
Abstract
Abstract
Background:
To present our initial experience with laparoscopic salpingotomy using the Floseal™ (Baxter International Corp., Deerfield, IL) hemostatic matrix for tubal pregnancy and to evaluate the efficacy and tubal patency after salpingotomy.
Materials and Methods:
A prospective study was conducted on 20 consecutive patients with tubal pregnancy undergoing laparoscopic salpingotomy using the Floseal hemostatic matrix. The outcome measures were treatment success rates and homolateral patency rates.
Results:
Of 20 cases, 19 cases (95%) were successfully performed without any additional intervention, and 1 case was switched to salpingectomy during the initial surgery. During the mean β-human chorionic gonadotropin resolution time of 17.9±6.4 days, postoperative complications or persistent trophoblasts did not occur. Of 19 salpingotomy patients, only 12 patients received a tubal patency test using hysterosalpingography, and the homolateral tubal patency rate was 75% (9 of 12).
Conclusions:
The use of Floseal allows laparoscopic salpingotomy to be performed successfully and easily with comparable outcomes.
Introduction
E
However, a particularly challenging problem in performing laparoscopic salpingotomy is control of bleeding at the implantation site after removing the product of conception from the Fallopian tube. Although bleeding points can be coagulated with microbipolar cautery, excessive coagulation may result, damaging the healthy tube. Therefore, novel methods for the control of bleeding in laparoscopic salpingotomy are needed.
Floseal (Baxter Healthcare Corp., Deerfield, IL, USA) is a hemostatic sealant composed of a gelatin-based matrix and thrombin solution. Upon coming into contact with blood after its application at a bleeding site, the gelatin particles swell and cause tamponade. The bulk of the gelatin matrix–thrombin composite has the effect of slowing blood flow and providing exposure to a high thrombin concentration, thus hastening clot formation. It is biocompatible and typically resorbed within 6–8 weeks. Therefore, this method may be particularly suitable for use in postsalpingotomy tubal bleeding, where there is a superficially pervasive focus of bleeding. The aim of this study was to present our initial experience with laparoscopic salpingotomy using the Floseal hemostatic matrix for tubal pregnancy and to evaluate both its efficacy and tubal patency after salpingotomy.
Materials and Methods
Study patients
After the approval of the Institutional Review Board, this study was conducted prospectively between February 2012 and December 2013 at the Department of Obstetrics and Gynecology of the CHA Gangnam Medical Center, Seoul, Republic of Korea. Patients who were diagnosed with a tubal ectopic pregnancy and elected laparoscopic surgical treatment were approached for study enrollment. A diagnosis of tubal pregnancy was performed using a nonlaparoscopic approach with clinical, physical, and vaginal ultrasound examinations, β-human chorionic gonadotropin (β-hCG) levels, or uterine curettage. 5 Preoperative informed consent was obtained from all patients after explanations of possible risks and complications for salpingotomy were given, such as persistent trophoblasts and repeated ectopic pregnancy in the operated tube.
The inclusion criteria were the following: (1) age of at least 18 years with visible tubal pregnancy on transvaginal sonography; (2) appropriate medical status for laparoscopic surgery (American Society of Anesthesiologists physical status classification 1 or 2); and (3) agreement to surgical treatment and follow-up. The exclusion criteria were the following: (1) patients with no desire for future pregnancy; (2) patients with interstitial or heterotopic pregnancy; (3) patients pregnant after in vitro fertilization; (4) patients with a pregnancy in a solitary tube; and (5) patients with a contralateral tubal occlusion or hydrosalpinx, as documented earlier at hysterosalpingography or laparoscopy or as found during surgery for the index ectopic pregnancy.
Surgical procedures
All surgical procedures were performed by a single surgeon (T.S.). The patients were placed in a deep Trendelenburg lithotomy position under general endotracheal anesthesia. A 12-mm trocar was inserted into the umbilical region, followed by three 5-mm trocars in both the lower quadrant and suprapubic area. Subsequently, the abdominal cavity was carefully examined, and a suction device was used to evacuate the hemoperitoneum, if present. After the involved tube was immobilized with an atraumatic grasper, a dilute solution of vasopressin (Hanlim Pharm, Seoul) (2.5 U of vasopressin in 10 mL of saline solution) was injected through a 22-gauge spinal needle into the mesosalpinx around the affected tube to reduce blood loss (Fig. 1). A linear incision, allowing removal of the ectopic mass in its entirety, was made using a fine-tip needle cautery in the superior aspect of the Fallopian tube just above the largest diameter of the tube, correlating with the location of the ectopic pregnancy. The ectopic mass was then removed by combining hydrodissection and traction using atraumatic forceps; aspiration and compression lateral to the incision site were used to facilitate removal of the products of conception, if necessary. In cases of ruptured tubal pregnancy, the product of conception was evacuated from the ruptured site without a separate incision. After the entirety of the pregnancy was removed, the placental bed was carefully evaluated. If any bleeding or oozing of blood from inside the lumen or tubal wall occurred, sites of bleeding were covered with Floseal under direct vision with a laparoscopic applicator, followed by a 2-minute wait for the Floseal to act. Bleeding sites were then reexamined by irrigation. Once hemostasis was achieved, the tube was closed in a single layer by two or three interrupted stitches using 6-0 (polydioxanone) monofilament synthetic absorbable suture (PDS®) II (Ethicon, Somerville, NJ). If Floseal was ineffective in bleeding control, excessive coagulation using microbipolar cautery was required; thus, resultant tubal damage occurred, and the procedure was altered to salpingectomy. The surgical specimens were then removed using a laparoscopic bag (LapBag; Sejong Medical, Pajoo, Korea). Subsequently, the contralateral Fallopian tube was closely inspected to exclude the possibility of unexpected tubal lesions (i.e., hydrosalpinx, severe peritubal adhesions, malformations, or other pathologies) and copiously irrigated with 3000–4000 mL of normal saline if a hemoperitoneum was present. If patients had not received methotrexate therapy within 1 week, all patients received a 50 mg/m2 intramuscular injection of methotrexate postoperatively to prevent the development of persistent trophoblast.6–8
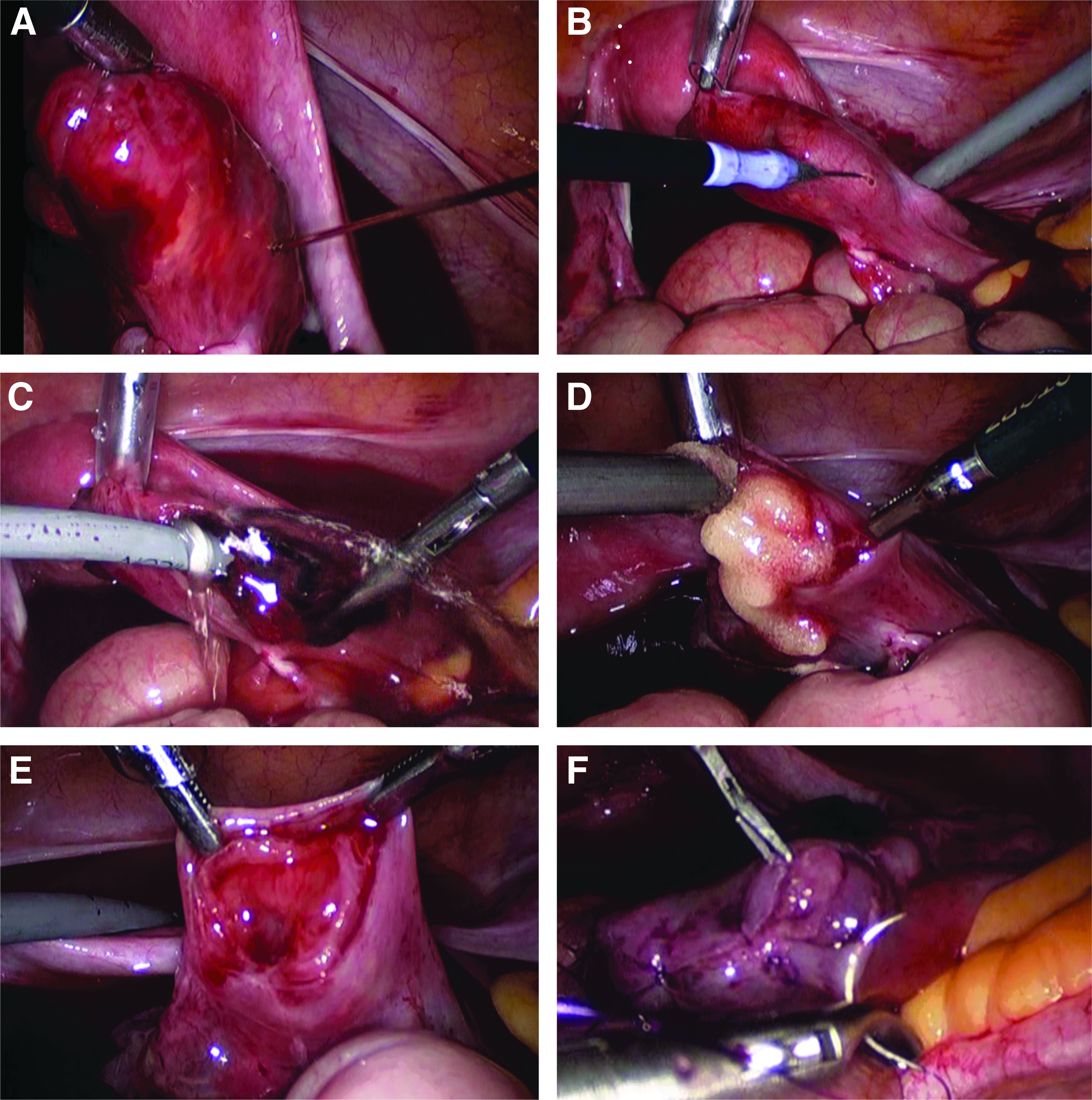
Surgical photographs.
The patients were discharged on postoperative Day 2 or 3, and their serum β-hCG levels were monitored on a weekly basis until levels were <5 mIU/mL to identify persistent trophoblasts. Patients were diagnosed as having persistent trophoblasts when the postoperative serum β-hCG concentration increased again or did not decrease for at least 1 week. 9 To assess affected tubal patency after surgery, the patients were offered a hysterosalpingogram at 3 months after achieving a β-hCG level of <5 mIU/mL. Tubal patency tests were assessed by a gynecologic radiologist unaware of the patient's treatment.
Outcome measures
The primary outcome measure was the treatment success, which was defined as the completion of the initially planned surgical treatment (laparoscopic salpingotomy) without the need for any surgical intervention (e.g., salpingectomy). Secondary outcome measures included (1) tubal patency test, (2) persistent trophoblasts, and (3) postoperative complication of salpingotomy. The β-hCG resolution time was defined as the period from the date that a serum β-hCG level of <5 mIU/mL was achieved.
SPSS version 13.0 software (SPSS, Inc., Chicago, IL) was used for the statistical analysis. Data were presented as the frequency (percentage) for qualitative variables and the mean±standard deviation value or median (range) for quantitative variables after the normal distribution of the data was assessed.
Results
Twenty consecutive patients with tubal pregnancies were included in this prospective cohort study. The baseline characteristics for all patients are given in Table 1. The mean age of the patients at the time of surgery was 30.3±4.3 years (range, 21–35 years). All patients but 1 were nulliparous. Two patients (10%) had a history of an ectopic pregnancy, which had been managed with systemic methotrexate treatment. The median levels of preoperative serum β-hCG and mean duration of gestation were 3760 mIU/mL (range, 816–61,700 mIU/mL) and 51.1±8.7 days (range, 38–64 days), respectively. Yolk sac, fetal echo, and embryonic cardiac motion on the preoperative transvaginal sonography were noted in 7 (35%), 5 (25%), and 4 patients (20%), respectively. Main indications of surgery were positive embryonic cardiac motion in 4 patients (20%), serum β-hCG level >15,000 mIU/mL in 2 patients (10%), suspicion of massive hemoperitoneum in 6 patients (30%), failure with systemic methotrexate treatment in 7 patients (35%), and refusal of medical therapy in 1 patient (5%). There were ruptured ectopic pregnancies in 2 cases (10%) and unruptured ones in 18 cases (90%). Of the 18 cases with unruptured tubal pregnancy, 12 cases involved a leaking tubal pregnancy: the Fallopian tube involving the ectopic pregnancy had an intact tubal surface, but active bleeding from the fimbrial end of the tube was noted.
Data are mean±standard deviation values (range), median (range), or n (%) as indicated.
Massive hemoperitoneum was noted on transvaginal sonography, and we could not preoperatively exclude tubal rupture with active bleeding.
Duration of gestation was calculated as the period from the date of last menstrual period to the date of surgery.
Leaking tubal pregnancy was noted in 12 cases; the Fallopian tube involving the ectopic pregnancy had an intact tubal surface, but active bleeding from the fimbrial end of the tube was present.
β-hCG, β-human chorionic gonadotropin.
At initial surgery, 19 cases (95%) were completed by intended laparoscopic salpingotomy, but 1 case (5%) was switched to laparoscopic salpingectomy (Table 2); despite the application of Floseal at the bleeding site of the tube, hemostasis was not completely achieved, and additional bipolar coagulation was extensively required. Thus, the affected tube was damaged, and resultant salpingectomy was performed. During the mean β-hCG resolution time of 17.9±6.4 days, postoperative complications or persistent trophoblasts did not occur. Therefore, the rate of treatment success was 95% (19 of 20). Of 19 salpingotomy patients, only 12 patients received a tubal patency test using hysterosalpingography at 3 months after achieving a serum β-hCG level of <5 mIU/mL. The homolateral tubal patency rate was 75% (9 of 12), whereas the contralateral patency rate was 83% (10 of 12).
Data are number (%) or mean±standard deviation values as indicated.
Despite the application of Floseal at the bleeding site of the tube, hemostasis was not achieved, and excessive bipolar coagulation was required. Thus, the affected tube was damaged, and resultant salpingectomy was performed.
Defined as the difference between preoperative hemoglobin level and that at postoperative Day 1.
Calculated as the period from the date of the surgery to the date achieving serum β-human chorionic gonadotropin (β-hCG) of <5 mIU/mL.
A tubal patency test using hysterosalpingography was performed in only 12 patients at 3 months after achieving a serum β-hCG level of <5 mIU/mL.
Discussion
The main finding of this study was that the use of Floseal allowed laparoscopic salpingotomy to be performed successfully and easily. The treatment success rates and homolateral tubal patency rates were 95% and 75%, respectively. To the best of our knowledge, this study is the first to evaluate the efficacy of Floseal hemostasis in laparoscopic salpingotomy for tubal pregnancy.
After the products of conception are removed from the Fallopian tube, bleeding control at the implantation site is of paramount importance. If bleeding persists despite the surgeon's earnest efforts, tube-sparing surgery such as salpingotomy or salpingostomy should be abandoned and switched to salpingectomy. To achieve hemostasis, direct compression of the bleeding bed, microbipolar cautery at the bleeding point, suture ligature of the mesosalpinx, and segmental tubal resection with reanastomosis have been used. In most cases, direct compression alone is insufficient. Microbipolar cautery can be used to desiccate a bleeding placental bed; however, damage to the myosalpinx may be irreversible. Suture ligature in the mesosalpinx is an effective hemostasis method but can potentially harm the surrounding tubal vasculature. Segmental tubal resection with reanastomosis is a time-consuming process requiring special expertise and extensive microsurgical experience. Our hemostatic method using Floseal, by comparison, is a simple and powerful method that avoids potential tubal injury. In this study, we provide new evidence that Floseal hemostasis in laparoscopic salpingotomy is a promising strategy to control tubal implantation-site bleeding and preserve tubal integrity.
The treatment success rate (95%) observed in this study was higher than those of other studies. Fujishita et al. 10 treated 97 cases of tubal pregnancy using laparoscopic salpingotomy: 75 (77%) were successfully treated by salpingotomy, and 22 (23%) were switched to salpingectomy; thus, their treatment success rate was 77%. Laparoscopic salpingostomy performed by Hajenius et al. 11 also showed a 72% treatment success rate. We believe that our high success rate was the result of the use of Floseal hemostasis, but additional studies are required to confirm this conclusion. In terms of homolateral patency rate after salpingo(s)tomy, our finding (75%) was comparable to those (66–94%) of previous studies.10,11
In this series, we encountered no persistent trophoblasts after salpingotomy. Such a condition is often considered attributable to methotrexate prophylaxis. Generally, a persistent trophoblast after conservative tubal surgery (either salpingotomy or salpingostomy) could arise in 4%–20% of patients.5,12 The rate of persistent trophoblast was reduced in one study 8 from 14% to 2% with the use of prophylactic methotrexate. A recent meta-analysis of ectopic pregnancy also showed that a single prophylactic shot of methotrexate, given intramuscularly immediately postoperatively, significantly reduced the occurrence of persistent trophoblasts after laparoscopic salpingostomy (relative risk, 0.89; 95% confidence interval, 0.82–0.98). 2 We believe that the prophylactic use of methotrexate after salpingotomy increases a woman's chance to preserve the affected tube by reducing the risk of tubal damage or salpingectomy resulting from a persistent trophoblast.
When we began performing tubal conservative surgery using Floseal hemostasis for the treatment of tubal pregnancy, we routinely closed the linear incisional wound of the affected tube, because of the worry about tubal fistula and the familiarity with laparoscopic suturing and tying. However, whether to treat an ectopic pregnancy with a salpingotomy (suturing) or salpingostomy (no suturing) is strongly debated, and multiple studies have investigated this issue. Pouly et al. 13 reported experience with laparoscopic salpingotomy for 321 tubal pregnancies. Second-look laparoscopy was performed in 18 patients to assess tubal healing, and all salpingotomy sites were covered by serosa. Lundorff et al. 14 reported 102 patients with tubal pregnancy who underwent second-look laparoscopy 6–10 weeks after initial salpingostomy. The authors reported failures of tubal closure after salpingostomy, with leakage in 5 cases. When such fistulas are present, repeated tubal pregnancy may occur at the fistula site, or it may increase the risk of defective ovum transport or a complication of abdominal pregnancy. However, the results of a study by Fujishita et al., 10 who compared laparoscopic salpingotomy with and without suturing for tubal pregnancy, were that the procedure that involved suturing had no additional benefit over the nonsuturing technique during salpingotomy. Additional large, randomized controlled trials are needed in order to resolve this issue.
In this series, there were many severe tubal pregnancies, such as a suspected ruptured tubal ectopic pregnancy, an ectopic mass >4.0 cm, the presence of embryonic cardiac motion, preoperative β-hCG levels >15,000 mIU/mL, or failures of medical treatment. The reason was our treatment protocol. According to our institutional policy for ectopic pregnancy, medical treatment with systemic methotrexate was the first-line treatment for all patients with tubal pregnancy who were hemodynamically stable with no evidence of rupture. If patients had any contraindication to methotrexate that was consistent with the 2008 American College of Obstetricians and Gynecologists practice bulletin, 15 we recommended surgery as a second-line treatment (laparoscopic salpingectomy in patients with no desire for future pregnancy and laparoscopic salpingotomy in patients with a desire for future pregnancy).
The limitations of this study include the followings. First, this study had a noncomparative design, a relatively small number of patients, and a relatively short follow-up period. Second, surgical procedures were performed by a single surgeon; thus, our results may not be applicable to other surgeons. Third, there was lack of fertility outcome. These factors may weaken our results.
In conclusion, this study indicates that the use of Floseal allows laparoscopic salpingotomy to be performed successfully and easily. However, to draw firm conclusions, more data are required, and a multicenter trial should be done to compare the current technique with conventional techniques.
Footnotes
Disclosure Statement
No competing financial interests exist.