
Abstract
Abstract
Background:
Single-incision laparoscopic colectomy (SILC) is one of several promising operation choices. Our previous study demonstrated that SILC with a self-made glove-port system both improves the feasibility of SILC and decreases the cost expense of surgery. Because the incision site for SILC could be made at either the umbilicus or McBurney's point, we are interested in whether the incision site affects the outcomes of patients, which is a less explored topic. The purpose of this study is not only to show the results of SILC with a self-made glove-port system for supporting its feasibility, but also to compare the short-term surgical outcomes between SILC with the incision made at the umbilicus and at McBurney's point.
Subjects and Methods:
We collected and reviewed the medical records of patients who received SILC with a self-made glove-port system for tumors in the left side of the colon from August 2009 to March 2011. All operations were performed by a single surgeon. Comparisons of the demographic characteristics, perioperative data, and clinical outcomes between umbilical and McBurney's SILCs were performed. Postoperative pain was assessed by a visual analog scale and opiate demand.
Results:
In total, 61 patients were enrolled in this retrospective study. Five of 48 (10.4%) tumors in the umbilical SILC group and 5 of 13 (38.5%) tumors in the McBurney's SILC group were located below the peritoneal reflection. The tumor location was significantly different between these two groups (P=.015). Patients in the umbilical SILC group had significantly higher frequency of opiate demand than those in the McBurney's SILC group (0.4±0.7 versus 1.4±1.8, respectively; P=.002).
Conclusions:
This study further provides evidence for supporting the safety and feasibility of SILC in treating colorectal diseases. More important is that McBurney's SILC not only alleviates the patient response to wound pain, but also provides the same site for a diverting enterostomy to avoid creating an additional wound.
Introduction
M
SILC is one of the SILS procedures and has been developed as an effective way to treat benign and malignant colorectal diseases because it has innovations in new access devices, instruments, and surgical techniques. 16 Therefore, SILC brings much more potential benefits compared with conventional laparoscopic colectomy.17,18 However, the challenges, such as instrument crowding, 19 the high cost of specially designed curved instruments, and the limitation of movement due to paralleled instruments, still remain in SILC and increase the difficulties of tissue manipulation and dissection.
Our previous studies as well as the reports of others have demonstrated that when SILC is introduced with a simple glove-port device18,20,21 by using a commercially available wound protector and surgical glove, it may both improve the feasibility of SILC and decrease the cost expense of surgery. It is worthy of mention that the single incision of SILC could be made not only at the umbilicus, but also at McBurney's point. Whether the site of single incision affects the outcomes of patients still remains unclear. The goal of this study was to evaluate the results of SILC using a self-made glove-port system and to compare the short-term surgical outcomes of SILC between umbilical and McBurney's incisions for tumors of the left side of the colon and rectum.
Subjects and Methods
Sample collection
The study was conducted to retrospectively collect the medical records of patients with tumors on the left side of the colon and rectum who underwent SILC using a self-made glove-port system via an umbilical or McBurney's incision wound from August 2009 to March 2011 at our institution. All the operations were performed by a single surgeon. We collected and analyzed the perioperative data, clinical outcomes, and demographic characteristics, including age, gender, body mass index, tumor size, tumor location, degree of malignancy, disease stage, incision length, length of bowel resection, lymph node harvest, resection margin, estimated blood loss, use of curved instrument, duration of operation, drain placement, pain score, duration of hospital stay, bowel return, use of extra ports, and creation of a diverting enterostomy.
Surgical equipment
All SILC procedures were performed with a self-made glove-port system. In brief, the system was constructed by connecting a commercial wound protector (ALEXIS® wound retractor system; Applied Medical, Rancho Santa Margarita, CA) to a surgical glove. Trocars (e.g., 5 mm, 10 mm, and 15 mm) were then introduced through the little finger, thumb, and middle finger of the glove, respectively (Fig. 1).
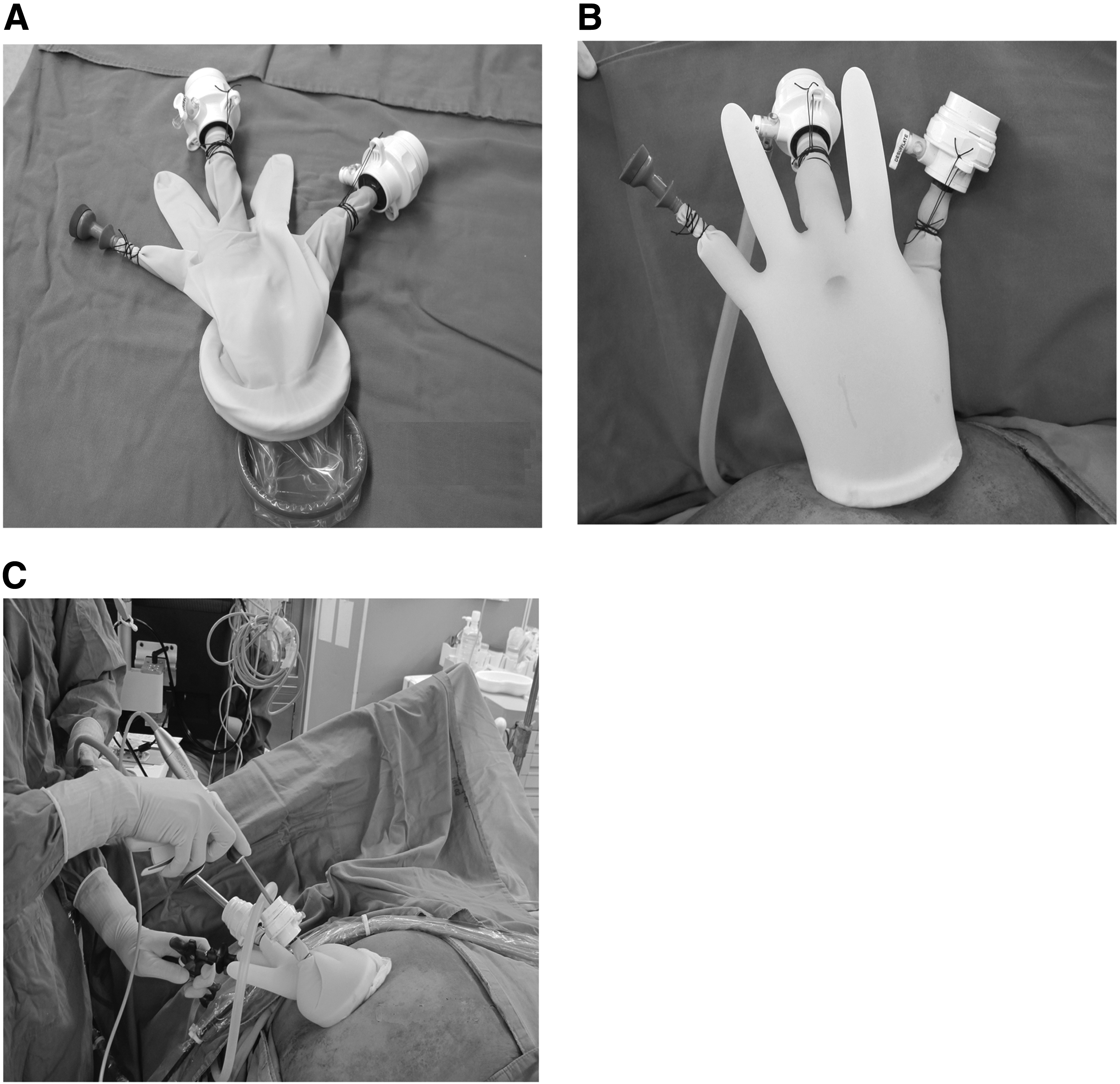
Illustration of the self-made single-port system.
Surgical procedures
Under general anesthesia, patients were placed in the lithotomy position. An incision 2.5–3 cm long was made at the umbilicus or McBurney's point. The incision was decided by the surgeon according to the tumor location, anatomic consideration, and surgical experience. Then, for SILC, the self-made glove-port system with the wound protector was placed, and a CO2 pneumoperitoneum was produced with a maximal pressure of 12 mm Hg. A laparoscope 30° in angle and 10 mm in diameter was used for all patients. A medial-to-lateral approach was used for all procedures. Conventional and curved laparoscopic instruments were used interchangeably. Dissection was primarily done with electrocautery and/or LigaSure™ instruments using the ForceTriad™ energy platform (Valleylab™, Covidien, Boulder, CO). The inferior mesenteric vessels were identified and ligated with hemoclips. In some cases, curved dissection instruments or scissors were used for lateral detachment of the sigmoid colon. After the left colon was freed, the mesorectum was dissected before dissection of the colorectum with an Echelon Flex 60 Endopath™ stapler (Johnson & Johnson, New Brunswick, NJ). The specimen was removed through the umbilical or McBurney's incision wound, and the anastomosis was made intracorporeally with a Proximate ILS intraluminal curved or straight stapler (Johnson & Johnson). Lymph node dissection was also performed in all cases. Representative images of specimen removal and postoperative wounds are shown in Figure 2.
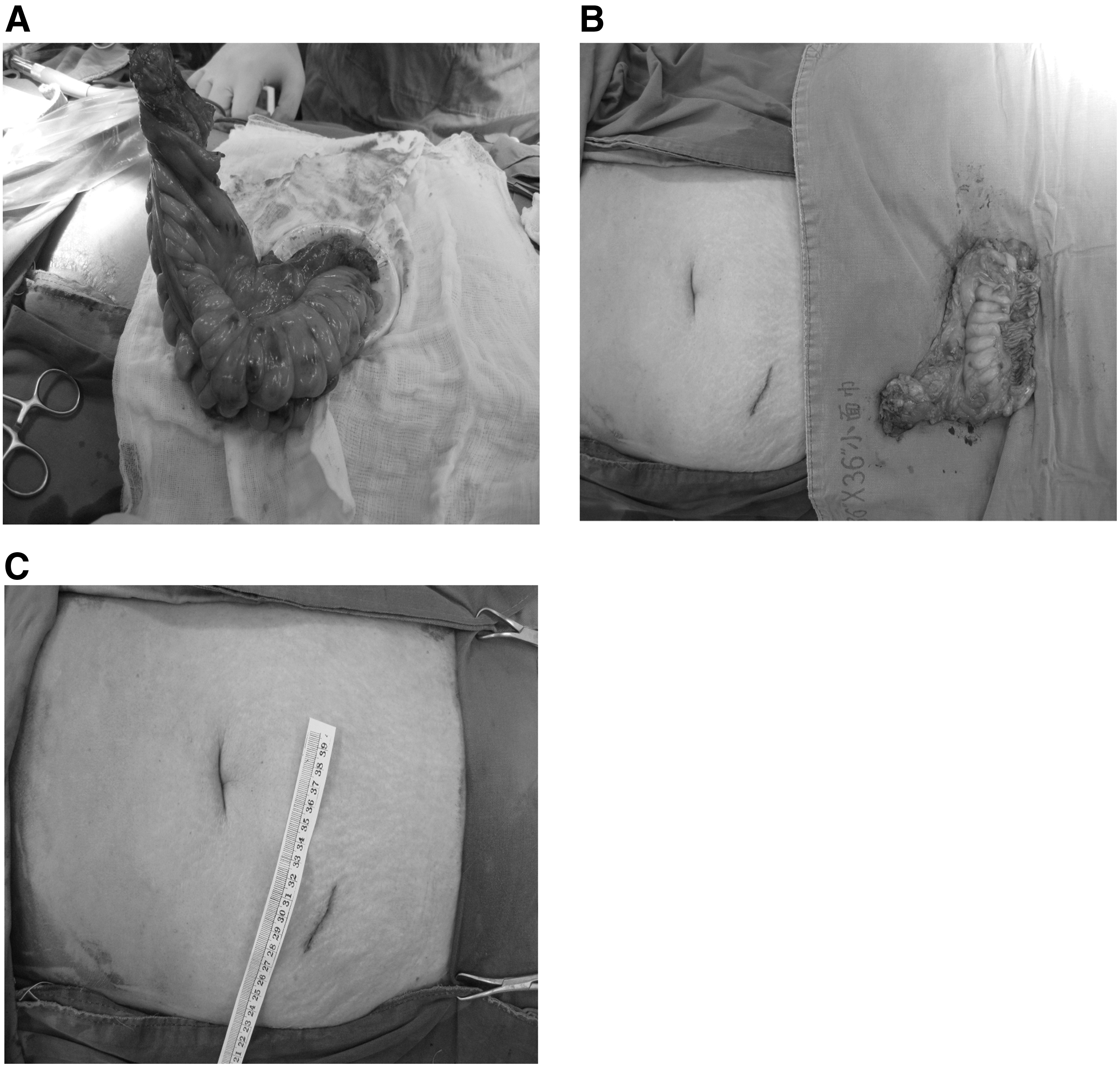
Representative images of specimen removal and postoperative wounds.
After the removal of the laparoscopic instruments and glove-port device, a Jackson–Pratt drain was placed through the incision wound if required, depending on the degree of dissection, blood loss, and presence of lymphatic or bloody discharge after completion of the procedure. On the other hand, a diverting enterostomy was created, if needed, over McBurney's point in the umbilical incision group and over the McBurney's incision wound in the McBurney's incision group, respectively.
Postoperative care
All patients received standard postoperative care and pain management. Pain severity was assessed 24 hours postoperatively using visual analog scale (VAS) pain scores. Patients were asked to rate their pain on a scale of 1 (no pain) to 10 (the worst pain imaginable). All patients were told of the availability of analgesia. Meperidine was administered as the postoperative analgesic upon patient request only. Patients weighing >50 kg received one injection of 50 mg of meperidine intramuscularly; for those weighing <50 kg, the dosage was adjusted by the patient's weight (1 mg/1 kg). Meperidine was administered intramuscularly once every 4 hours or as needed. No other form of pain relief was administered in the postoperative period. If drains were placed, they were removed when the drainage amount was <50 mL/day and the contents were clear. Patients were kept fasting until the bowel function returned, defined as passage of flatus, and then sips of water were allowed. If water was tolerated, the diet was advanced to clear liquids followed by a soft diet. When tolerating a general diet, patients were discharged typically on postoperative Day 5–7, and they were followed up in the outpatient clinic.
Statistical analysis
Patients' demographic, perioperative data, and clinical outcomes were summarized as mean±standard deviation values for continuous data and n (%) for categorical data for the McBurney's and umbilical incision groups. Differences between groups were compared by using two-sample t test for continuous variables and Pearson's chi-squared test or Fisher's exact test if any cell number was less than 5 for categorical variables.
All statistical assessments were two-tailed and considered significant at P<.05. Statistical analyses were performed by using SPSS version 15.0 statistics software (SPSS Inc., Chicago, IL).
Results
In this study, we examined whether the site of the single incision of SILC affects the outcomes of patients. Therefore, all the patients' data, including demographic and clinical characteristics, for the umbilical and McBurney's SILC groups are listed in Table 1. In total, 61 patients were enrolled in this retrospective study, including 48 patients (25 males, 52.1%; 23 females, 47.9%) in the umbilical SILC group and 13 patients (9 males, 69.2%; 4 females, 30.8%) in McBurney's SILC group. Patients' mean age was 63.2±13.8 years and 63.4±9.5 years for the umbilical SILC and McBurney's SILC groups, respectively. There were no significant differences in age, gender, body mass index, tumor size, degree of malignancy, and disease stage between these two groups. However, we found that the tumor location was significantly different between these two groups (P=.015): the percentage of tumor location below the peritoneal reflection was much higher in the McBurney's SILC group (38.5%) than in the umbilical SILC group (10.4%).
Data are mean±standard deviation values or number (%) as indicated.
Statistically significant difference.
BMI, body mass index; SILC, single-incision laparoscopic colectomy.
Surgical data and clinical outcomes between these two groups were further analyzed and are shown in Table 2. All operations were performed successfully because no intraoperative complication occurred and no patient needed conversion to laparotomy. Median incision length was 3.5 cm and 4.9 cm in the umbilical and McBurney's SILC groups, respectively. Median duration of operation was 176.0 minutes and 180.8 minutes in the umbilical and McBurney's SILC groups, respectively. Although the above data revealed some differences, there was no statistically significance difference between the two groups with respect to the incision length and duration of operation. Similarly, there was no significant difference in length of bowel resection, lymph node harvest, resection margin, blood loss, use of curved instrument, drain placement, and return of bowel function between these two groups. Nonetheless, we observed an interesting phenomenon that patients in the umbilical SILC group had a significantly higher frequency of meperidine demand for the alleviation of wound pain than those in the McBurney's SILC group (0.4±0.7 versus 1.4±1.8, respectively; P=.002), despite the lack of statistical significance in pain score between the two groups.
Data are mean±standard deviation values or number (%) as indicated.
Indicates statistically significant difference.
Also, 2 of the 48 patients (4.2%) in the umbilical SILC group and 1 of the 13 patients (7.7%) in the McBurney's SILC group received an extra port (5 mm) over the left lower quadrant of the abdomen in addition to the single incision wound because of difficult anatomy. Owing to the multiple underlying diseases, a diverting enterostomy was created in 5 patients (10.4%) in the umbilical SILC group and 3 patients (23.1%) in the McBurney's SILC group. Finally, no mortality or complication occurred in either group during the postoperative hospital stay. Moreover, no significant difference in the length of hospital stay was observed between the two groups.
Discussion
To achieve better performance of SILC, a glove-port system constructed by connecting a commercial wound protector to a surgical glove has been developed and used.18,22 The double-ring design of the wound protector allows not only the wound protector and surgical glove to be connected tightly, but also the glove to roll completely around the wound protector without air leakage. The device allows a larger range of movement, better wound protection, and more feasibility of direction change at any time. Furthermore, it is suitable for all body types and different incision sites to enter the abdominal cavity. Thus, the glove-port system also provides the feasibility of SILC by McBurney's incision.
Several studies have revealed that SILC could reduce postoperative wound pain and decrease the use of analgesics compared with multiport or hand-assisted laparoscopy.23–25 However, our previous study showed that the postoperative VAS pain scores were higher in the umbilical SILC group than in the conventional laparoscopic colectomy group. 18 Based on the potential clinical benefits of postoperative pain control, we investigated the use of postoperative single-dose local anesthesia wound infiltration after umbilical SILC. An association between lower pain scores and administration of local anesthesia after SILC procedures was shown, but the difference was not statistically significant.
In the last two centuries, open appendectomy is the most common approach to treat appendicitis when time and cost are taken into consideration. Most surgeons are familiar with the procedure of McBurney's incision, which makes the McBurney's SILC an alternative choice for performing SILC. Although there were comparable surgical outcomes between the umbilical and McBurney's SILCs in this study, several technical issues have to be considered in choosing which incision site to be made for SILC. For McBurney's SILC, the splenic flexure take-down is hard to manipulate as the incision wound is much more distant than that of the umbilical SILC. Moreover, patients with a redundant sigmoid colon have the advantage for the performance of the McBurney's SILC because splenic flexure may not need to be taken down. Based on this observation, it is highly recommended that a lower gastrointestinal series examination be done before the McBurney's SILC to examine the redundancy of sigmoid colon. For those tumors located below the peritoneal reflection, a limited angle for traction and dissection in the umbilical SILC is encountered because the axis is parallel between the umbilicus and the rectum. In this situation, McBurney's SILC may be a better choice than the umbilical SILC to provide the feasibility of lateral dissection for the tumors below the peritoneal reflection. Hence, 38.5% and 10.4% of the tumors were located below the peritoneal reflection in the McBurney's and the umbilical incision groups, respectively. It is notable that the tumor location was significantly different between these two groups (P=.015). We also found that small bowel interference during the operation is a potential problem in McBurney's SILC. Patients were put in the right Trendelenburg position to keep the small bowel free from the surgical field. Because the incision wound in McBurney's SILC is laterally to the umbilical SILC, the operated angle of the laparoscope is limited in McBurney's SILC, leading to frequent small bowel interference. Therefore, meticulous and careful dissection is needed while performing McBurney's SILC. On the other hand, when it is planned to create a diverting enterostomy, patients receiving the umbilical SILC need an additional incision wound for enterosotmy. However, McBurney's SILC provides the same incision site for a diverting enterostomy so as to avoid an additional incision wound. Collectively, the selection of incision site for SILC still depends on the surgeon's experience and considerations with respect to the tumor location and anatomy.
Although poorly controlled postoperative pain may increase morbidity and mortality, both clinical outcomes and patient satisfaction improve when postoperative analgesia is optimized. 26 Opioid drugs administered for postoperative wound pain may result in problematic side effects such as nausea, vomiting, oversedation, confusion, and delay of postoperative resumption of bowel function. 27 In this study, there was no statistical significance for the difference in VAS pain score between the umbilical and McBurney's SILC groups. However, patients in the umbilical SILC group had a significantly higher frequency of meperidine demand compared with those in the McBurney's SILC group (0.4±0.7 versus 1.4±1.8, respectively; P=.002). The result suggests that patients in the McBurney's SILC group have less opiate demand and better postoperative wound pain control compared with those in the umbilical SILC group. In this way, it may reduce the side effects caused by opioid drugs. Furthermore, there are some limitations in this study, and they should be taken into consideration in further studies. First, the sample size is too small, and the study is just a retrospective study. However, all procedures were performed by the same surgeon, and the patients in these two groups were comparable. Second, we did not assess the cosmetic outcome of the postoperative wound. Therefore, a longer follow-up may have to be planned, and then the cosmetic outcomes will be evaluated at that time.
In conclusion, this study further strengthens the safety and feasibility of SILC in treating colorectal diseases. Although SILC via an umbilical or McBurney's incision brings comparable surgical outcome as observed in this study, McBurney's SILC in particular alleviates the patient response to the postoperative wound pain. In addition to this promising advantage, McBurney's SILC provides the same site for a diverting enterostomy to avoid an additional wound. Therefore, McBurney's SILC seems to be an alternative approach for treatment of colorectal diseases.
Footnotes
Disclosure Statement
No competing financial interests exist.