
Abstract
Abstract
Background:
There are few reports of the laparoscopic findings of the internal inguinal ring (IIR) in patients with hydrocele. The purpose of this study was to assess the safety and efficacy of laparoscopic percutaneous extraperitoneal closure (LPEC) for hydrocele in comparison with that of open repair (OR) and compare the findings of the IIR between cases of hydrocele and inguinal hernia (IH).
Materials and Methods:
We analyzed 69 consecutive patients with hydrocele who underwent surgery at our institution between April 2009 and February 2014. The patients were divided into two groups (LPEC and OR) according to the procedure. Age, length of operation/anesthesia, and complications were compared. Concerning the findings of the IIR, we classified the features into three categories, as follows: Type 1, flat; Type 2, narrow patent processus vaginalis (PPV) with a peritoneal veil; and Type 3, widely opened PPV. We then compared these findings between the cases of hydrocele and IH treated with LPEC during the study period.
Results:
Among a total of 69 patients, 40 underwent LPEC, and 29 underwent OR. There were no significant differences in the length of operation/anesthesia and complications. No recurrences were observed in either group. The findings of the IIR were mostly classified as Type 2 (59.1%) among the cases of hydrocele and Type 3 (92%) among the cases of IH.
Conclusions:
LPEC is a safe and effective procedure for treating hydrocele. The findings of the IIR differ between cases of hydrocele and IH.
Introduction
H
We adopted the use of laparoscopic percutaneous extraperitoneal closure (LPEC) 2 in cases of hydrocele in April 2009. Although the laparoscopic approach for pediatric inguinal hernia (IH) has prevailed, even in pediatric surgery, there are few reports regarding the efficacy of laparoscopic surgery for the treatment of pediatric hydrocele.1,3–5 In addition, little is known about the laparoscopic findings of the internal inguinal ring (IIR) in cases of hydrocele.
The purpose of this study was to assess the safety and efficacy of LPEC for hydrocele compared with OR and evaluate the morphological findings of the IIR in cases of hydrocele compared with those observed in cases of IH.
Materials and Methods
We retrospectively reviewed 69 consecutive patients with pediatric hydrocele surgically treated at the Department of Pediatric Surgery of Hyogo College of Medicine, Hyogo, Japan, between April 2009 and February 2014. The patients were divided into the LPEC group or the OR group according to the procedure. Age, preoperative diagnosis, postoperative diagnosis, operative time, anesthesia time, and complications were compared between the two groups.
The authors retrospectively evaluated the IIR on operative videos in every case. The intraoperative findings of the IIR were assessed during LPEC for hydrocele (hydrocele affected side and contralateral side). As the control, the findings of the IIR in boys (>12 months of age) who underwent LPEC for IH during the same period at our institute were also evaluated (inguinal hernia affected side). The findings of the IIR were classified into three categories according to the report of Chin et al., 6 as follows: Type 1, flat without a peritoneal slit; Type 2, PPV covered with a peritoneal veil; and Type 3, widely opened PPV (Fig. 1).
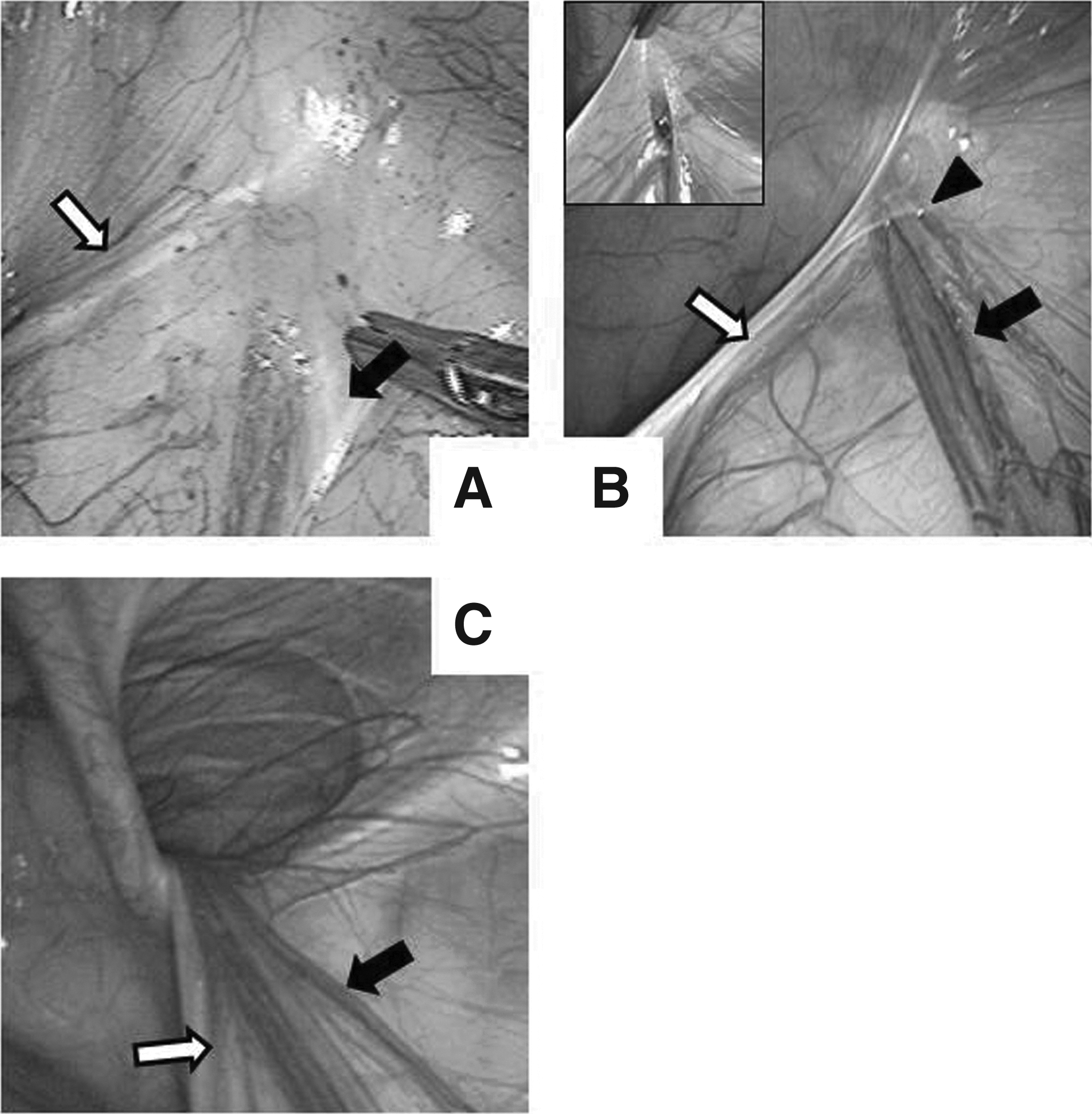
Intraoperative findings of the internal inguinal ring.
The diagnosis of hydrocele was made by pediatric surgeons based on clinical manifestations and physical examination and ultrasonography findings in all cases. The indications for surgery were age >12 months and concomitant contralateral IH regardless of age. The procedures (OR and LPEC) and respective possible complications were explained to the parents, who selected the procedure. The LPEC procedure is characterized with a circuit suturing with a straight needle, Lapaherclosure™ (Hakko Medical Co., Tokyo, Japan), which has a wire loop to hold and release the suture material. The details of the procedure are described in the legend of Figure 2. We used 2-0 nonabsorbable sutures in every case. When the hydrocele wall could be confirmed laparoscopically, it was incised electrically to open the hydrocele. At the end of the operation, if the hydrocele had not diminished, we punctured it via the trans-scrotal approach.
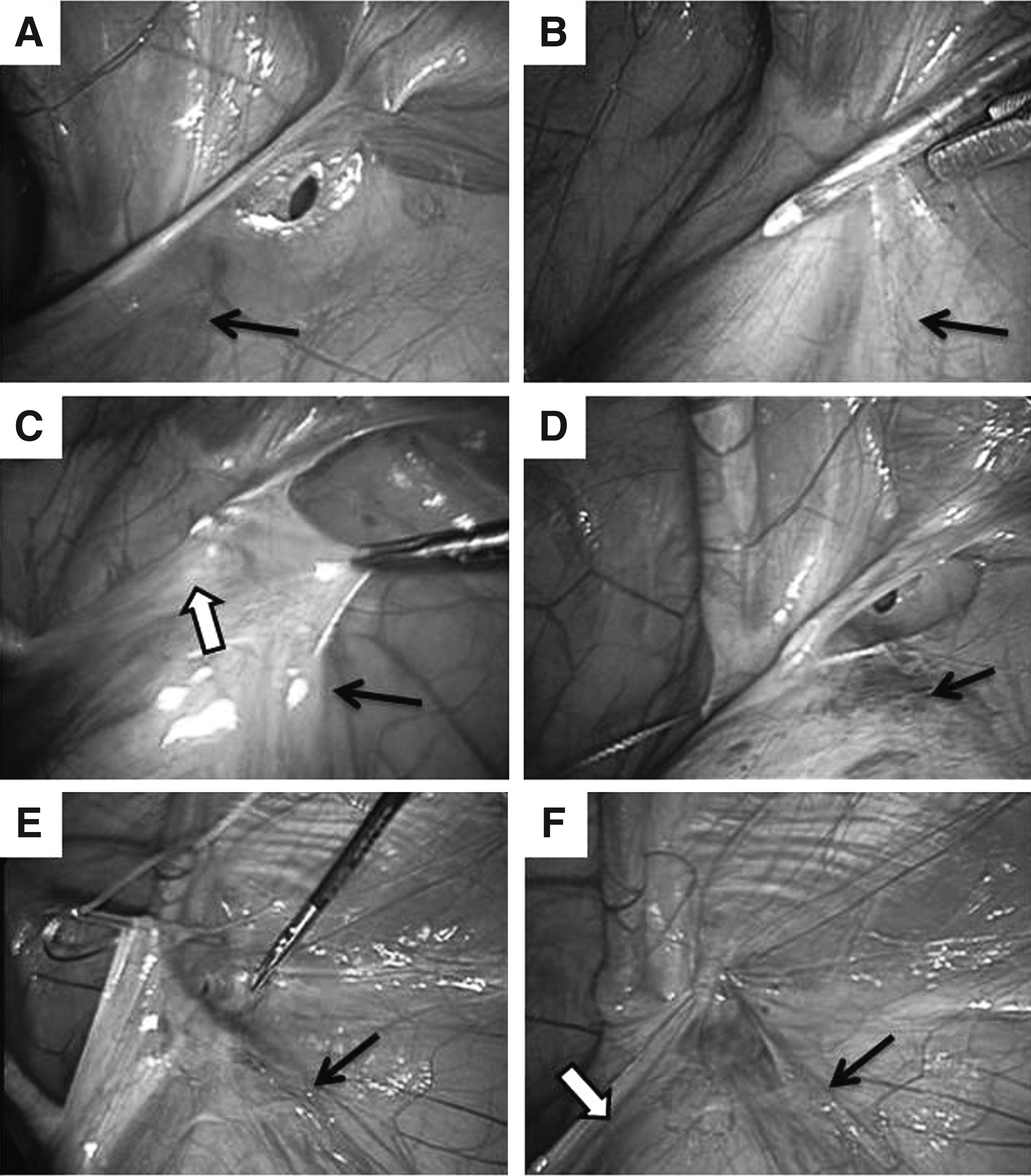
Intraoperative findings of laparoscopic percutaneous extraperitoneal closure (a case of right-sided hydrocele).
Statistical analyses
Continuous data are expressed as mean±standard deviation values. The statistical significance was calculated using Student's t test and the chi-squared test. All statistical analyses were performed with the JMP software program (version 10; SAS Institute Inc., Cary, NC). A value of P<.05 was considered to be statistically significant.
Results
The patient demographics are given in Table 1. There were no significant differences in age or body weight at surgery between the LPEC and OR groups. There were no significant differences in the laterality of the preoperative presentation between the LPEC and OR groups. The length of follow-up was significantly shorter in the LPEC group. One patient in the OR group had previously undergone OR for a contralateral hydrocele. Two patients underwent surgery at <12 months of age because of concomitant contralateral IH (1 in the LPEC group, 1 in the OR group).
Data are mean±standard deviation (range) values.
LPEC, laparoscopic percutaneous extraperitoneal closure; OR, open repair.
There were no intraoperative complications in either group. Although 1 patient in the LPEC group with abdominoscrotal hydrocele (ASH) required an additional working port, no conversion to OR was experienced. In the LPEC group, 22 of 36 (61.1%) cases of the preoperative unilateral manifestation of hydrocele were found to involve contralateral PPV intraoperatively, all of which were closed with LPEC.
A comparison of the length of operation/anesthesia and recurrence between the two groups is given in Table 2. There were no significant differences between the two groups in the length of operation/anesthesia. The postoperative course was uneventful in all patients, and no cases of recurrence were observed in either group.
Data are mean±standard deviation values.
LPEC, laparoscopic percutaneous extraperitoneal closure; OR, open repair.
The findings of the IIR on the preoperatively affected side were mostly categorized as Type 2 in 26/44 sides (59.1%) in the cases of hydrocele and Type 3 in 46/50 sides (92%) in the cases of IH (Table 3). We closed the IIR on the contralateral side if the IIR exhibited Type 2 (14 cases, 38.9%) or 3 (8 cases, 22.2%) features (22/36 cases, 61.1%). There were significant differences in the type of IIR between the patients with hydrocele and IH (P<.001).
Various forms of IIR and hydrocele were confirmed using laparoscopy (Fig. 3). Drainage of hydrocele was performed laparoscopically in 3 cases, including 1 case of ASH (Fig. 3D). Percutaneous aspiration was performed at the end of the operation in 5 cases. In the remaining cases, the hydrocele fluid drained into the peritoneal cavity with compression of the scrotum and groin. In all cases in both groups, the hydrocele was found to have diminished by the week after surgery. Although postoperative swelling of the scrotum was observed in approximately half of the OR cases, no patients in the LPEC group exhibited a swollen scrotum.
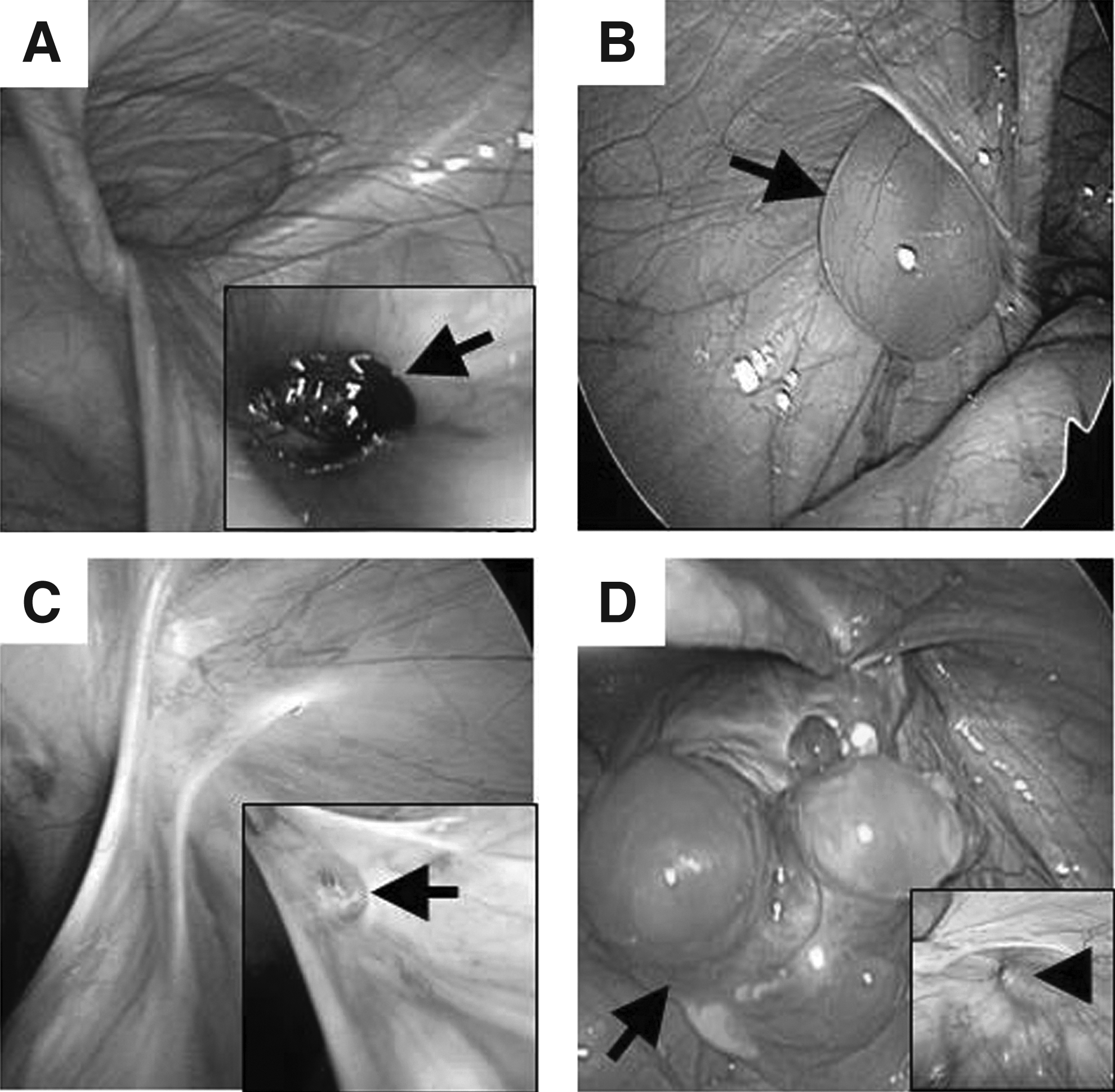
Various types of hydrocele.
Discussion
Hydrocele is a common entity in pediatric surgery, and closure of the PPV with or without drainage of hydrocele via an inguinal incision (OR) is commonly performed. Although OR is thought to be safe, this procedure has been reported to be the most common cause of iatrogenic injury to the vas deferens. 7 As a less invasive technique, the “scrotal approach” has been advocated; however, the indication for this procedure is recommended to be limited to patients >12 years of age. 8 To date, there have been few reports on the laparoscopic approach for hydrocele.1,3–5 The laparoscopic approach should have an advantage of magnification, resulting in safer dissection of the vas deferens and testicular vessels from the PPV. LPEC is a simple procedure that involves circuit suturing of the IIR without the need for an incision in the PPV. Dissection is performed with a straight 19-gauge needle; therefore, the extent of dissection of the vas deferens and vessels can be minimized.
Although more parents recently have chosen LPEC in our institute, the length of follow-up was significantly shorter in the LPEC group compared with the OR group. This is one of the limitations of our study. Although the length of operation/anesthesia was not statistically significantly different between the two groups in this study, this parameter tended to be longer in unilateral cases and shorter in bilateral cases in the LPEC group. In the LPEC group, more time was spent for insertion of the first trocar and closure of the abdomen, with a difference of approximately 10 minutes between the unilateral and bilateral cases. In contrast, in the OR group, the bilateral cases required two procedures compared with the unilateral cases. Although our patient population was relatively small, LPEC may be safe and efficient for treating pediatric hydrocele in the same manner as IH. 9 The rate of long-term complications, such as infertility due to obstruction of the vas deferens, should be compared between these patient groups in the future.
The findings of the IIR may indicate a high rate of patency of the processus in cases of hydrocele. For some IIRs in the patients with hydrocele, the peritoneal veil was difficult to distinguish; however, we were able to detect the PPV, which was either widely opened or covered with a peritoneal veil in 97.7% of cases. Although we did not find a communication between the PPV and hydrocele in every case, at a minimum, the processus was opened at the level of the IIR excluding 1 case (Type 1). In our series, only 1 patient exhibited Type 1 features, indicating the presence of “noncommunicating” hydrocele during inguinal exploration. In this case, we performed LPEC to ligate any microscopic communication (or PPV). At the time of operation, the size of the hydrocele was relatively small; therefore, percutaneous aspiration was not performed. One week after LPEC, the hydrocele diminished spontaneously in this case. Matsukawa 10 compared the features of the cord-like remnant between the processus and hydrocele microscopically and found a continuous lumen in all cases. Therefore, performing simple high ligation of the PPV is essential for treating a hydrocele, whereas creating an incision of the hydrocele may be unnecessary. The incidence of a closed processus during inguinal exploration has been reported to be 6.3% (12/190). 11 Wilson et al. 8 reported that the proportion of cases of “noncommunicating” hydrocele increases according to the patient's age and that approximately one-quarter of cases involve noncommunicating hydrocele, even among patients 0–5 years of age. This difference may be due to the differences in view point (inguinal or intraperitoneal) and the use of pneumoperitoneum. The processus, if patent, is dilated via pneumoperitoneum, and magnifying the area using laparoscopy makes it easy to distinguish the orifice of the processus.
The findings of the IIR in the cases of hydrocele differed from those observed in the cases of IH. Although almost all patients with IH displayed Type 3 features, Type 2 characteristics were most frequent among the patients with hydrocele. These morphological differences in the IIR may contribute to differences in symptoms. For example, Chin et al. 6 reported an age-dependent decrease in the detection of PPV and increase of the frequency of peritoneal veil (Type 2 in our study). It is interesting that, in that study, the incidence of a flat peritoneal floor was almost constant, regardless of age. The spontaneous obliteration of the PPV may lead to veiled depression, whereas incomplete closure of the PPV results in Type 2 features.
Although the laparoscopic findings revealed various forms of hydrocele as well as IIRs, it was possible to perform the LPEC procedure uniformly, regardless of the types of hydrocele or IIR. A case of ASH was observed in the LPEC group. In that case, performing intraperitoneal drainage of the ASH was easy, and LPEC was subsequently performed without difficulty. The pathogenesis of ASH may be the same as that observed in other types of hydrocele, including incomplete closure of the PPV. LPEC is thought to be feasible in cases of ASH as well as simple hydrocele.
The limitations of our study were the relatively small patient population and the possibility of selection bias on the procedure. Further investigations including the long-term complications in larger populations will be required.
Conclusions
LPEC is a safe procedure for treating pediatric hydrocele. The findings of the IIR in cases of hydrocele tend to reflect a narrow PPV with a peritoneal veil.
Footnotes
Disclosure Statement
No competing financial interests exist.