
Abstract
Abstract
Background:
The aim of this study is to compare the number of retrieved lymph nodes according to lymph node stations in laparoscopy-assisted distal gastrectomy (LADG) of the early experience of a new surgeon with that in open distal gastrectomy (ODG).
Materials and Methods:
From May 2008 to August 2012, clinicopathologic data of gastric cancer patients subjected to LADG or ODG at a single institution by one surgeon were retrospectively reviewed. The surgeries were stratified as follows: early LADG (initial 30 LADGs), late LADG, and ODG. Station-specific counts of lymph nodes retrieved served for group comparisons.
Results:
Gender distribution (male:female ratio) was not different among the three groups (early LADG, 16:14; late LADG, 19:4; and ODG, 38:30). Mean lymph node retrieval in the early and late LADG groups (39.1 and 45.6, respectively) fell significantly below that of the ODG group (53.0) (P<.001). Compared with the ODG group, fewer station-specific lymph nodes were retrieved via LADG, both early (stations 3, 8a, and 11p) and late (station 11p).
Conclusions:
Surgeons inexperienced in LADG for gastric cancer should be particularly diligent in lymph node dissection at stations 3, 8a, and 11p. Even with more experience (>30 LADGs), lymph node dissection at station 11p merits special attention.
Introduction
O
Although LADG with regional lymph node (LN) dissection is now a well-established practice for early, distal gastric cancers in East Asia, this is a delicate and complex procedure for an inexperienced surgeon. Learning-curve studies have thus been conducted at some facilities, focusing on duration of surgery, intraoperative blood loss, LN counts, and morbidity rates.7–9 These studies indicate that 30–60 LADG procedures are required to master LN dissection within a reasonable operative time frame.
Regional LN dissection, performed by station, is a valuable means of gauging the extent of anatomic dissection. Two recent studies have actually addressed this, comparing LN counts in LADG and ODG by station. One report by Han et al. 10 cited significantly lower counts for group 1 and group 2 LNs in LADG. On the other hand, Bouras et al. 11 found station-specific LN counts in LADG and ODG to be similar, with the exception of common hepatic artery nodes. Nevertheless, studies directed at the learning curve for proper execution of LN dissection in LADG are limited.
Our intent was to assess the counts of LNs retrieved during station-specific dissection in both LADG and ODG, as performed by a new surgeon fresh from fellowship training. In addition, perioperative states were evaluated, and therapeutic outcomes were monitored in follow-up.
Materials and Methods
Patients
The patient population was confined to a consecutive cohort of one surgeon who had completed a 2-year fellowship in gastrointestinal division. During the training, the surgeon jointly experienced roughly 200 laparoscopic gastrectomies, serving therein as the first assistant or the laparoscopist. After that, the surgeon performed about 5 cases of laparoscopic gastrectomies as the operator. Regarding open gastrectomies, the surgeon experienced roughly 300 cases as the first assistant and 10 cases as the operator. Between May 1, 2008 and August 31, 2012, the patients surgically treated for gastric cancer (LADG or ODG) at Konkuk University Medical Center (Seoul, Korea) were eligible for this study. The breakpoint for early and late LADG groups was defined at 30 procedures.
Gastric cancer patients with following conditions were excluded from this study: (1) combined malignancies; (2) preoperative chemotherapy; (3) distant metastasis; (4) residual tumor (macroscopic or microscopic); or (5) indications for endoscopic submucosal dissection.
Study parameters included patient demographics (age, sex, and body mass index), operative data (surgical approach, extent of nodal dissection, type of anastomosis, and operative time), perioperative course (postoperative hospital stay, morbidity, and mortality), tumor staging by TNM classification, 12 and follow-up status.
LNs were separated from the specimen according to station. Each LN station was clearly labeled and classified, as stipulated by the Japanese Gastric Cancer Association. 13 Accordingly, the number of nodes retrieved and nodes with metastases were collected at each station.
Surgical procedure
The indication for LADG was clinical T1N0M0 gastric cancer located at the lower to middle third of the stomach, with ODG reserved for T2 or higher disease stage. Depth of invasion and distant metastasis were evaluated by preoperative endoscopic ultrasonography and computed tomography. A distal gastrectomy with more than D1+ LN dissection was performed in both the LADG and ODG groups. In accordance with Japanese Gastric Cancer Association guidelines, more than D1+ or D1+ regional LN dissection was performed during LADG, and D2 regional LN dissection was usually performed during ODG. With stations 1, 3, 4sb, 4d, 5, 6, 7, 8a, and 9 as D1+, stations 11p and 12a were added for D2 (Fig. 1). LN dissection was completed en bloc, simultaneously with gastric mobilization and resection.
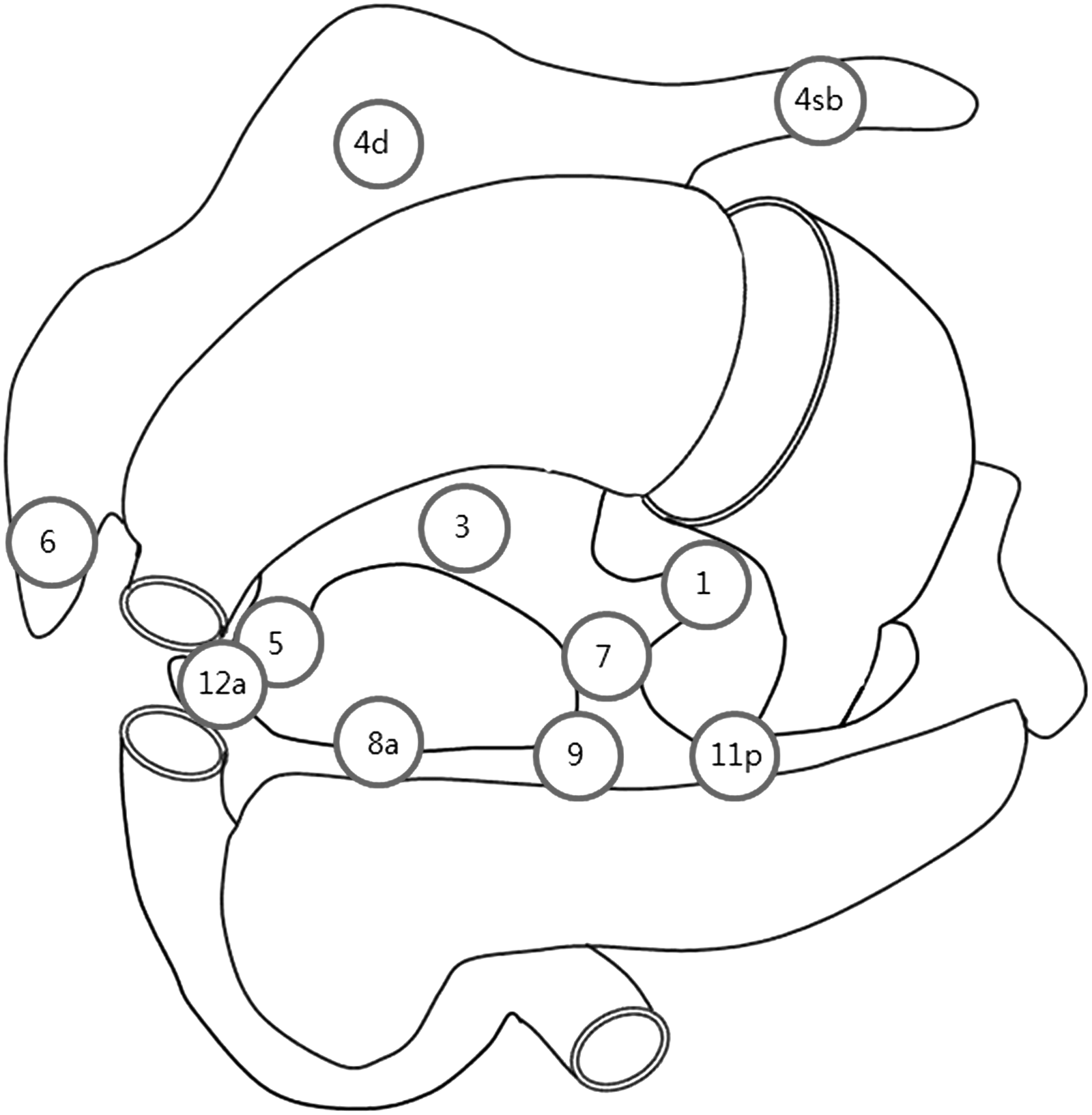
Regional lymph nodes in distal gastrectomy.
In LADG, patients were placed under general anesthesia in the supine, reverse Trendelenburg position, with leg elevation. A 12-mm trocar for the camera port was inserted through the infraumbilical side using the open technique, and a pneumoperitoneum was established by CO2 inflation at a pressure of 12 mm Hg. Under visualization by fiberscope introduced through the infraumbilical port, one 5-mm trocar and one 11-mm trocar were placed on the right upper side of the camera port, and two 5-mm trocars were inserted at the left upper side of the camera port. The procedure for partial omentectomy commenced from the division of the omentum approximately 3–4 cm inferior to the gastroepiploic arcade using an ultrasonic device. This procedure included dissection of the No. 4d (right gastroepiploic artery) and No. 4sb (left gastroepiploic artery) LNs. The No. 6 (infrapyloric) LNs were meticulously dissected, followed by ligation of the right gastroepiploic vessels. The No. 12 (proper hepatic artery) and No. 5 (suprapyloric) LNs were dissected followed by ligation of the right gastric vessels. Suprapancreatic LNs were dissected, and the left gastric artery was ligated. During this procedure, dissections of the No. 7 (left gastric artery), 8a (common hepatic artery), 9 (celiac artery), 11p (proximal splenic artery) LNs were completed, and the celiac branch of the posterior vagus nerve was sacrificed. The lesser omentum along the hepatoduodenal ligament was divided. Then dissection of the No. 1 (right cardia) LNs was performed followed by clearing the lesser curvature's side of the stomach for resection.
After LN dissection and mobilization of the stomach, the stomach was extracted through the 5-cm transverse minilaparotomy at the epigastric area. Depending on the location and size of the tumor, the stomach was resected, and gastroduodenal or gastrojejunal anastomosis was performed.
Statistical analysis
Descriptive statistics were expressed as mean±standard deviation or percentage. Student's t test, chi-squared test, and one-way analysis of variance with multiple comparison of least significant difference were used for comparative statistical analysis. Data were analyzed using SPSS version 17.0 software (SPSS, Chicago, IL). In two-tailed testing, statistical significance was set at P<.05.
Results
Clinical characteristics of the 121 patients investigated are presented in Table 1. No LADG procedures were converted to ODG during the course of surgery. Mean follow-up periods for the early and late LADG groups were 39.2 and 15.3 months, respectively. The complications of the early LADG group were as follows: surgical wound infection in 2 cases and postoperative intraperitoneal fluid accumulation in 1 case. In the late LADG group, the sole incident was urethral injury due to abrupt withdrawal of a urinary catheter (the patient self-extracted with the balloon inflated). No cancer recurrences were recorded in the early or late LADG group.
F, female; LADG, laparoscopy-assisted distal gastrectomy; M, male; ODG, open distal gastrectomy.
Mean LN retrieval (procedural total) was significantly lower in the early and late LADG groups, compared with the ODG group (P<.001) (Table 2). In multiple comparison testing (least significant difference), mean LN retrieval at each of three stations (3, 8a, and 11p) was significantly lower in the early LADG group (versus the ODG group), whereas the late LADG group differed only at station 11p when similarly compared (Table 3).
LADG, laparoscopy-assisted distal gastrectomy; ODG, open distal gastrectomy.
There is a significant difference between the ODG and early LADG group.
There is a significant difference between the ODG and late LADG group.
LADG, laparoscopy-assisted distal gastrectomy; LN, lymph node; ODG, open distal gastrectomy.
Discussion
Oncologic feasibility is assessed by comparing respective LN counts achieved with the two procedures (LADG and ODG), as well as disease recurrence and survival rates. Because the number of dissected LNs can be evaluated earlier than the other two factors, it is given considerable weight by surgical oncologists who are overcoming learning curve. Although LN harvesting in LADG and ODG have proved similar in some randomized controlled studies,14–16 at least one such effort and a recent meta-analysis, consolidating 6 randomized controlled trials and 19 high-quality, nonrandomized comparative studies, have shown that LN harvesting in ODG is significantly higher.17,18 Unfortunately, few investigations have examined LN counts by station, and none has addressed the learning curve for LN dissection in a station-specific manner. Our intent was to overcome these former limitations.
Prior efforts have suggested that 30–90 procedures are needed for proficiency in LADG.7,19–21 More recently, however, the roles of the laparoscopist and the assistant have been credited with impacting the learning curves of trainees,22,23 resulting in a reset of this prerequisite to about 30 cumulative procedures. We therefore stratified LADGs at this breakpoint, assigning the initial 30 procedures to the early group and the remainder to the late group. At the same time, we acknowledged exposure to far more than 30 LADG procedures as part of our own fellowship training, whether as scopist or assistant.
In this study, the extent of nodal dissection varied by group. LADG was indicated for cT1N0 disease, generally corresponding with D1+ dissection (D1 plus stations 8a and 9), but D2 dissection was done increasingly as experience rose. Similar to previous studies, D2 dissections were performed more in the ODG group. Although mean LN retrieval (procedural total) of our early and late LADG groups exceeded 26 nodes, which was defined as radical lymphadenectomy, 24 it was statistically inferior to that of the ODG group. Compared with ODG, mean LN retrieval at each of three stations (3, 8a, and 11p) was significantly lower in the early LADG group. This outcome is aligned with findings of Han et al., 10 in terms of perigastric/extragastric LNs retrieved in the first 100 LADGs logged. Likewise, 259 LADGs performed by Bouras et al. 11 resulted in fewer nodes at station 8a (versus ODG), similar to station 8a counts in our early LADG group, but again our late LADG group did not follow suit. Insufficient sampling size, low frequency (36%) of 11p station dissection in the study of Bouras et al., 11 or technical differences may account for the observed disparity.
The differences we encountered in station 11p LN counts of late LADG and ODG groups may reflect either technical or psychological divergence. If technical inexperience has an impact on this result, more cases of LADG will be necessary to elucidate the learning curve of 11p dissection. In another viewpoint, because D1+ nodal dissection can be enough for cT1N0M0 gastric cancer, it is conceivable that station 11p dissection is subliminally viewed as overtreatment, dampening the vigor with which nodes are obtained even though D2 lymphadenectomy was planned preoperatively.
The distinct improvement seen in late versus early LADG node retrieval (perigastric and station 8a) once more may corroborate our learning curve breakpoint (30 cases for D1+). Overall, our results confirm the surgical feasibility of LADG with D1+ LN dissection for early gastric cancer, given a foundation of at least 30 procedures to hone surgical skills. If D2 LN dissection is performed for advanced gastric cancer, station 11p dissection could be tenuous even after the initial experience of 30 LADG cases. The early and late LADG groups showed briefer postoperative hospitalization than the ODG group, ostensibly because of earlier recovery and fewer related complications.
In conclusion, surgeons inexperienced in LADG for gastric cancer must appreciate the need for meticulous nodal dissection at stations 3, 8a, and 11p. Even in surgeons more skilled (>30 LADGs), dissection at station 11p merits special attention.
Footnotes
Disclosure Statement
No competing financial interests exist.