
Abstract
Abstract
Background:
Pylorus-preserving gastrectomy (PPG) has been performed to reduce postprandial symptoms for some early gastric cancer (EGC) cases. The aim of this study was to evaluate the possible advantages after PPG for middle-third EGC in comparison with distal gastrectomy.
Materials and Methods:
We searched Medline, Embase, and Science Citation Index Expanded for relevant studies. Statistical analyses were conducted to calculate the summary weighted mean differences (WMDs) and odds ratios (ORs) with corresponding 95% confidence intervals (95% CIs) using random-effects models.
Results:
We identified 15 nonrandomized controlled trials (16 studies) with 1774 patients, which consisted of 11 studies for conventional PPG (CPPG) versus conventional distal gastrectomy (CDG) and 5 studies for laparoscopy-assisted PPG (LAPPG) versus laparoscopy-assisted distal gastrectomy (LADG). Meta-analysis of CPPG versus CDG revealed that CPPG had the advantage of prevention of early dumping syndrome (OR=0.18; 95% CI 0.12, 0.27), gastritis (OR=0.19; 95% CI 0.07, 0.53), duodenal juice reflux (OR=0.20; 95% CI 0.06, 0.66), and regaining of weight (WMD=3.53; 95% CI 2.34, 4.72). However, the incidence of gastric stasis was higher in the CPPG group than in the CDG group (OR=1.70; 95% CI 1.13, 2.57). Meta-analysis of LAPPG versus LADG revealed that LAPPG shortened the operation time (WMD=−21.12; 95% CI −31.33, −10.90) and did not increase the occurrence of postoperative complication (OR=0.72; 95% CI 0.41, 1.27).
Conclusions:
With the benefits of prevention of early dumping syndrome, duodenal juice reflux, gastritis, and regaining of weight, PPG can be an excellent option for middle-third EGC.
Introduction
G
Pylorus-preserving gastrectomy (PPG) was first developed by Maki et al. 5 in 1967 to treat gastric ulcers. In 1991, Kodama and Koyama 6 first reported the indications of PPG for middle-third EGC by analysis of the relationship between lymph node metastasis and the clinicopathologic findings. Attributing to the preservation of pyloric function, PPG was reported to be beneficial in terms of postoperative quality of life. However, in order to maintain good pyloric function, this gastrectomy required preservation of the root of the right gastric artery, the infrapyloric vessels, and the hepatic, pyloric branch of the vagus nerve.7–9 Such a delicate technique may be difficult to perform laparoscopically because of limited maneuverability of the instruments. In particular, the suprapyloric lymph node (station No. 5 node) was not dissected during the procedure. 10 It was unclear whether PPG was beneficial to patients preoperatively diagnosed with EGC located in the middle third of the stomach. Therefore, we performed a meta-analysis to assess systematically the value of PPG for treatment of middle-third EGC.
Materials and Methods
Literature search
A comprehensive search of Medline, Embase, and Science Citation Index Expanded was carried out for all related literature published in English, including references from relevant articles. The medical subject headings and key words searched for individually and in combination were as follows: “pylorus-preserving gastrectomy,” “conventional pylorus-preserving gastrectomy,” “conventional distal gastrectomy,” “laparoscopy-assisted pylorus-preserving gastrectomy,” and “laparoscopy-assisted distal gastrectomy.” The last search was conducted on January 1, 2014.
Inclusion criteria and exclusion criteria
We identified and screened the search findings for potentially eligible studies. The inclusion criteria were as follows: (1) human trials of patients with histologically confirmed gastric cancer; (2) the tumor was located in the middle or lower third of the stomach; (3) EGC (invasion depth confined to the mucosal or submucosal layer); and (4) studies with at least one of the outcomes mentioned. The exclusion criteria were as follows: (1) abstract, letters, editorials, expert opinions, reviews, and case reports; (2) tumor invades deeper than the submucosal layer; (3) studies without a control group; and (4) studies without available data.
Data extraction and quality assessment
Two authors (P.S. and M.L.) independently reviewed and extracted the data needed using standard forms. Disagreements were resolved through discussion among the authors to achieve a consensus. For the purpose of assessing quality, we use the Newcastle–Ottawa scoring system 11 : having 5–9 stars was defined as high quality, and having <5 stars was defined as low quality.
Statistical analysis
Weighted mean differences (WMDs) and odds ratios (ORs) with corresponding 95% confidence intervals (95% CIs) were used for the analysis of continuous variables and dichotomous variables, respectively. Considering there is potentially clinical heterogeneity among the studies due to differences with respect to eligibility of population, kind of surgical procedures, different definitions of outcome parameters, and differences in the perioperative or postoperative management, random-effect models were applied in this meta-analysis. 12 This model might provide an appropriate estimate of the average treatment effect even if trials are statistically heterogeneous and result in a more conservative statistical claim. Statistical heterogeneity among studies was evaluated by the chi-squared-based Q test and I2 statistics, with Pheterogeneity<.1 regarded as statistical heterogeneity among the studies. 13 An I2 of 0%–25% indicated no heterogeneity, 25%–50% may represent low heterogeneity, 50%–75% may represent moderate heterogeneity, and 75%–100% was considered to represent high heterogeneity. Sensitivity analysis was conducted by sequential omission of individual studies. Egger's test and Begg's funnel plots were used to evaluate publication bias. 14 If publication bias existed, the Duval and Tweedie nonparametric “trim and fill” method was used to adjust for the bias. 15 All statistical analyses were carried out with Stata software (version 12; StataCorp LP, College Station, TX).
Results
Search results, study characteristics, and quality assessment
Overall, in total, 402 records were identified by the search strategy, of which 82 were considered with potential value and full text was retrieved for detailed assessment. Among these 82 articles, 62 were further excluded for the following reasons: review or editorial (n=20), without comparison (n=32), and without available data (n=10). Four articles that investigated the outcome of laparoscopy-assisted PPG (LAPPG) in comparison with open PPG were excluded. Because only one randomized controlled trial (RCT) has been published, no meta-analysis of RCTs can be performed, so we excluded the RCT. Finally, 15 non-RCTs (16 studies)10,16–29 were considered suitable for meta-analysis, consisting of 11 studies for conventional PPG (CPPG) versus conventional distal gastrectomy (CDG) and 5 for LAPPG versus laparoscopy-assisted distal gastrectomy (LADG) (Fig. 1).
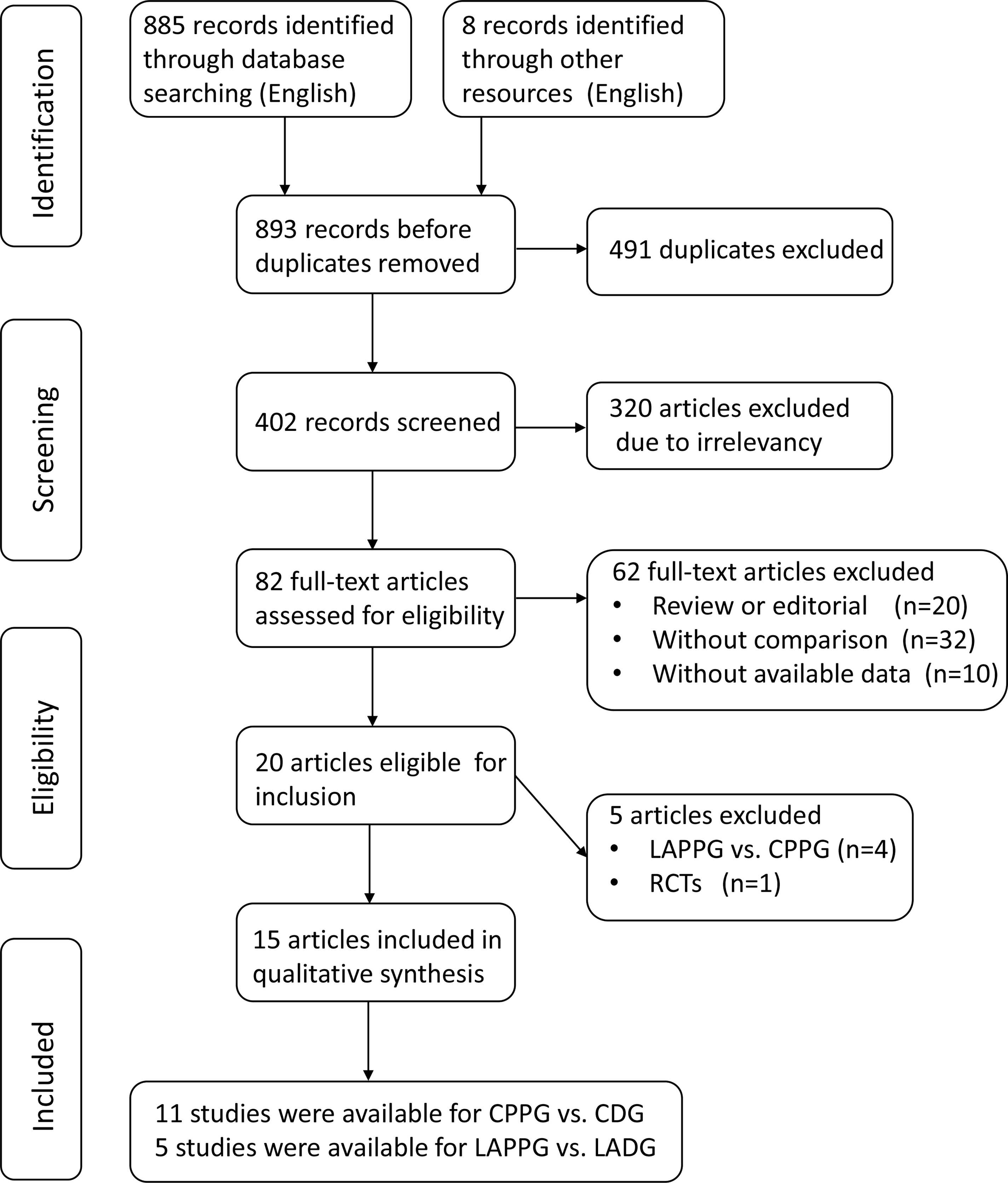
Flowchart of articles identified with criteria for inclusion and exclusion. CDG, conventional distal gastrectomy; CPPG, conventional pylorus-preserving gastrectomy; LADG, laparoscopy-assisted distal gastrectomy; LAPPG, laparoscopy-assisted pylorus-preserving gastrectomy; RCT, randomized controlled trial.
The characteristics of these 16 studies are summarized in Table 1. There were, in total, 1774 subjects involved in the meta-analysis. All studies were carried out in Asia. The sample size of the included studies ranged from 21 to 453. The number of patients who underwent PPG or LAPPG was 715. The mean age of the patients in these studies varied from 54 to 69.2 years. A nine-star Newcastle–Ottawa Scale was used to assess the quality of studies (see Supplementary Table S1 [Supplementary Data are available online at www.liebertpub.com/lap]). 11 Each study had a score of ≥5 stars (see Supplementary Table S2).
The method of reconstruction in conventional distal gastrectomy (CDG) or laparoscopy-assisted distal gastrectomy (LADG).
Operations in conventional pylorus-preserving gastrectomy (CPPG) or laparoscopy-assisted pylorus-preserving gastrectomy (LAPPG).
BI, Billroth I; NA, not applicable.
CPPG versus CDG
Dumping syndrome
Five studies reported data on the early dumping syndrome.17,18,20,21,28 The combined results showed an obvious favorable tendency for CPPG compared with CDG (OR=0.18; 95% CI 0.12, 0.27) (Table 2), and no heterogeneity was observed (I2=0.0%). Only two studies provided data on late dumping syndrome.17,21 The summary results indicated that there was no statistical difference (OR=0.66; 95% CI 0.28, 1.55) (Table 2) with no heterogeneity (I2=26.3%).
Number of comparisons.
P value of Q-test for heterogeneity test.
P value of Egger's test for publication bias.
P value of Begg's test for publication bias.
CDG, conventional distal gastrectomy; CPPG, conventional pylorus-preserving gastrectomy; LADG, laparoscopy-assisted distal gastrectomy; LAPPG, laparoscopy-assisted pylorus-preserving gastrectomy.
Gastritis, bile regurgitation, and esophagitis
Nine studies provided data on the gastritis.16–18,20–24,28 The rate of gastritis was lower for CPPG (OR=0.19; 95% CI 0.07, 0.53) (Table 2) with significant heterogeneity (I2=75.4%). Six studies provided data on bile regurgitation.16,17,20–22,24 The results showed that CPPG had a lower incidence of bile regurgitation (OR=0.20; 95% CI 0.06, 0.66) (Table 2), and a marked heterogeneity was observed (I2=67.9%). Five studies reported data on esophagitis.17,18,20,21,28 The rate of esophagitis was also lower for CCPG (OR=0.36; 95% CI 0.06, 2.21) (Table 2) with significant heterogeneity (I2=67.2%).
Gastric stasis
Five studies10,17,18,24,28 compared the gastric stasis between CPPG and CDG groups, and the incidence of gastric stasis was higher in CPPG (OR=1.70; 95% CI 1.13, 2.57) (Table 2) with no heterogeneity (I2=0.0%).
Gallbladder stones
Five studies16,17,23,24,28 compared the occurrence of gallbladder stones between the two groups, and there was no significant difference among them (OR=0.65; 95% CI 0.37, 1.14) (Table 2) with no heterogeneity (I2=0.0%).
Serum albumin level and recovery body weight ratio
Data on serum albumin level was available in four studies,16,19–21 and no significant difference was found (WMD=0.03; 95% CI 0.04, 0.11) (Table 2). Recovery body weight ratio (present body weight/preoperative weight) was reported in four studies.17,20,23,28 The results were in favor of the PPG group (WMD=3.53; 95% CI 2.34, 4.72) (Table 2), and heterogeneity was not observed (I2=0.0%).
LAPPG versus LADG
Operative time
The duration of operative time (three studies)25,27,29 in the LAPPG group was shorter than in the LADG group (WMD=−21.12; 95% CI −31.33, −10.90) (Table 2) with no heterogeneity (I2=0.0%).
Postoperative complications
Postoperative complications were specified in three studies.10,26,29 The rate of overall postoperative complications was lower for LAPPG versus LADG (15.1 versus 19.7%; OR=0.72; 95% CI 0.41, 1.27) (Table 2). The level of heterogeneity was low (I2=34.3%). Gastric stasis was found in 6.8% of the LAPPG group and in 5.4% of the LADG group. Anastomotic leak occurred in 0.7% of LAPPG group compared with 4.9% of the LADG group.
Test of heterogeneity
When comparing CPPG with CDG, we observed significant heterogeneity in the gastritis, esophagitis, and bile regurgitation complications. To explore the sources of heterogeneity, we performed subgroup analysis stratified by the length of the antral cuff preserved. Among the subgroup in which a 1.5-cm length of the antral segment was preserved, no heterogeneity was found, and the pooled ORs were 0.16 (95% CI 0.08, 0.29) (Fig. 2A) for gastritis, 0.12 (95% CI 0.05, 0.29) (Fig. 2B) for bile regurgitation, and 0.18 (95% CI 0.05, 0.72) (Fig. 2C) for esophagitis. The level of heterogeneity in the subgroup in which a >2.5-cm length of the antral cuff was preserved was low.

Conventional pylorus-preserving gastrectomy versus conventional distal gastrectomy:
Furthermore, sensitivity analysis was performed to assess the influence of each individual study on the pooled estimate. Figure 3 shows that the study conducted by Nunobe et al. 17 seemed to be the most influencing single study on the overall pooled estimates. After this study was omitted, heterogeneity of gastritis, esophagitis, and bile regurgitation was not detected. Moreover, the sensitivity analysis indicated high stability of results. After that study was removed, the estimated ORs (95% CI; P value) were 0.16 (0.09, 0.28; P<.001) (Fig. 3A) for gastritis, 0.12 (0.05, 0.27; P<.001) (Fig. 3B) for bile regurgitation, and 0.18 (0.05, 0.72; P=.015; Fig. 3C) for esophagitis.
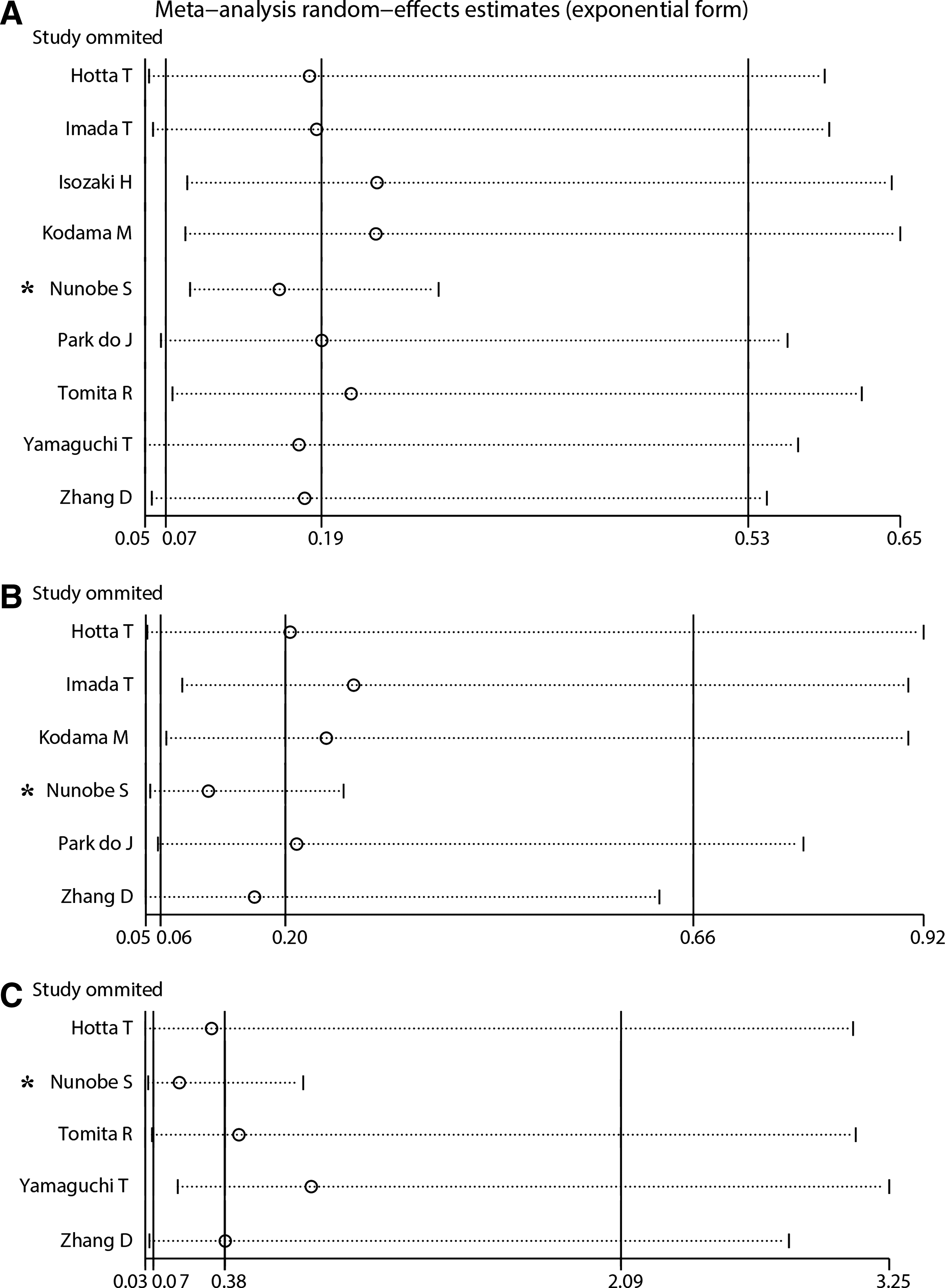
Influence analysis of the summary odds ratio for conventional pylorus-preserving gastrectomy versus conventional distal gastrectomy:
Publication bias
The Begg's funnel plot and Egger's test were performed to provide a diagnosis of the publication bias in the available literature. As shown in Table 2, the results suggested that gastritis, esophagitis, and gallbladder stones in the CPPG versus CDG group had potential publication bias (for gastritis, Egger's test=0.004, Begg's test=0.384; for esophagitis, Egger's test=0.025, Begg's test=0.462; for gallbladder stones, Egger's test=0.033, Begg's test=0.462). We further used the Duval and Tweedie “trim and fill” method to detect and adjusted the bias, and the results did not change. The shapes of the filled funnel plot based on random-effects meta-analytic point estimates for gastritis and esophagitis did not reveal obvious evidence of asymmetry (Fig. 4A and B, respectively). However, the funnel plot for gallbladder stones seemed to indicate asymmetry (Fig. 4C).
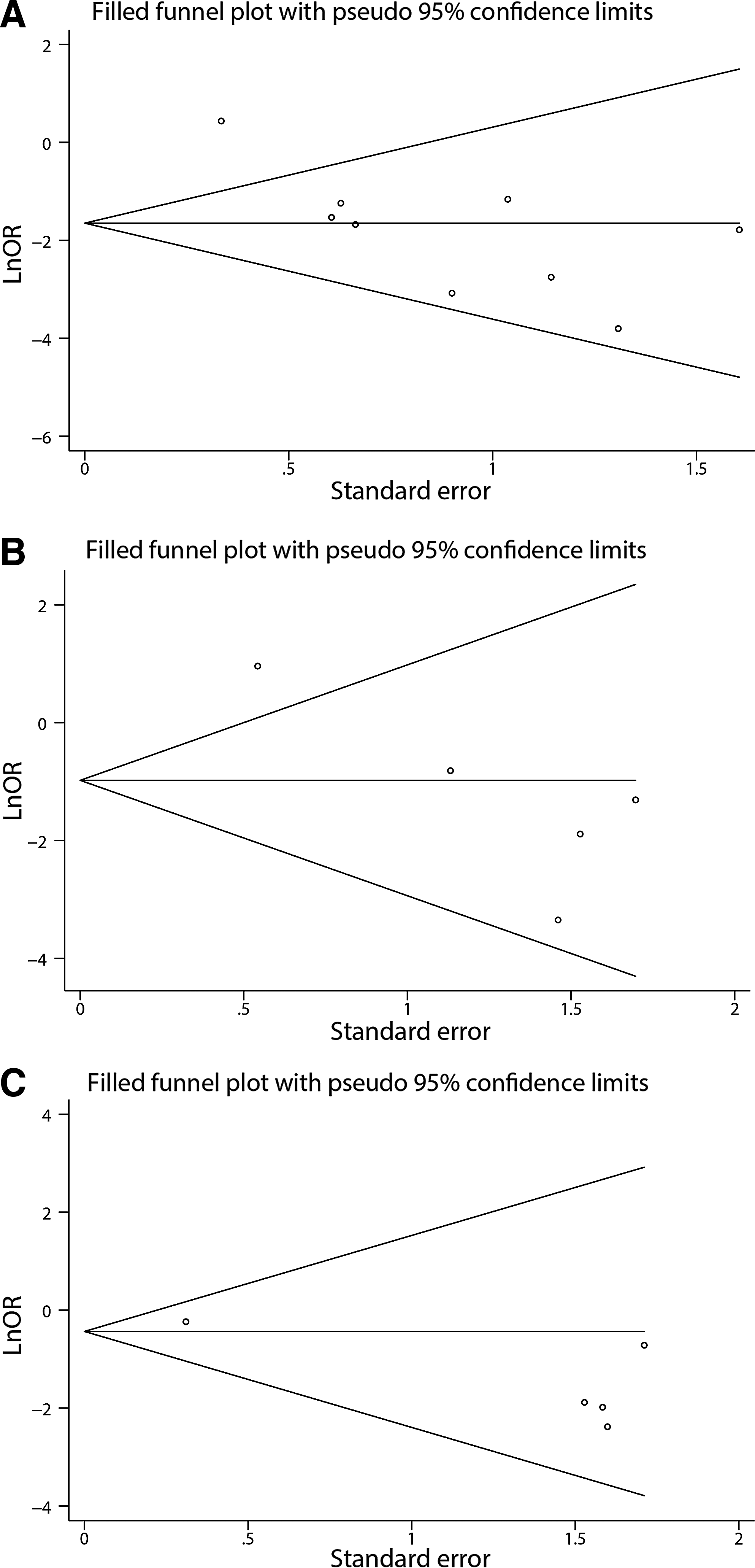
Filled funnel plot based on random-effects meta-analytic point estimates for publication bias test:
Discussion
Reconstructive procedures, such as Billroth-I, Billroth-II, and Roux-en-Y, have been performed commonly for patients following distal gastrectomy because of their simplicity. However, they often caused dumping syndrome, gastritis, and bile regurgitation, which would affect the quality of life for these patients. The PPG procedure, with limited stomach resection and antral cuff preservation, is a function-preserving surgery. Debate on improving postoperative quality of life made the function of PPG still controversial. Thus, we performed this meta-analysis to evaluate the value of PPG. With the development of endoscopic techniques, the laparoscopic approach is now being widely used with the aim of achieving minimally invasive therapy for gastric cancer.30–32 So our meta-analysis contained five studies that compared LPPG with LADG.
In this meta-analysis, it was demonstrated that CPPG has several benefits, such as the prevention of early dumping syndrome, duodenal juice reflux, gastritis, and regaining of weight compared with CDG. In addition, we found that the serum albumin level, late dumping syndrome, esophagitis, and the incidence of gallbladder stone were not different between the two groups. However, the incidence of gastric stasis after CPPG was higher than after CDG. The one RCT enrolled 36 patients for PPG and 38 for CDG. 33 It was reported that PPG has an advantage in terms of early dumping syndrome over CDG. No difference was found in serum albumin level and gallstone incidence. These results in the RCT did not conflict with those in our meta-analysis. Nevertheless, our meta-analysis, based on a comprehensive literature search, gave relatively reliable conclusions. Besides, we also evaluated more postoperative outcomes such as gastritis, bile regurgitation, esophagitis, and recovery body weight ratio. Currently, the development of endoscopy has penetrated into all areas of surgical treatment. Laparoscopic-assisted gastrectomy has aroused interest among many surgeons owing to its minimal invasion and low levels of pain. LAPPG versus LADG meta-analysis showed that operation time was significantly shorter in the LAPPG group, whereas postoperative complications such as gastric stasis and anastomotic leak were not different between the two groups.
The length of the antral cuff preserved played an important role in investigating the postoperative evaluation. In the stratified analysis, we found that gastritis, bile regurgitation, and esophagitis occurred significantly less often after PPG than after CDG when a 1.5-cm length of the antral segment was preserved. However, there was no difference for gastritis, bile regurgitation, and esophagitis in the subgroup in which a >2.5-cm length of the antral cuff was preserved. Given that the number of studies in the subgroup having a >2.5-cm length of the antral cuff preserved was small, we should treat this finding with caution.
To maintain the pyloric function, the root of the right gastric artery, the infrapyloric vessels, and the hepatic, pyloric branch of the vagus nerve were routinely preserved.6,34 As a result, the station No. 5 lymph node was not dissected during PPG, which might be worrisome in terms of oncologic safety and lead to an increased risk of cancer recurrence and death. According to previous reports, about 10%–32 % of EGC patients had micrometastasis.35–37 When focused on the station No. 5 lymph node, the rate of micrometastasis might be much lower than in other reports. 38 Moreover, the overall 5-year survival rate of patients with EGC who undergone PPG was 96.3%. 8 Considering the overall 5-year survival rates were 95%–100% and 85%–95% for patients with mucosal and submucosal cancer following gastrectomy, respectively,4,39 the survival rate for PPG was not worse. In addition, Suh et al. 29 reported that the 3-year recurrence-free survival rates were 98.8% for patients who underwent LADG and 98.2% for those who underwent LAPPG, which was not significantly different. In summary, PPG appeared to be oncologically safe and achieved an equivalent long-term prognosis to other gastrectomies.
However, the following limitations in this meta-analysis should be considered. First, we only identified one RCT, so high-quality meta-analysis of RCTs could not be performed. Second, because the operations using unified methods did not compare results during the same period and with the same surgeons, the possibility of bias could not excluded. Third, we were unable to analyze some important outcomes, including gastric emptying function and gallbladder emptying function, owing to lack of available data. Fourth, a high level of heterogeneity was detected for gastritis, bile regurgitation, and esophagitis in the CPPG versus CDG group, which may be due to the results of the study conducted by Nunobe et al. 17 The study appeared to be distinguished from other studies because of the following reasons: (1) surgical procedures may be different from the others, in particular, the length of the antral cuff preserved ranged from 2.5 to 6 cm; and (2) gastritis, bile regurgitation, and esophagitis were all the endoscopic findings, and the criteria of this study were different than those of the other studies. 40 Fifth, we only evaluated perioperative or postoperative outcomes for LAPPG versus LADG because of the lack of literature regarding long-term outcomes. Finally, the total sample size was small, and all the participants came from Asia, so there was a potential publication bias. Thus, more studies are needed from other racial groups to evaluate the benefits of PPG.
In conclusion, PPG is a safe and feasible surgical procedure for middle-third EGC. In contrast, because of the limited data, we cannot consider PPG is totally better than CDG or LADG. However, with the benefits of prevention of early dumping syndrome, duodenal juice reflux, gastritis, and regaining of weight, PPG can be an excellent option for experienced surgeons. Well-designed multicenter RCTs are still needed to confirm the benefits of PPG.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.