sewn in a single layer.
The outcome measures included demographics (age, gender), tumor characteristics (histology, location), and oncological outcomes (number of harvested lymph nodes, final margins). We also looked into the incidence of pulmonary complications such as pneumonia (clinical and radiographic data) 9 and pleural effusion/chylothorax requiring intervention (thoracentesis, placement of pigtail catheter, thoracostomy tube, or return to the operating room), as well as other surgical complications (recurrent laryngeal nerve injury, anastomotic leak). We also included the length of hospital stay and perioperative mortality. The data were collected from electronic medical records and hospital and outpatient clinic charts.
Fisher's test and Student's t tests were used for statistical analysis; significance was reached with P<.05. Numerical data are presented as mean±standard deviation values unless otherwise specified.
Results
In total, 126 patients were eligible for the study. Six patients (4.8%) were converted from MIE to an open approach and were excluded from the analysis. The causes for conversions were: bleeding (n=3), significant adhesions (n=2), and inadequate conduit length (n=1) (Fig. 1). Receipt of CRT did not seem to predict the need for conversion (P=1.0). Of the 120 patients who completed the resection, 98 were male (82%); the overall mean age was 62±13 years (range, 22–88 years), and 58 underwent CRT (48%) (Group 1). The stomach was used as the esophageal replacement in all patients, with the anastomoses preferentially performed in the neck (n=90, 75%). The location of the anastomosis mainly depended on the tumor location from the incisors and the surgeon's preference.
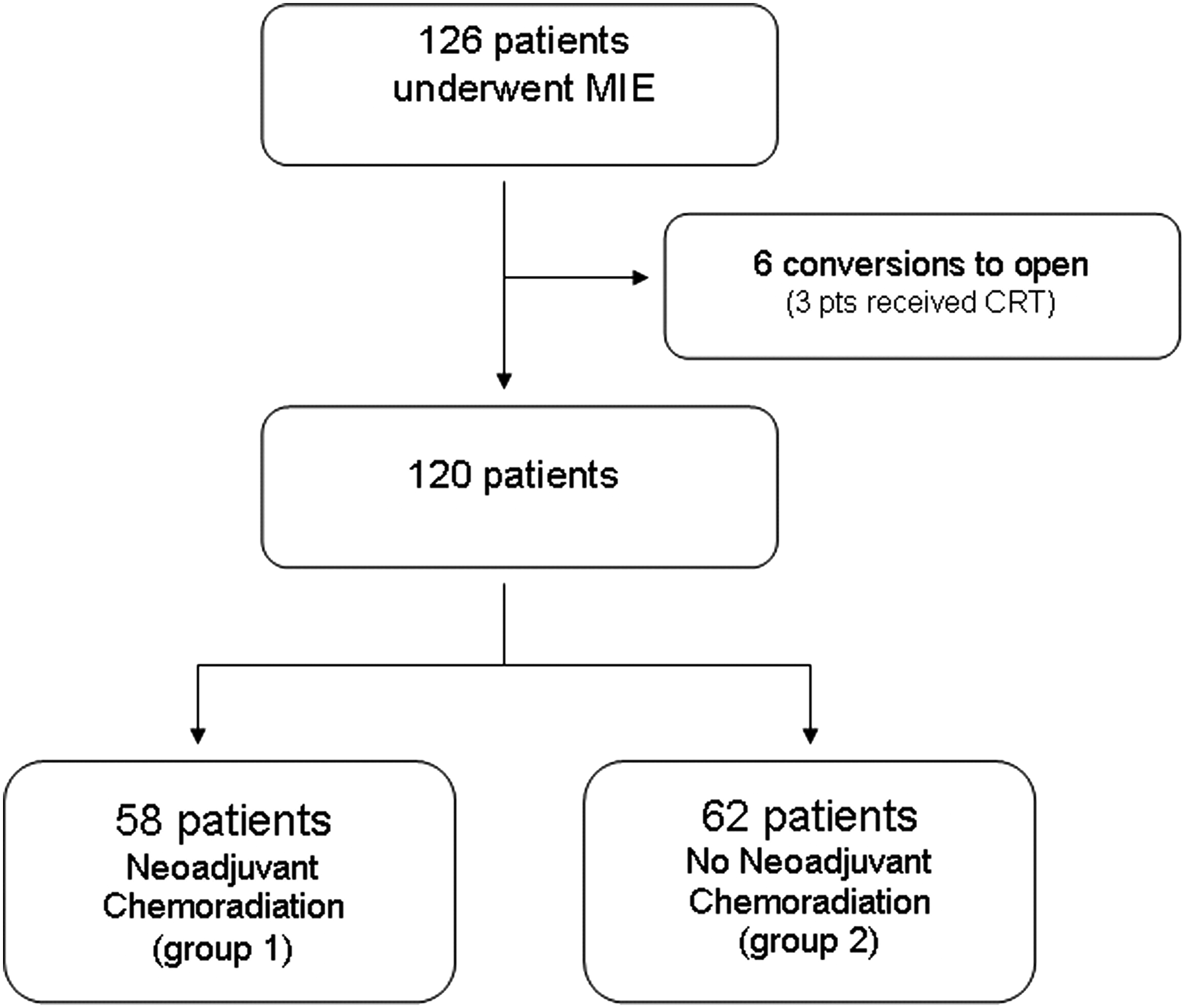
Diagram depicting the study population. CRT, neoadjuvant chemoradiation treatment; MIE, minimally invasive esophagectomy.
The distribution of MIEs between the two institutions is presented in Table 1; demographic and histopathologic features of both groups are presented in Table 2. Patients who received CRT were statistically significantly younger (P=.006). Gender and performance of a cervical anastomosis were not statistically different (P=.82 and P=.67, respectively), nor was the tumor location or preoperative albumin levels (P=not significant). Preoperative jejunostomy feeding tubes were placed in 74% of the patients who underwent CRT. None of the patients in Group 2 underwent preoperative esophageal stenting of jejunostomy tube placement.
Institution A was the Hospital of Saint Raphael (New Haven, CT), and Institution B was Beth Israel Deaconess Medical Center (Boston, MA).
CRT, neoadjuvant chemoradiation treatment.
One patient had synchronous proximal and distal tumors.
CIS, carcinoma in situ; CRT, neoadjuvant chemoradiation treatment; HGD, high-grade dysplasia.
Chemotherapy consisted of a platinum-based chemotherapy regimen, except in 2 patients (3%) who received 5-fluorouracil chemotherapy alone due to underlying chronic renal failure. The radiation dose was 5040 cGy, and the average length of neoadjuvant treatment was 46±11 days. CRT could not be fully administered in 9 patients (14%) because of intolerance or other complications. These included the following: renal failure/acute kidney injury in 3 patients (5%), febrile neutropenia in 2 (3%), failure to thrive in 7 (12%), esophagitis in 4 (7%), enteritis in 1 (2%), dehydration from nausea and vomiting requiring recurrent visits to the emergency room in 5 (9%), pulmonary embolism in 1 (2%), and re-admission to the hospital in 3 (5%). Receipt of CRT was fluctuant throughout the study period, and its distribution per year is presented in Figure 2. Restaging data were available for 72% of the patients who underwent CRT and consisted of repeat positron emission tomography and/or computed tomography scans. Among these patients, the rate of downstaging was 61%, as defined by a decrease in fluorodeoxyglucose activity and/or decrease in tumor or lymph node(s) size(s).

Distribution of neoadjuvant chemoradiation treatment throughout the study period. pts, patients.
Comparison of the other outcomes parameters are presented in Table 3. There was no difference in lymph node harvest between Groups 1 (median, 15; range, 4–40) and 2 (median, 17; range, 2–51). R0 resection was achieved in most patients (95%), regardless of CRT. There was a trend toward more pleural effusions in the group of patients who received CRT (P=.09). More patients in Group 1 required a re-interventional surgical procedure over the short and intermediate term, but the difference did not reach statistical significance. The reasons for re-operations were variable and included small bowel obstruction, repair of hiatal or incisional hernia, drainage of hemothorax, and ligation of thoracic duct for chylous leak, as well as drainage of empyema and repair of anastomotic leak.
Data are number of patients (%) or mean±standard deviation values (except length of stay [LOS], which is median±standard deviation values).
LN, lymph node; RLN, recurrent laryngeal nerve.
The overall mortality rate was low (2.5%) and was not different between both groups. The causes of deaths were as follows: 1 patient died on postoperative Day 21 at home, 2 weeks after his discharge, and an autopsy was not performed; 1 patient died from pneumonia and subsequent respiratory failure; and the third patient died from sepsis and multiorgan failure due to a tracheo-neoesophageal fistula. The three deaths occurred in patients who underwent a neck anastomosis. Two of the patients had an adenocarcinoma (final pathological stage T3N0 for both) and died in the first half of the study period, and the third patient who died had a squamous cell carcinoma (final pathological stage T4N0) during in the second half of the study period.
Discussion
Esophagectomy remains a complex and challenging procedure, even more so after the introduction of minimally invasive techniques, which aim at reducing the morbidity of surgical resection. MIE is currently being adopted with increased frequency in the United States and around the world and is known for its steep learning curve. Before these surgical advancements were introduced, induction treatment was advocated a few decades ago with the hopes of improving survival of patients with resectable esophageal cancer. However, the benefit of multimodality treatment was somehow controversial over many years, partially because of the concern about increased perioperative morbidity from the effects of chemotherapy and/or radiation. In fact, radiation is known to impair wound healing in general and has been shown to adversely affect the healing of gastrointestinal anastomoses in some laboratory models. 10 In a retrospective series by Avendano et al., 5 preoperative chemoradiotherapy was also found to be a significant risk factor for pulmonary complications after esophagectomy. Furthermore, a prospective ECOG Phase II trial showed high-dose chemoradiotherapy to cause severe toxicity, resulting in eight treatment-related deaths, out of the 46 patients who were enrolled in the study (two preoperative and six postoperative deaths). 11
However, significant improvements in chemotherapy regimens and radiation modalities have occurred in the last two decades, and more recent data did not show any significant deleterious effect due to CRT. For instance, Berger et al. 6 did not find any significantly increased morbidity or mortality in patients who underwent induction treatment, except for the incidence of recurrent laryngeal nerve injury and deep vein thrombosis. Another retrospective analysis of 138 esophagectomies by Merritt et al. 7 found similar intensive care unit stay, ventilator time, and overall complication and mortality rates between patients who underwent induction treatment (n=54) and those who did not (n=84).
In addition to these retrospective reviews, recent clinical prospective data clearly demonstrated the overall survival benefit of preoperative chemoradiation in the management of locally advanced or node positive esophageal cancer.12,13 For instance, the recent randomized (CROSS) trial from Europe included 368 patients with resectable esophageal cancer and showed better overall survival in those who received CRT (hazard ratio, 0.657; 95% confidence interval, 0.495, 0.871; P=.003); the survival benefit was not limited to patients with adenocarcinomas (P=.049), but also included patients with squamous cell cancer (P=.011). 13 The authors also found no difference in the mortality rate, anastomotic leak rates, the incidence of chylothorax, or pulmonary or cardiac complications between those who received CRT and those who did not. These results were confirmed in two recent meta-analyses that supported the use of preoperative induction therapy (chemotherapy or chemoradiation) in patients with resectable esophageal cancer.14,15
However, it is noteworthy to mention that most of these studies almost exclusively included patients who underwent open esophagectomies. In fact, there is a paucity of data specifically examining the outcomes of MIE following CRT. We sought in our study to demonstrate the safety and feasibility of MIE after induction treatment and to investigate whether or not this treatment modality can affect the outcomes. Similar to two other retrospective series,16,17 we found no significant deleterious effect of induction chemoradiation on performance of a MIE. There were only six conversions from a minimally invasive to an open approach in our series, and that did not seem to be directly related to CRT, as half of the converted patients received trimodality therapy and the other half did not. Either way, these conversions were excluded from the analysis in view of the retrospective nature of our study. We found no statistical difference in the incidence of anastomotic leak, pneumonia, or recurrent nerve injury, the incidence of which seemed to be dispersed over the study period.
The oncological outcomes, length of hospital stay, and the mortality rate (2.5% overall) were not different either.
Our outcomes also mirror those of open esophagectomies after CRT series that we discussed earlier2,6,7 and are not surprising. In fact, the updated MIE series from the University of Pittsburgh also demonstrates superior results with low mortality (1.68%) and overall complication rates. 4 One has to acknowledge that these outcomes are the result of not just a refined technique, but also of high-volume centers.
Patients in both groups in our series had similar baseline characteristics except for age, where those who underwent CRT were significantly younger. This may have influenced the results as the effects of chemoradiation may be more pronounced in older patients. In fact, Mak et al. 18 reported substantial morbidity in their series of 36 patients older than 75 years of age who underwent definitive or neoadjuvant chemoradiation. However, other authors showed that age >70 years was not a risk factor for morbidity or mortality after trimodality therapy for esophageal cancer. 19
A positive relationship between esophagectomy outcomes and smoking or American Society of Anesthesiologists class has been demonstrated mainly in large retrospective reviews or database analyses.20,21 We did not feel we could investigate the association between them and be able to draw firm conclusions, in view of the relatively low incidence of overall complications, relatively small sample size of our series, and the wide variability of smoking history that we found in the patient population.
The other limitations of our series are its bi-institutional and retrospective nature, with a potential for selection bias. Although more than 90% of the data were gathered by two authors only, we have to acknowledge some interinstitutional variability in the operative and postoperative care that may have led to differences in the outcomes. We did not include the operative time or blood loss in the comparative analysis either.
Acknowledging these limitations, we found that MIE can be safely performed after CRT in the management of esophageal cancer, with a low conversion rate. Surgical and oncological outcomes of esophageal resection seem comparable regardless of preoperative CRT, which should not be an obstacle for the adoption of a minimally invasive approach.
Footnotes
Acknowledgments
We thank Jean M. Cornwell for design of the poster presented at the SAGES meeting, March 2012.
Disclosure Statement
No competing financial interests exist.