
Abstract
Abstract
Fetal hydrothorax is associated with significant mortality. However, the development of fetal thoracoamniotic shunting has reduced the mortality rate. Fetal thoracoamniotic shunting can be characterized by significant complications, such as intrathoracic dislodgement of the catheter. The ideal management of dislodged catheters postnatally is not known. We report two newborns with a prenatal diagnosis of fetal hydrothorax who underwent thoracoamniotic shunting complicated by intrathoracic dislodgement of the catheters requiring thoracoscopic removal of the shunts in the neonatal period.
Introduction
F
Case Reports
Case 1
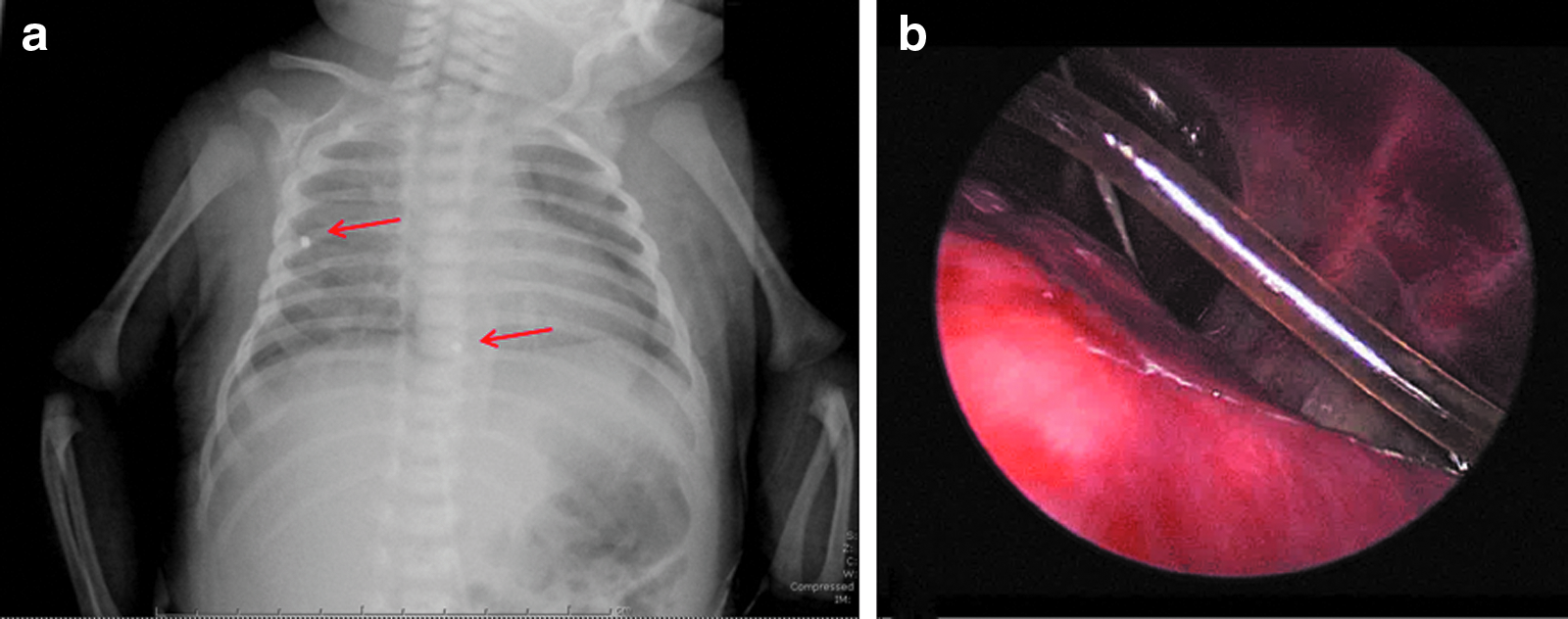
A gravida 3 para 2 woman was referred to our Center of Perinatal Surgery because of evidence of fetal hydrops in primary bilateral hydrothorax at 27 weeks of gestation. No associated anomalies were found. At a different institution, bilateral thoracoamniotic shunt pigtail catheters were positioned at 30 weeks of gestation with complete resolution bilaterally of the fetal hydrothoraces. A female newborn, weighing 3805 g, was delivered at 37 weeks by spontaneous vaginal delivery. Apgar scores were 8 and 10 at 1 and 5 minutes, respectively. The left catheter was removed immediately after birth, whereas the right one was not visible. The baby was stable with no need for respiratory support. A chest radiograph revealed the right catheter inside the right hemithorax with extension into the right paracardiac region (Fig. 1a). An ultrasound suggested that the catheter was positioned in the fissure between the right upper and the right middle lobe. Based on the concern about the risk of hilar strangulation, the decision was made to perform thoracoscopy to remove the catheter on Day 5 of life. The site where the shunt had been placed was not visible on the chest wall, and two 3-mm ports were inserted: one beneath the tip of the scapula and the other along the posterior axillary line, after induction of pneumothorax at 6 mm Hg. The catheter was identified in the fissure and was easily removed under vision with a grasper (Fig. 1b). No chest tube was left. Operative time was 35 minutes. The postoperative course was uneventful.
Case 1.
Case 2
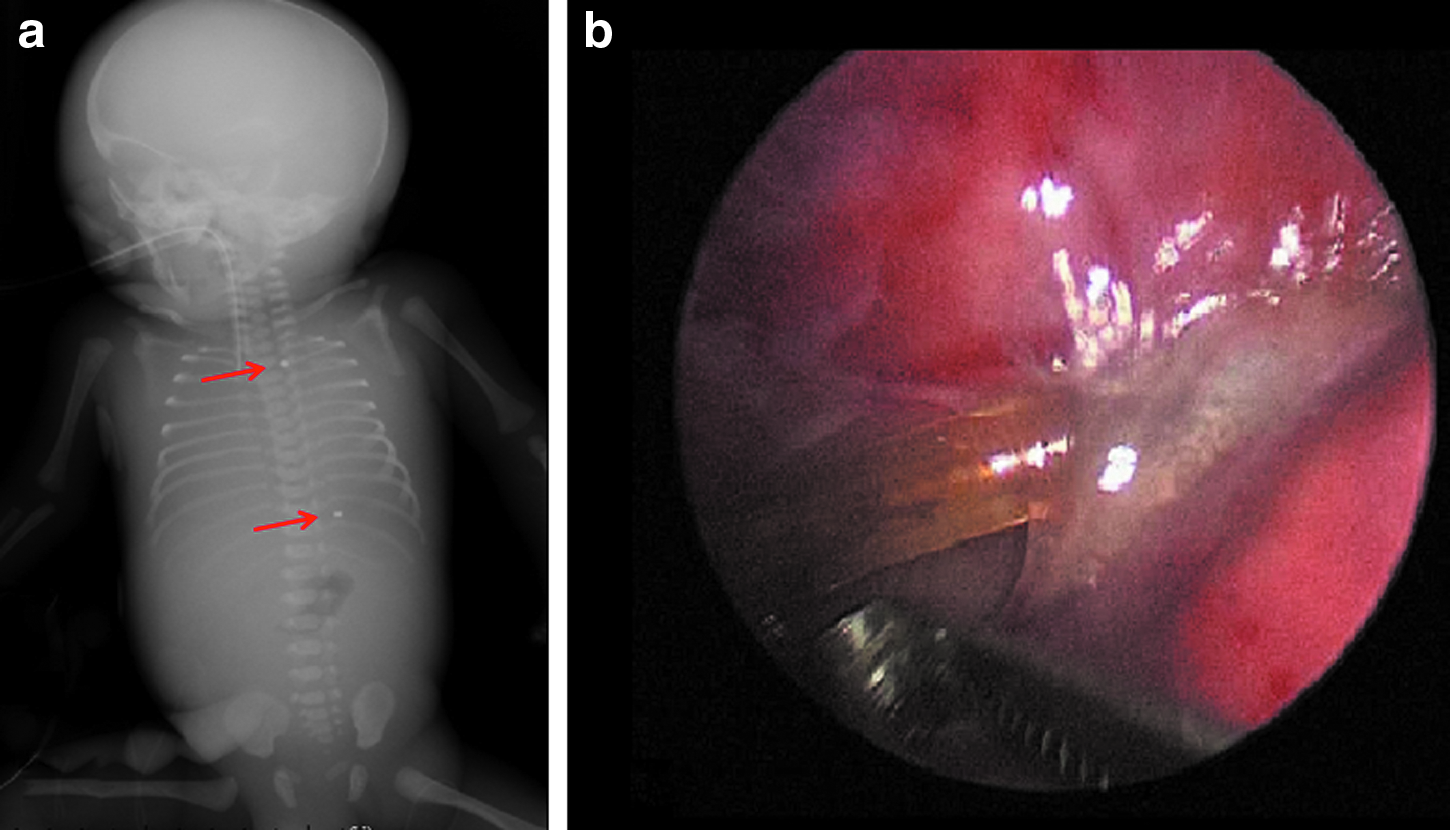
A gravida 1 para 0 woman was referred to our Center of Perinatal Surgery because of suspected primary bilateral hydrothorax and fetal hydrops at 23 weeks of gestation and drained with bilateral thoracoamniotic shunt pigtail catheters that were inserted at a different institution at 27 weeks. Prenatal ultrasound scans revealed the persistence of a left hydrothorax (24×49 mm). A male baby was delivered at 29 weeks through cesarean section due to maternal indications. Birth weight was 1880 g, and the newborn was apnoic, requiring intubation and mechanical ventilation. The right catheter was removed at birth, whereas the left one was not visible on the chest wall. A chest radiograph demonstrated that the catheter was located in the left paravertebral region along the course of the intrathoracic aorta (Fig. 2a). There was a large left pleural effusion requiring a left chest tube that initially drained 120 mL of pleural fluid. After stabilization of the patient and resolution of the hydrothorax, the decision to surgically remove the catheter was made. Thoracoscopy was performed on Day 14 of life. As in the previous case, the site where the shunt had been placed was not visible on the chest wall, and two 3-mm trocars were inserted, one beneath the tip of the scapula and the other one along the posterior axillary line. With insufflations to 5 mm Hg, the catheter was located in the left paravertebral region, where it was enveloped by fibrous tissue (Fig. 2b). Careful removal of the catheter was performed bluntly with a grasper. A chest tube was not left. Operative time was 30 minutes. The postoperative course was complicated by a left pneumothorax that was successfully drained with a chest tube placed on the first postoperative day.
Case 2.
Discussion
The outcome for fetuses with hydrothorax is strongly influenced by different factors: the gestational age at birth, the presence or absence of other congenital anomalies or hydrops, and the degree of pulmonary hypoplasia and hemodynamic impairment. Fetal thoracoamniotic shunting has been shown to be effective and can reverse the hydrops and prevent death. 4
Although rare, dislodgement of the shunt into the fetal chest can occur. This may be due to the internalization of the intraamniotic segment due to growth of the chest wall or fetal respiratory movements. It may also be secondary to misplacement of the device at initial placement. Nothing is known about the specific causes of catheter dislodgement as the devices were not positioned in our institution, and the patients were only subsequently transferred to our Center because of the lack of a pediatric surgery department in the initial center.
The decision of placing a thoracoamniotic shunt on both sides for bilateral hydrothoraces can be argued and is not generally part of our practice. In fact, the bilateral effusions can be considered as part of the hydrops spectrum, and treating one side usually leads to the resolution of the contralateral hydrothorax. Placing two shunts would furthermore increase the risk of complications. In our Center we place on average 10 shunts per year, and an additional shunt is added in bilateral effusions only for reaccumulation of fluid. In the last year this happened in 1 out of 5 patients (20%) with bilateral hydrothoraces.
Different postnatal strategies in managing thoracoamniotic shunts have been proposed. Some authors13,14 have suggested conservative treatment without surgical removal. Their follow-up (24 and 12 months, respectively) did not revealed significant complications. Infections or respiratory distress was not reported in their series. Other authors have reported significant perinatal morbidity and mortality due to retained shunts. Blanch et al. 8 reported a case where abnormal position caused strangulation of the pulmonary hilum, resulting in neonatal death. Other authors have advocated retrieving the shunt 15 when a thoracic surgical procedure was required postnatally. Primary reason for us to advocate removal of the catheters was their position and concern for injury to the pulmonary hilum as a result. In fact, in both cases they were located in the mediastinum next to the lung hilum, so that they were considered at high risk of fatal complications. In addition, the limited number of reported cases and the short follow-up do not offer specific validated indications. However, because of the increasing accuracy of prenatal diagnosis and the widespread of fetal thoracoamniotic shunts, the number of thoracoamniotic shunting procedures will certainly rise, leading to the need for specific guidelines and standardized management protocols for a dislodged catheter. We suggest removing intrathoracic dislodged catheters sooner rather than later, once the patient has been stabilized, in order to avoid the risk of fibrous and inflammatory response that may make removal of the shunt more difficult.
To the best of our knowledge, this is the first report of totally thoracoscopic removal of retained thoracoamniotic shunts. Thoracoscopy was considered as the procedure of choice thanks to its advantages: clear visualization of the thoracic cavity, removal under direct vision avoiding lesions to organs and vessels, small incisions, and reduced postoperative course.
Conclusions
Thoracoscopic removal of dislodged thoracoamniotic shunt catheters in newborns is a safe and effective procedure. We believe that centralization of such rare cases in dedicated perinatal surgical centers with well-established fetal and neonatal surgical skills is mandatory to improve the clinical outcome and reduce mortality.
Footnotes
Disclosure Statement
No competing financial interests exist.