
Abstract
Abstract
Esophagogastric fistula is a rare complication related to severe inflammation at the gastroesophageal junction. Most causes are related to severe gastroesophageal reflux disease, previous surgery, or malignancy. This is the case of a 72-year-old man who had a laparoscopic Nissen fundoplication. He developed an esophageal obstruction from an intraesophageal pledget. It was removed laparoscopically, and the esophagotomy was buttressed with a Nissen fundoplication. Two months later he developed severe dysphagia, and an esophagogastric fistula was diagnosed. This was a large fistula measuring 20 mm in diameter. A novel hybrid technique was used to divide the fundoplication. Under endoscopic guidance, a 12-mm balloon-tipped trocar was inserted transgastrically. A linear-cutting surgical stapler was used to divide the fundoplication and reopen the gastroesophageal junction. The patient had no further dysphagia or gastroesophageal reflux.
Introduction
E
Case Report
A 72-year-old man presented to the clinic with substantial dysphagia. He had undergone a laparoscopic paraesophageal hernia repair with Nissen fundoplication 3 months earlier at another institution. This was complicated by severe, persistent dysphagia. Despite multiple endoscopic attempts at dilation, he was unable to eat or drink. He was also having difficulty tolerating his own saliva. He was admitted to the hospital where an endoscopy was performed. His gastroesophageal junction was strictured. It could only accommodate a pediatric endoscope. There was a foreign body suggestive of an intraesophageal Teflon® (Dupont, Wilmington, DE) pledget. He was given parenteral nutrition for several days prior to laparoscopic exploration. When his fundoplication was taken down, it was apparent that the sutures and pledgets used on his fundoplication had led to partial necrosis of the anterior wall of his esophagus. This was closed primarily over a nasogastric tube. The fundoplication was reconstructed over this esophagotomy. He had drains and a gastrostomy tube placed.
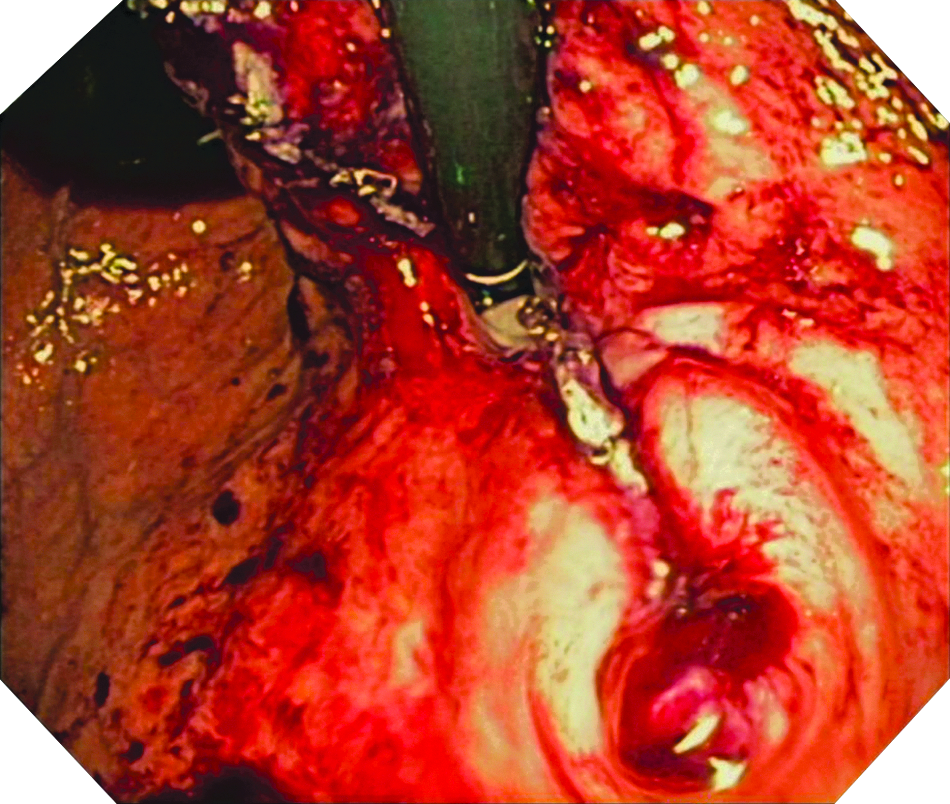
On postoperative Day 5, an esophogram was negative for leak or obstruction. He was initiated on a liquid diet. He tolerated this without difficulty and was discharged home. He was advanced to a regular diet over several weeks. Over the course of the next few months, he began to have progressively worsening dysphagia. This failed to respond to dilations. He was sent to a gastroenterologist for stenting of his gastroesophageal junction. Following stent placement, he had horrendous gastroesophageal reflux disease. He could not eat and was intolerant of tube feeds. The stent was removed, and he was referred back to his surgeon. At this point, he could not tolerate any solid foods. Anything more than sips of water led to severe odynophagia. Manometry was performed that did not reveal any esophageal spasm or esophagogastric junction obstruction. An endoscopy revealed a double-lumen esophagus. Near the gastroesophageal junction, a large lumen was present to the left with a smaller opening inferior and to the right. This represented a large esophagogastric fistula (Fig. 1). Based on the endoscopic findings, the fistula was from the esophagotomy to the anterior fundus, where the fundoplication had been constructed. Surgical options were discussed, including attempted endoscopic closure, partial esophagectomy, and transgastric division of his fistula. Because this fistula was to the anterior fundus, it was assumed this would remain well vascularized despite operative division. The patient elected to proceed with transgastric division using a combination of laparoscopic instrumentation with endoscopic guidance.
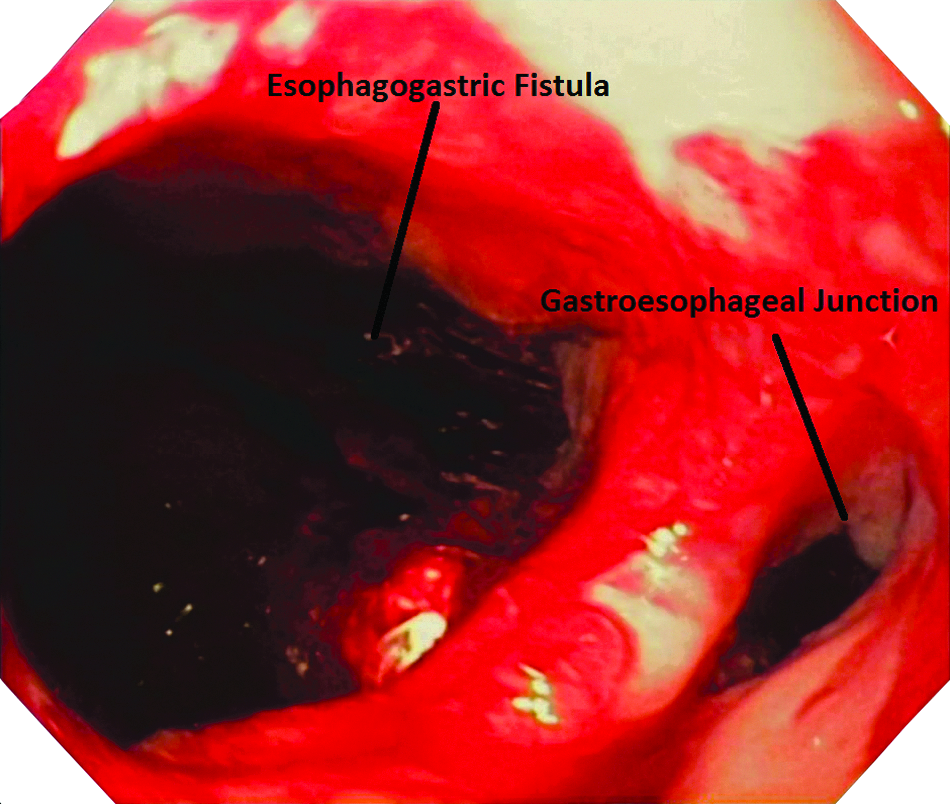
Endoscopic visualization of the esophagogastric fistula with the gastroesophageal junction to the right and the esophagogastric fistula to the left.
Procedure
A 5-mm trocar was placed near the umbilicus. This functioned as the camera port. The stomach was insufflated with CO2. We then placed a 12-mm balloon-tipped trocar (Applied Medical, Rancho Santa Margarita, CA) into the stomach by performing an anterior gastrotomy under endoscopic guidance. This was placed near the inferior greater curvature of the stomach. The balloon was then inflated and pulled tight against the abdominal wall. This allowed the stapler to be directly in alignment with the anterior portion of the fundoplication that we were about to divide. The endoscope was used for visualization of the transgastric portion of the procedure. We performed a retroflex view of the gastroesophageal junction through both the fistula and the gastroesophageal junction. This was critical during manipulation of the stapler as it prevented a reversed image. Once the stapler was through the fistula and gastroesophageal junction (Fig. 2), the endoscope was retracted into the esophagus (Fig. 3). The anterior fundoplication was divided using blue loads on the powered stapler (open staple height of 3.5 mm). This is reflected in Figures 4 and 5. The 12-mm port was removed from the intragastric location. The gastrotomy was closed with the stapler. A nasogastric tube was left for decompression. Two drains were placed near the hiatus.
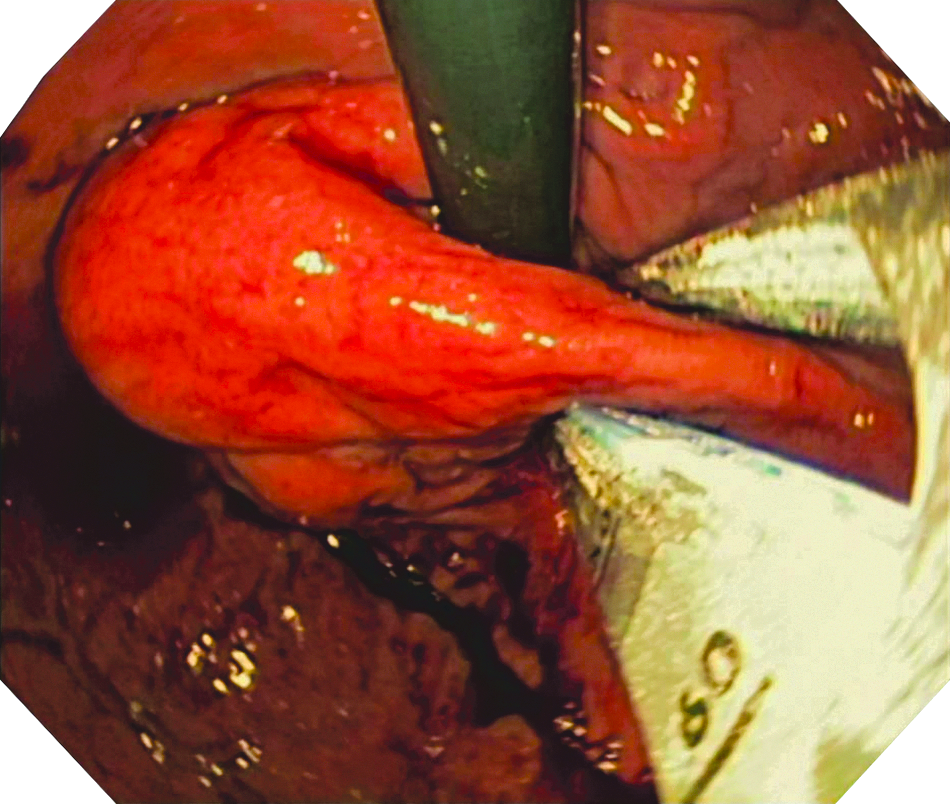
Retroflexed visualization of the stapler.
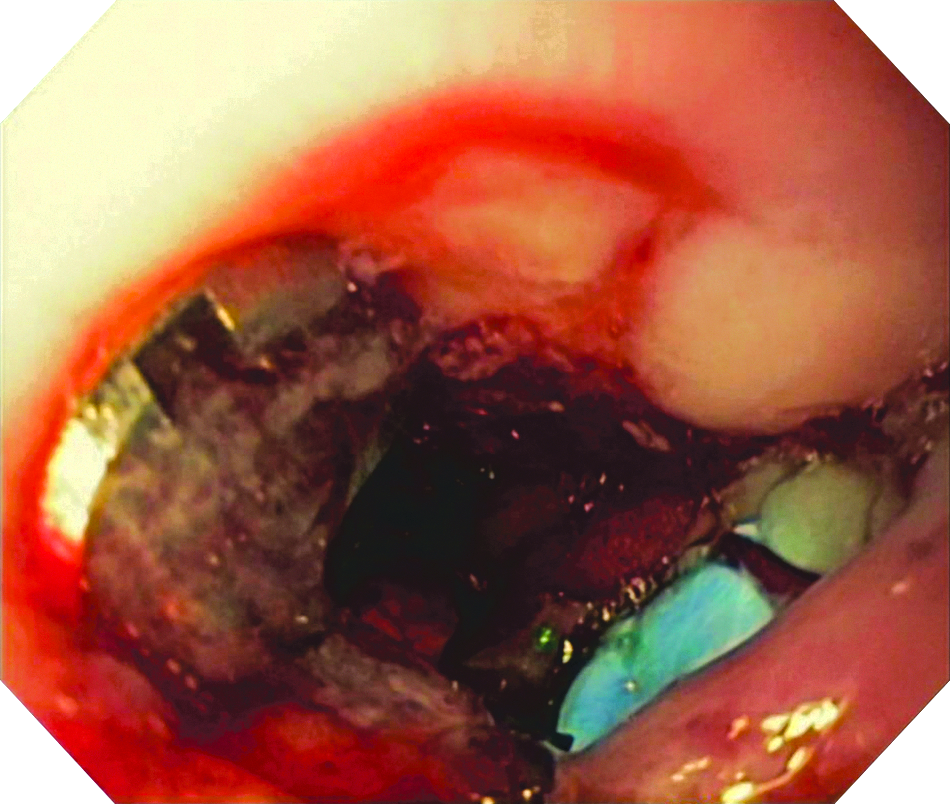
Visualization of the stapler from within the esophagus.
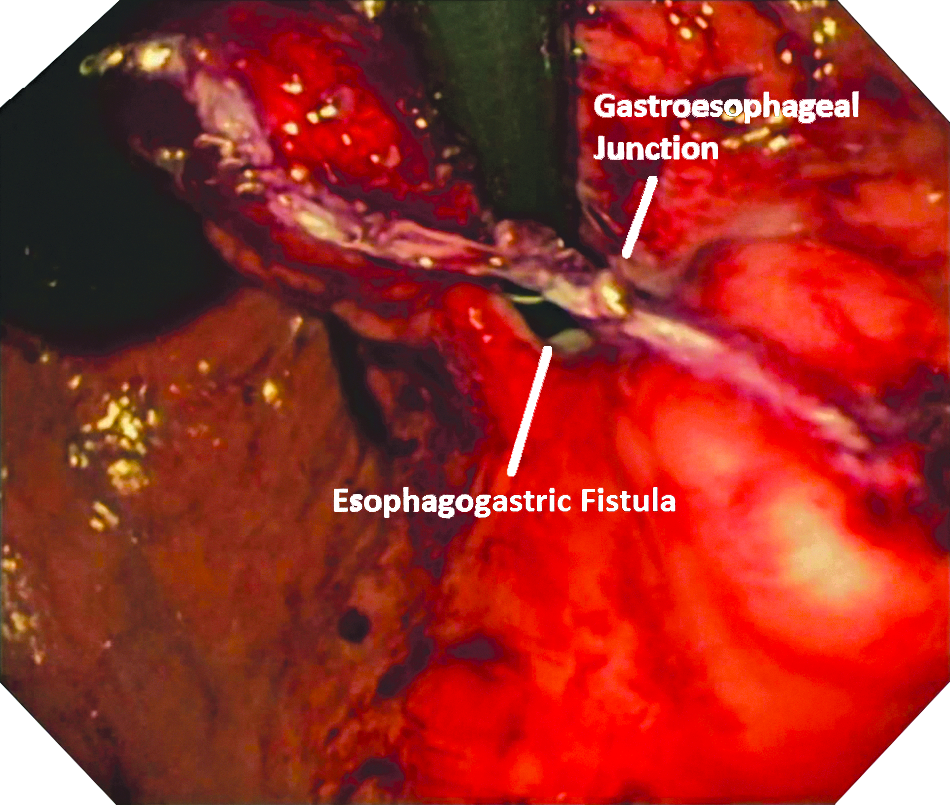
Retroflexed visualization of partial division of the fundus.
Retroflexed view of complete division of the fistula and reopening of the gastroesophageal junction.
Clinical course
On postoperative Day 3, he underwent an esophagram that demonstrated normal passage of contrast into the stomach and no leak. He had not undergone an esophagram since his fistula was diagnosed. He was initiated on a liquid diet. His diet was advanced over 2 weeks to regular food. Both drains were discontinued. Four months postoperatively he is free of all dysphagia. He has no complaints of gastroesophageal reflux disease. His gastrostomy tube has been removed. Prior to the division of this fistula, he had been completely dependent on gastrostomy feeds for his nutrition.
Discussion
Esophagogastric fistulas have long been recognized as a rare, potential complication of gastroesophageal reflux disease and fundoplication. This was first described in 1975 following an esophageal surgery for strictures; although there were 2 cases, only 1 case required an operation. 1 In 1980, a case of multiple, nonsurgical esophagogastric fistulas was described; this case was believed to be secondary to severe reflux esophagitis. 2 In 1986, Fleming and DiMagno 3 reported a series of 2 patients with an esophagogastric fistula following Nissen fundoplication; 1 patient had developed an esophageal ulcer, whereas the second patient had an esophageal cancer. An additional case report found a Teflon pledget had led to an esophagogastric fistula at the time of fundoplication; this required an additional operation and prolonged convalescence. 4 An additional small case series 5 in 1996 demonstrated 2 patients with “double-lumen esophagus”; 1 case was secondary to perforation at the time of fundoplication, and the second was likely related to gastroesophageal reflux disease. At that time, no surgical therapy was believed to be helpful. 5 Patients can still develop an esophagogastric fistula from gastroesophageal reflux disease if they do not receive treatment for it, but it has become much less common in the era of proton pump inhibitor therapy. 6 Thus, most modern cases are likely iatrogenic. Since 1975, there have been 10 cases of esophagogastric fistula described in the literature. In our case, an esophagram when the patient first developed dysphagia (6 weeks following removal of his pledget) demonstrated a single-lumen esophagus with delayed transit through the gastroesophageal junction. This stricture coupled with serosal apposition over the esophagotomy likely led to the development of the fistula. It is our belief that with the gastroesophageal junction being strictured, the gastroenterologist unknowingly stented the esophagogastric fistula. This would explain the severe reflux and intolerance of gastrostomy feeds following its placement.
Although the phenomenon of esophagogastric fistulas has been relatively well described, its management has been unclear. When related to esophageal reflux, the management has been antireflux medications and conservative therapies. Most of these fistulas are relatively small. When related to previous operations, the management has been medical with few surgical interventions. Operations attempted included partial esophagectomy, resection and primary closure, and thoracotomy with transgastric division. Unfortunately, the endoscopic dilations failed to demonstrate any meaningful improvement. As endoscopic therapies changed, some attempted closures of small fistulas from esophagogastric junction surgeries using endoscopic suturing devices, stents, and clips have been reported with varied success. Only a single case report exists in the literature of endoscopic repair. 7 Theoretically, this would be an alternative for small fistulas. Our fistula was large. There has been 1 case in which a double-lumen esophagus was repaired through a gastrotomy on a child with two previous fundoplications; this was performed through a thoracotomy and involved transgastric division of the fistula and Collis gastroplasty due to shortened esophagus. 8 Our case represents the first case in which a laparoscopic transgastric approach has been used to divide a large esophagogastric fistula and restore esophagogastric continuity.
Like many of the cases above, the patient had no symptomatic improvement with sequential dilation of his gastroesophageal junction. The procedure chosen used techniques commonly used for resection of submucosal tumors near the gastroesophageal junction, pancreatic cystgastrostomy, and removal of eroded adjustable gastric bands. This novel approach avoided the morbidity of major resection in an elderly, chronically malnourished patient while providing symptomatic relief.
Conclusions
Laparoscopic transgastric gastroplasty is a surgical alternative for esophagogastric fistula that avoids a major resection and its concomitant morbidity.
Footnotes
Disclosure Statement
No competing financial interests exist.