
Abstract
Abstract
Background:
Partial splenectomy is preferred to total splenectomy when possible to reduce the risk of life-threatening infection. Several techniques have been described, each with its merits. Laparoscopic transection with monopolar saline-cooled radiofrequency coagulation has not been previously described.
Patients and Methods:
Two patients with enlarging cystic splenic lesions consented to laparoscopic partial splenectomy. In 1 case, high-power saline-cooled monopolar radiofrequency transection was performed with a laparoscopic sealing hook; the procedure was performed with a rigid resectoscope and ball diathermy in the other.
Results:
Both cases were performed without complications. Transection with the resectoscope and ball diathermy was combined with selective clamping of the splenic hilar vessels and was performed in 100 minutes with estimated blood loss of 250 mL. Transection with the sealing hook was performed in 80 minutes without hilar vessel clamping, with an estimated blood loss of 100 mL. No additional hemostatic agents were required for either case.
Conclusions:
Laparoscopic partial splenectomy can be performed with monopolar saline-cooled radiofrequency for parenchymal transection and hemostasis in a simple and effective manner.
Introduction
T
Laparoscopic splenectomy is now the preferred technique in the elective setting with significantly reduced blood loss, morbidity, and postoperative length of stay.8,9 Although there are large series reporting outcomes of laparoscopic splenectomy, the data are far more limited for laparoscopic partial splenectomy. Some of the techniques described for parenchymal transection during partial splenectomy include use of ultrasonic dissectors, the LigaSure™ (Covidien, Mansfield, MA) device, 10 endovascular stapling,11,12 and laparoscopic radiofrequency ablative needles. 13 Each technique has its potential utility without clear evidence that one is superior over the other.
We report a technique of laparoscopic partial splenectomy using high-power monopolar saline-cooled radiofrequency coagulation. We used a rigid resectoscope with ball diathermy in 1 case and a laparoscopic sealing hook in the other.
Operative Techniques
Case 1
A fit 19-year-old woman was referred with an enlarging splenic cyst that was causing mild intermittent discomfort. Over a period of 12 months the mass had grown several centimeters. Hydatid serology was negative.
On ultrasound and computed tomography imaging (Fig. 1), a superior pole splenic cyst measuring 10×9×8 cm, with a single septation, was noted. There was no retroperitoneal lymphadenopathy or other intraabdominal cystic lesions. The patient consented to operative intervention given her increasing abdominal symptoms and enlargement of the splenic cyst over the period of observation.
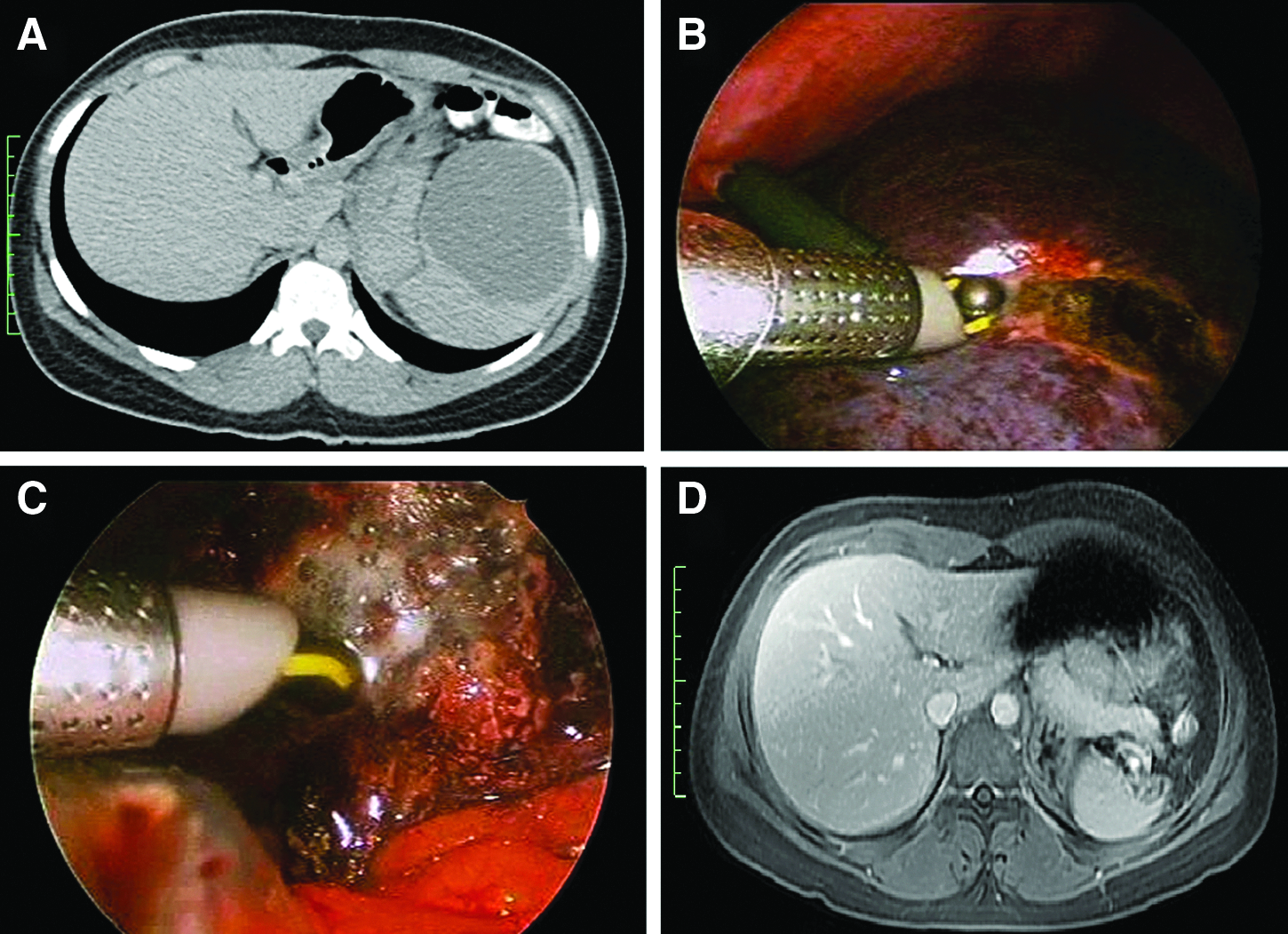
Case 1.
The patient was positioned in a standard right lateral decubitus position for possible total splenectomy. One 11-mm and two 5-mm ports were inserted in the left upper quadrant. A laparoscopic 5-mm LigaSure device was used to divide the short gastric vessels supplying the upper splenic pole. The hilum of the spleen was dissected, and a laparoscopic bulldog clip (Aesculap Inc., Center Valley, PA) was applied to the upper and middle pole vessels. This produced a clear region of splenic ischemia. Transection lines were then marked with a standard laparoscopic diathermy hook just within the ischemic region. Transection was then performed predominantly with the resectoscope introduced through the ports using ball diathermy set at coagulation setting of 120 W (spray), connected to a ForceTriad™ generator (Covidien) with a saline drip irrigation set-up to prevent tissue charring (Fig. 1). Occasional large crossing vessels were clipped with a 5-mm Endo Clip™ (Covidien) applicator prior to being coagulated with the diathermy set-up. In some cases the vessel needed to be divided with scissors after being clipped and coagulated. The bulldog clamp on the hilar vessels was removed after complete transection of the spleen. Bleeding points on the cut surface were further treated with the ball diathermy set-up. The total blood loss was approximately 250 mL. The operative procedure time was 100 minutes. The specimen was placed into a large endocatch bag and removed through extension of the 11-mm port site. The patient made an uncomplicated recovery and was discharged home 4 days following surgery. The final pathology was consistent with a benign simple splenic cyst. Follow-up computed tomography 1 month after surgery confirmed no residual cysts or perisplenic collections.
Case 2
A 56-year-old woman was referred with an incidentally enlarging splenic cyst over 24 months of observation. She was otherwise well with no comorbidities. Hydatid serology was negative. Magnetic resonance imaging demonstrated a 5-×5-×4-cm cyst in the superior pole of the spleen's multiple internal septations (Fig. 2). The cyst had almost doubled in size since initial detection. The patient declined the option of further observation and consented to operative intervention.
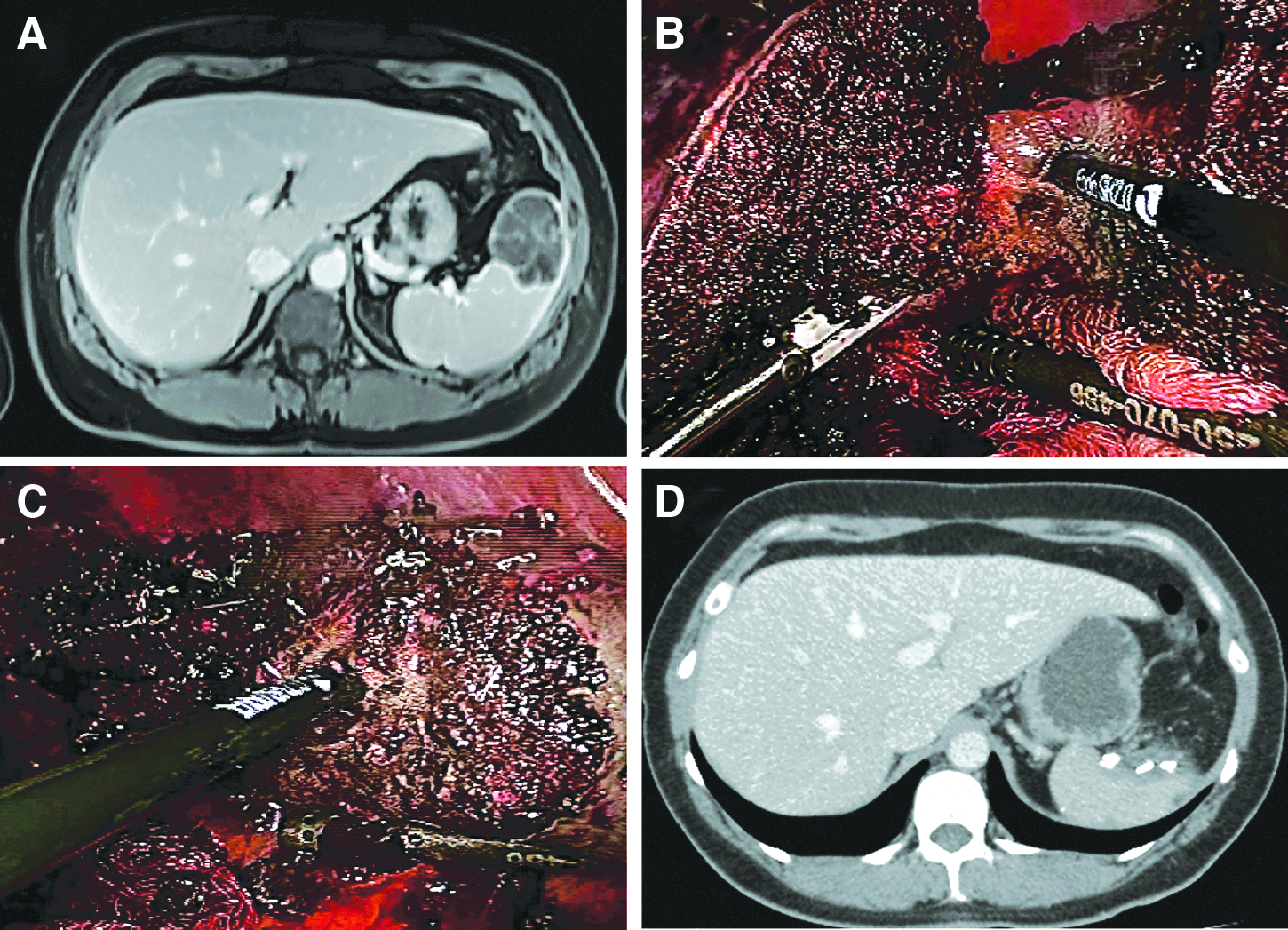
Case 2.
A standard laparoscopic splenectomy approach was once again undertaken. The LigaSure device was used to divide the short gastric vessels supplying the upper spleen pole. Intraoperative ultrasound was then undertaken and clearly showed confinement of the cyst to the upper pole of the spleen. The region of the spleen for transection was marked with hook diathermy and was in the nonischemic portion of the spleen in this case. Transection of the spleen was then performed cautiously with the Endo SH2.0™ laparoscopic sealing hook (Medtronic, Minneapolis, MN) device at a coagulation setting of 120 W (spray) connected to the ForceTriad generator with a saline drip irrigation set-up. Occasional large traversing vessels were clipped with 5-mm clips prior to division for added security. Total blood loss was 100 mL. The operative time was 80 minutes. The patient made an uncomplicated recovery and was discharged home on Day 4 postoperatively. Histopathology confirmed a completely excised intrasplenic lymphangioma. A magnetic resonance imaging follow-up scan 1 month postsurgery showed no residual cyst or collections (Fig. 2).
Discussion
Partial splenectomy, retaining at least 25% of normal spleen volume, is thought to be required to retain its immunological functions. 14 Partial splenectomy is preferred when it can be performed safely. Various techniques have been described, mainly in the setting of open surgery. The basic premise of any technique is to allow spleen transection, while insuring complete hemostasis. 10 To our knowledge, the use of high-power monopolar saline-cooled radiofrequency ablation for splenic transection has not been described previously.
The use of ultrasonic dissectors to divide the spleen parenchyma is most frequently reported, particularly in the setting of partial splenectomy in children with specific hematological disorders.11,12 In such cases hilar vessels are generally divided with endovascular staplers or a similar device to create an ischemic zone, prior to parenchymal transection. Minor bleeding from the parenchyma can then be managed with cautery or application of hemostatic agents such as Surgicel® (Johnson & Johnson, New Brunswick, NJ). 11 The use of the LigaSure device to transect the spleen has also been described. 10 Other techniques include radiofrequency ablation of the spleen by insertion of radiofrequency needles (LeVeen® needle electrode; Boston Scientific Corp., San Jose, CA). 13 This is usually performed 5 mm within the ischemic demarcation line after hilar vessel ligation, and the ablated region is then divided using scissors. A similar technique using a four-needle radiofrequency system has also been reported (Habib® 4X laparoscopic sealer device; Angiodynamics, Fremont, CA), dividing in between the coagulated tissue. Transection of the parenchyma using staples following crush clamping of the spleen has also been described. 15
In the majority of laparoscopic and open partial splenectomy cases, parenchymal transection follows ligation of hilar vessels, usually with ties, clips, or staplers, which creates a region of ischemia that minimizes blood loss.11,15,16 In some cases preoperative embolization of hilar vessels has been used in an attempt to reduce blood loss.12,17 Embolization in itself is not complication free, and these cases have the potential for abscess formation, spontaneous splenic rupture, and a common postembolization syndrome of fever, pain, and vomiting. 18
Application of the radiofrequency ablation technique using a laparoscopic hook or a floating ball via a rigid resectoscope has not been described previously. The use of the floating ball device with saline irrigation has, however, been described for open partial splenectomy. 19 This device combines radiofrequency energy with continuous saline irrigation that bathes the “floating ball,” allowing high temperatures to be achieved that produce tissue ablation without charring and burning.20–22 Vessel sealing using this method is very effective. It is important that the laparoscopic hook applicator allows for both sealing and dissecting of vessels. Because of the nature of the splenic parenchyma, once the capsule is breached, the ball device acts as an effective dissecting tool. Larger vessels, once sealed, however, may need to be ligated with scissors in some cases. At times we elected to clip as well as coagulate larger vessels in our cases, although this may not be necessary. In 1 case transection was performed in a region of parenchymal ischemia following temporary clamping of the upper and midsplenic pole vessels. In the other case, although superior pole splenic vessels were sealed with the LigaSure device, transection of the spleen was through nonischemic parenchyma. The blood loss was similar in both cases. This suggest that prior ligation of hilar vessels with this technique may not be necessary and can be avoided to minimize risks of inadvertent major bleeding.
The effectiveness of saline-cooled laparoscopic radiofrequency transection of the spleen makes the need for additional hemostatic products to achieve coagulation of the cut spleen surface unnecessary. With many of the other described techniques, hemostasis requires use of additional devices such as the argon beam coagulator or the application of fibrin glue or similar products to the cut spleen surface.10,23,24 Additional hemostasis of the raw cut spleen can be achieved easily with application of the saline-cooled radiofrequency hook or ball probe to bleeding points on the spleen surface for several seconds. In open surgery, we use the ball diathermy with saline water irrigation to successfully achieve hemostasis in cases of inadvertent spleen injury, often when other techniques fail (authors' unpublished data). In these circumstances we use standard ball diathermy set at a coagulation power of 120 W (spray), to which we attached tubing that allows saline to be dripped onto the ball to prevent charring. In the 2 cases presented, we found the laparoscopic application of saline-cooled radiofrequency energy with a sealing hook or ball diathermy applied through a resectoscope to be equally effective.
In conclusion, partial splenectomy using radiofrequency energy with saline irrigation with a sealing hook or ball diathermy applied through a resectoscope appears to be an effective transection and hemostatic technique. Several aspects of this technique, such as consistent hemostasis, even without inflow vascular control, and the ease of application make this technique an appealing spleen transection method. Its superiority to other techniques would require further comparative studies.
Footnotes
Disclosure Statement
No competing financial interests exist.