
Abstract
Abstract
This study investigated the impact of laparoscopic rectal cancer resection for patients with high operative risk, which was defined as American Society of Anesthesiology (ASA) grades III and IV. This study was conducted at a single center on patients undergoing rectal resection from 2006 to 2010. After screening by ASA grade III or IV, 248 patients who met the inclusion criteria were identified, involving 104 open and 144 laparoscopic rectal resections. The distribution of the Charlson Comorbidity Index was similar between the two groups. Compared with open rectal resection, laparoscopic resection had a significantly lower total complication rate (P<.0001), lower pain rate (P=.0002), and lower blood loss (P<.0001). It is notable that the two groups of patients had no significant difference in cardiac and pulmonary complication rates. Thus, these data showed that the laparoscopic group for rectal cancer could provide short-term outcomes similar to those of their open resection counterparts with high operative risk. The 5-year actuarial survival rates were 0.8361 and 0.8119 in the laparoscopic and open groups for stage I/II (difference not significant), as was the 5-year overall survival rate in stage III/IV (P=.0548). In patients with preoperative cardiovascular or pulmonary disease, the 5-year survival curves were significantly different (P=.0165 and P=.0210), respectively. The cost per patient did not differ between the two procedures. The results of this analysis demonstrate the potential advantages of laparoscopic rectal cancer resection for high-risk patients, although a randomized controlled trial should be conducted to confirm the findings of the present study.
Introduction
D
Patients and Methods
Patients, diagnoses, and staging
This study included 248 patients who had high operative risk as well as rectal cancer at Ruijin Hospital (Shanghai, China) from October 2006 to November 2010. Patients with rectal cancer within 15 cm from the anal verge were included, and high operative risk was defined as patients with ASA Physical Status Classification System III or IV disease, such as the elderly (age >70 years old) with comorbidities, cardiac events (coronary disease, post-percutaneous coronary intervention, decompensated heart failure, post-cardiac valve replacement), respiratory dysfunctions (asthma, restrictive and obstructive dysfunction, severe chronic obstructive pulmonary disease), cerebrovascular and neurological disease, and liver and renal dysfunction. The attending anesthetist assigned the ASA grade to each patient after considering the patient's physical condition and comorbidities. The Charlson Comorbidity Index was used to add additional information to the ASA score in comparing the patients. 3 The diagnoses of these patients with rectal cancer were made preoperatively. The tumor node metastasis (TNM) staging system of the National Comprehensive Cancer Network 4 and the American Joint Committee on Cancer 5 was used. The diagnoses were next confirmed by postoperative pathology.
Group assignment
Patients were assigned preoperatively to the laparoscopic or open approach based on clinical criteria and imaging. Patients with a pelvic exenteration or multivisceral resection were assigned to the open surgery group (OpS group); patients' preference had also been considered. Cases for which conversion to an open procedure was deemed necessary remained in the laparoscopic surgery group (LapS group) for all outcomes by intention-to-treat analysis.
Surgical procedures and quality control
Patient, tumor, and treatment characteristics were collected routinely by trained registrars from the hospital records. The preoperative preparation and the techniques of the procedures were described in our previous publications, 6 and with our experience from open total mesorectal excision, laparoscopic surgery was performed according to the same oncologic principles.7,8 Postoperative adjuvant chemotherapy would be offered to the patients undergoing apparently radical surgery for nonmetastatic rectal carcinoma.
Statistical analysis
The results were subjected to a nonparametric Mann–Whitney U test. A paired Student's t test was also used to analyze the intragroup differences. Analyses were performed with Stat View version 5.0 for Windows software (SAS Institute Inc., Cary, NC). The chi-squared test or Fisher's exact test and Cochram–Artimage test were applied to analyze the categorical variables, as appropriate. A P value of <.05 was considered statistically significant. The Kaplan–Meier method was used to analyze the overall survival of patients. Cochran–Mantel–Haenszel statistics was used to analysis the differences of complication risk between the LapS and OpS groups after operations based on the age of patients, and the log-rank test was used to compare patient survival between groups.
Results
The initial search identified 1576 consecutive patients who underwent rectal resection. After screening by ASA grade, 248 patients who met the inclusion criteria were identified (Table 1). These two groups of patients had no differences in gender and age. There was no significant difference in Charlson Comorbidity Index distribution (P=.611). In the laparoscopic resection group, 16 patients met the inclusion criteria who had undergone previous abdominal surgery, with no significant difference from the OpS group. The center's experience found that laparoscopic surgery might be also suitable for these patients.
APR, abdominoperoneal resection; BMI, body mass index; F, female; ISR, intersphincteric resection; LAR, low anterior resection; M, male.
The postoperative complications included anastomotic leakage (5.7% versus 6.3%), ileus (5.7% versus 2.1%), intrapelvic abscess, arrhythmia (OpS=5 versus LapS=4 [data not shown]), heart failure (OpS=3 versus LapS=1 [data not shown]), stress ulcer, hypoproteinemia, cerebral infarction, and pneumonia; the specifics are listed in Table 2. Laparoscopic resection had a significantly lower total complication rate in 30 days (OpS=74.0%, LapS=43.8%; P<.0001). It is notable that the two groups of patients had no significant difference in cardiac and pulmonary complication rates. Thus, these data showed that the laparoscopic group for rectal cancer could provide short-term outcomes similar to those of their open counterpart with high operative risk. Laparoscopic resection also had a significantly lower pain rate (OpS=16.4%, LapS=2.8%; P=.0002). When the verbal rating scale was used to evaluate the pair scale after operation, the threshold was a value of >2. In addition, the LapS group had a significantly lower estimated blood loss, which was in accordance with the changes of hemoglobin level (P<.0001) during the resection (Table 2). Four cases (2.8%) in the LapS group were converted to open surgery in the present study, and the conversion were due to the presence of severe adhesion, hemorrhage, bulky tumors, and invasion to adjacent organs.
Also includes stress ulcer, electrolyte imbalance, etc.
Significant difference.
Hb, hemoglobin; VSR, Verbal Rating Scale.
The survival curves of patients with high operative risk who underwent laparoscopic and open surgery are shown in Figure 1. The 5-year actuarial survival rates were 0.8361 and 0.8119 in the LapS and OpS groups for stage I/II, respectively, without a significant difference (Fig. 1A). The 5-year actuarial survival rates in the LapS and OpS groups for stage III/IV were significantly different (P<.05), but among these patients, 2 in the OpS group and 1 in the LapS group suffered from multisource tumor or tumor recurrence, and 1 in the OpS group underwent renal operation before rectal cancer resection and died of renal disease. Once we removed the bias, further analysis suggested there was no significant difference between the two groups (P=.0548) (Fig. 1B). Patients with concurrent preoperative cardiac diseases who underwent laparoscopic resection had lower pulmonary complications and overall complications rates. However, the cardiac complications rate showed no significant difference. The overall survival rates of patients with cardiovascular or pulmonary diseases are shown in Figure 1C and D, respectively. In patients with preoperative cardiovascular disease, the 5-year survival curves of laparoscopic and open resection were significantly different (P=.0165), respectively, whereas in patients with preoperative pulmonary disease, the 5-year overall survival rates were significantly different (P=.0210).
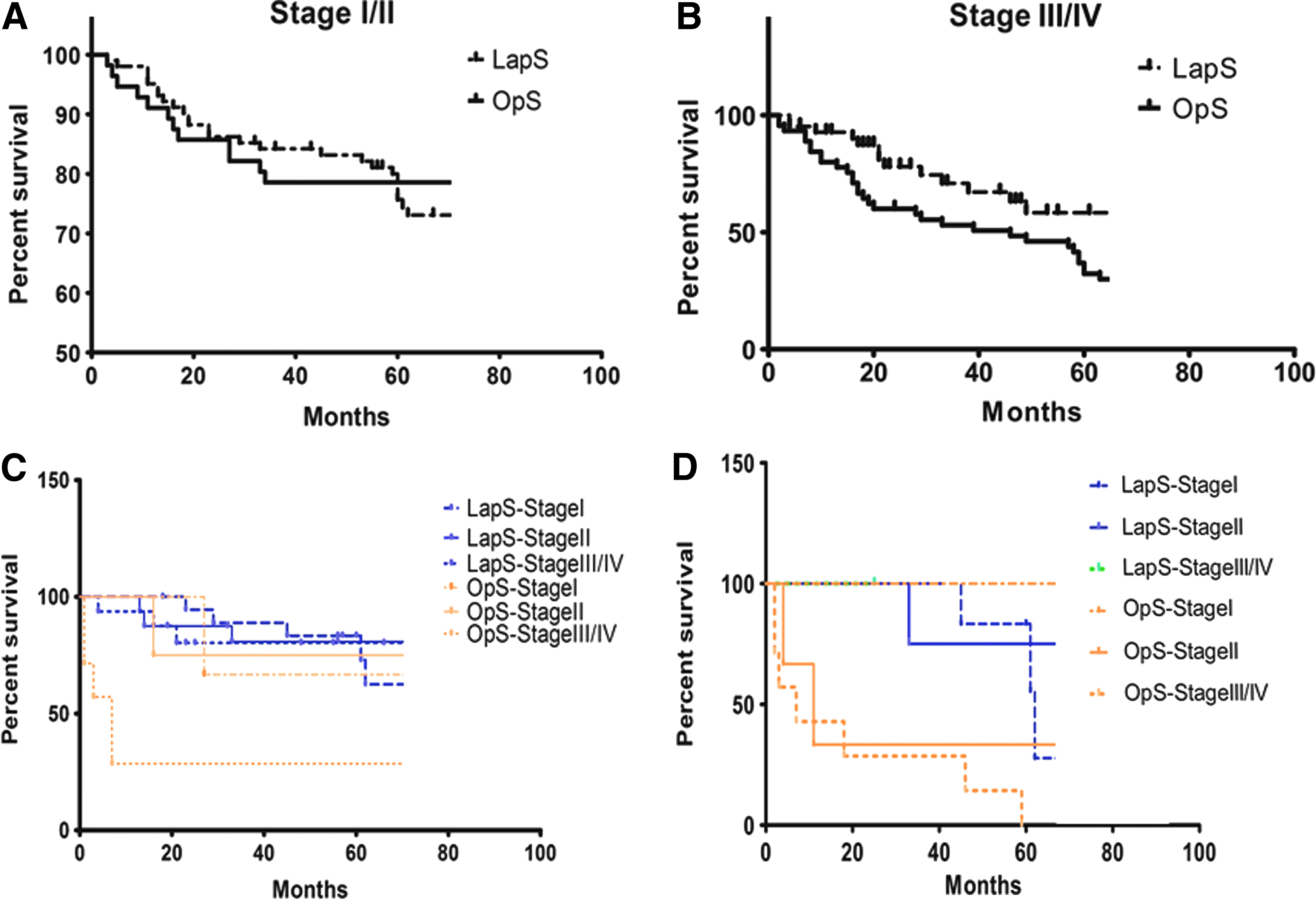
The overall survival of patients with high operative risk:
In the present study, we found that the in-hospital costs are almost the same between the two groups of patients with high operative risk, without a statistically significant difference (P=.9175; mean±standard error of the mean of LapS=3502.4±91.7; mean±standard error of the mean of OpS=3526.5±234.8). We divided the cost into various items (diagnosis, operative fee, anesthesia, pharmacy, blood or blood products, surgical instruments, daily room cost, and nursing). We found that despite the higher cost of medical devices, the difference in total cost between the LapS and OpS groups derives from savings in the preoperative and postoperative stages (Fig. 2B).
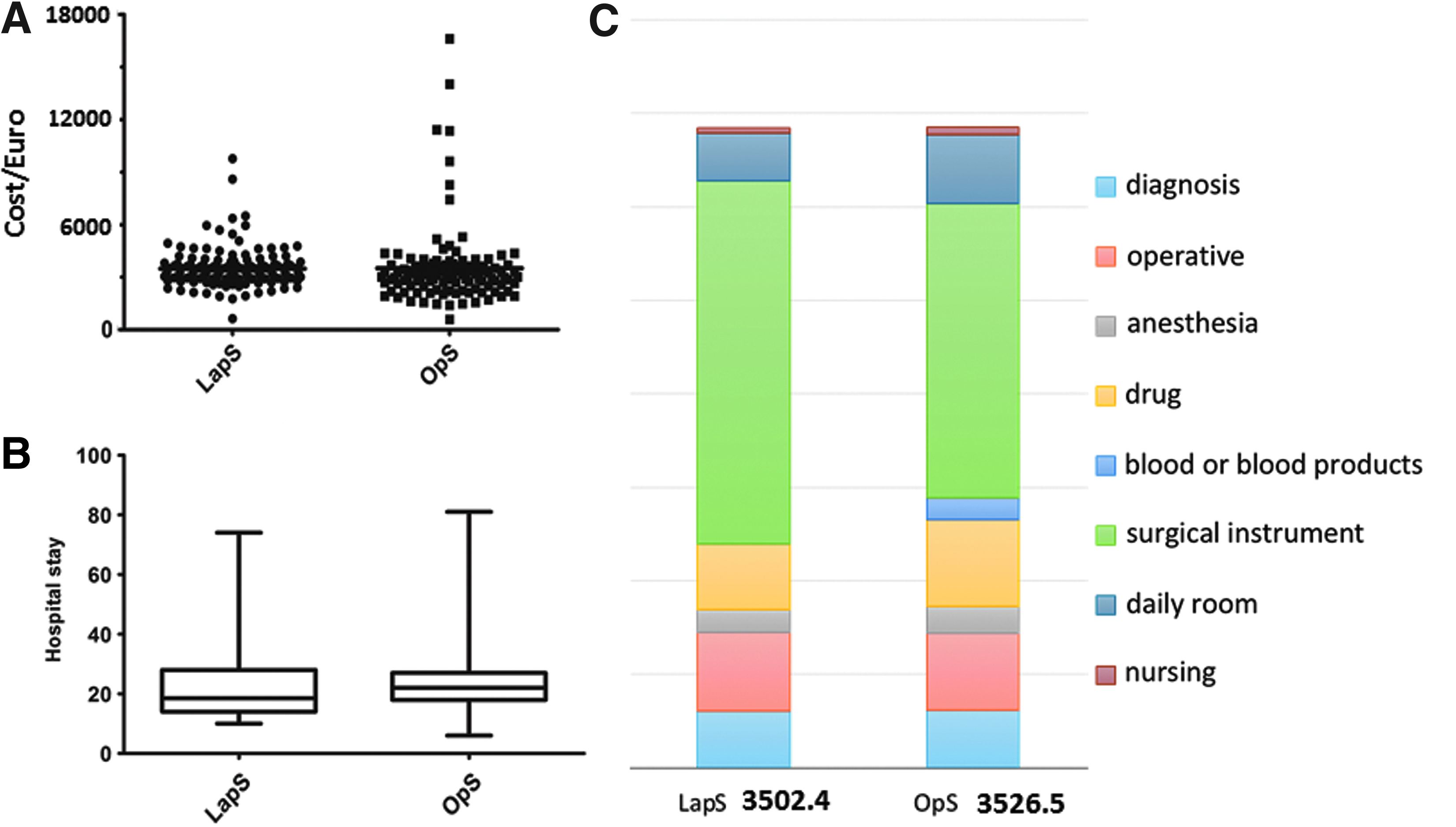
Statistical cost-efficiency analysis of patients by types of procedure:
Discussion
With the advances in technique, laparoscopic total mesorectal excision is now being performed more commonly, because of the excellent results of its feasibility 3 and favorable short-term outcomes regarding faster recovery of bowel motility, minimum stress response, and short hospital stay, especially in specialized centers.9–14 Laparoscopic surgery for colorectal cancer is associated with survival and recurrence rates equal to those of open surgery. 15 A recent meta-analysis also found no significant differences in overall morbidity and perioperative mortality rates between the two groups. 6 However, creation of pneumoperitoneum with carbon dioxide is potentially associated with adverse pathophysiological changes, including hypercapnia and reduced venous return, and it is still controversial for the patients with high operative risk because of the limitation of data on the outcome and complication rate. In addition, patients are most vulnerable when their preexisting comorbidities make them susceptible to perioperative risk.14,16,17
Several studies have claimed that the laparoscopic procedure lasts longer than open surgery but entails a shorter hospital stay. 18 Clinical evidence showed that laparoscopy shortened patients' hospital stay by 20.6% with respect to the open technique. 19 In the present study, the difference in length of hospital stay reach statistical significance for patients with high operative risk. In the center, patients need regular observation for 5–7 days after operation, for early detection and solution of complications such as anastomotic leakage, which may be the contributing factors for the observed longer hospital stay than in American/European series in this cohort.
From an economic perspective, some reports claim that laparoscopic surgery is more expensive than open surgery; on the other hand, a statistically significant difference was found for rectum procedures, for which the laparoscopy group costs were 14% lower than those of the laparotomy group in European hospitals. 20 However, in the present study the in-hospital costs were almost the same between the two groups of patients with high operative risk, without a statistically significant difference (Table 2 and Fig. 2A).
The overall rates of postoperative complication were similar between the two groups, but the LapS group had fewer pulmonary infections, which might be attributable to the enhanced postoperative recovery of lung function21,22 in the LapS group. In addition, laparoscopy might have an amplifying effect. It was reported that laparoscopic rectal cancer surgery can preserve the pelvic nerve, which induced less male sexual dysfunction, 23 but the same result was not seen in the present study.
However, the limitation of this research is that in our LapS and OpS groups, only 2.9% (3/104) and 1.4% (2/144) ASA grade IV patients were involved in the analysis, which could not reflect the operative comparison between patients in ASA grade IV, so this research focused on rectal cancer resection for patients with ASA grade III. Although a randomized controlled trial should be conducted to confirm the findings of the present study, we believe that the present study is of value in proposing the future studies.
Footnotes
Acknowledgments
The authors sincerely thank Yanye Yang, Kai Hu, and Hongchao Zhao for their much-appreciated administrative assistance during the course of this study.
Disclosure Statement
No competing financial interests exist.