
Abstract
Abstract
Background:
Single-incision laparoscopic surgery (SILS) developed rapidly in recent years. This report describes our initial experience on SILS combined cholecystectomy and appendectomy (SILSC&A) with a unique method of umbilical reconstruction. In addition, a retrospective comparison with conventional combined laparoscopic cholecystectomy and appendectomy (LC&A) was analyzed.
Materials and Methods:
Between April 2009 and December 2013, 62 patients with benign gallbladder and appendix disease underwent laparoscopic combined cholecystectomy and appendectomy at our institution. Of these, 34 (54.8%) underwent SILSC&A (Group 1), and 28 (45.2%) underwent LC&A (Group 2). Demographic, intraoperative, and postoperative data were analyzed retrospectively and compared between the two groups.
Results:
No significant differences were identified in the preoperative patient characteristics between the two groups. SILSC&A was associated with a shorter operative time (62.2±19.7 versus 77.5±21.4 minutes, respectively; P=.005) and better cosmetic results (4.6±0.7 versus 4.1±0.6, respectively; P=.004). There were no significant differences between the two groups with respect to other postoperative variables.
Conclusions:
The present study suggests that SILSC&A is as safe and efficacious as conventional LC&A in experienced hands. A uniform method of umbilical reconstruction is helpful in improving cosmesis and decreasing hernia rate. Long-term follow-up and further prospective randomized trials are anticipated.
Introduction
S
However, for SILS combined surgeries, the experience was rather limited. The main purpose of these studies is usually that of introducing new techniques.5–7 To date, no comparative studies concerning the outcomes of SILS combined cholecystectomy and appendectomy (SILSC&A) versus conventional combined laparoscopic cholecystectomy and appendectomy (LC&A) have been reported in the literature. Umbilical reconstruction is important for SILS, but this aspect of the procedure is seldom discussed in the literature.
In the current study, we present our experience on SILSC&A. The procedure details with our unique method of umbilical reconstruction were described. A retrospective comparison between SILSC&A and LC&A was analyzed.
Materials and Methods
Patients
Between April 2009 and December 2013, 62 patients with benign gallbladder and appendix disease underwent laparoscopic combined cholecystectomy and appendectomy in the Department of General Surgery of Shengjing Hospital, Shenyang, China. All the patients had a history of chronic appendicitis and chronic calculus cholecystitis or a gallbladder polyp larger than 1 cm. The acute onset of either appendicitis or cholecystitis forced the patients to come to our hospital for operation. When informed that cholecystectomy and appendectomy could be performed at the same time, they were pleased to receive a combined surgery. Of these patients, 34 (54.8%) underwent SILSC&A (Group 1), and 28 (45.2%) underwent LC&A (Group 2). All the diagnoses were confirmed by preoperative computed tomography scan or ultrasonic examination and postoperative pathologic examination.
Age, gender ratio, operation time, blood loss, conversion rate, postoperative visual analog pain scale (VAS) scores, cosmetic scores, first flatus time, and postoperative hospital stay were compared between the two groups. The subjective pain was evaluated on postoperative Day 1 by a 10-cm VAS score, which ranged from 0 (no pain) to 10 (extremely severe pain). Rescue analgesics (20 mg of parecoxib sodium, intravenous) were given at the request of the patient or if the VAS scored moderate or more intense. All the patients had a follow-up visit at 3 months after discharge and were asked to rate their overall satisfaction with the appearance of their scars using a 5-point scoring system. 2 An informed consent form was obtained from all the patients, and the study was approved by the Institutional Review Board of our hospital.
Surgical procedure
SILSC&A surgical technique
The surgical team set-up, incision design, and trocar placement were the same as previously described (Fig. 1b). 5 The patient was first positioned in a reverse Trendelenburg position with a 15° left tilt. We began our procedure with cholecystectomy in a retrograde fashion. The gallbladder was dissected to the cystic duct, which was then ligated using two clips. It was then amputated using a Harmonic® scalpel (Ethicon Endo-Surgery, Cincinnati, OH) and placed in the right hepatorenal recess before removing. The patient was then repositioned in the Trendelenburg position with a further left tilt to 25°. The appendix was located, and the cecum was adequately mobilized. The mesoappendix was dissected using a Harmonic scalpel to the base of the appendix. Thereafter the appendix was ligated using clips (if the appendix measured less than 10 mm in diameter) or a silk ligature in the case of an enlarged appendix. The appendix was then amputated, and the specimens of both gallbladder and appendix were put into a specimen bag. The opening of the 10-mm trocar was extended to form a vertical incision about 15 mm in length. Both specimens were delivered out of the body in a specimen bag via umbilical incision.
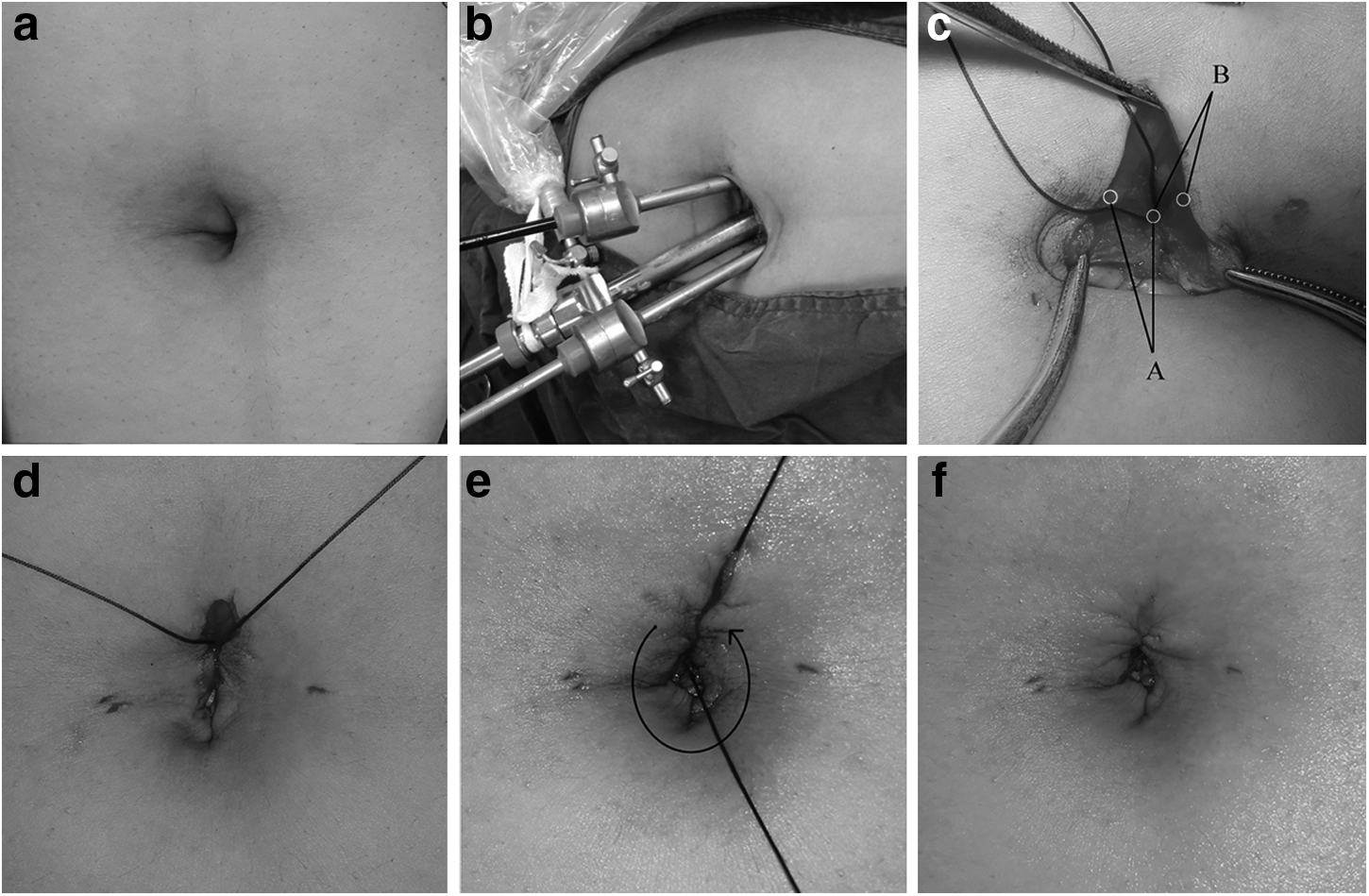
The transumbilical incision was closed in two layers with “0” absorbable suture (CL-884, Polysorb™; Covidien, Inc., Mansfield, MA). The umbilical fascia with the peritoneum was closed by use of a running suture. The knot was left in the middle of the entire incision, which was just beneath the superior margin of the umbilical ring (Fig. 1c). Next, two anchor sutures were placed separately to fix the skin of the superior umbilical margin on the umbilical fascia, and the incision was thus separated into two halves (Fig. 1d). Three or four running subcuticular sutures were done to close the caudal half of the incision. The oval umbilical ring was thus rebuilt, and the umbilical fossa with sufficient depth was reconstructed (Fig. 1e). For the other half of the incision, subcutaneous fat tissue was closed in the caudal-to-cranial direction, and the skin was closed in the cranial-to-caudal direction by running a subcuticular suture. Thus the entire transumbilical incision can be perfectly concealed within the umbilical fossa (Fig. 1f). No abdominal drainage was placed after the procedure.
LC&A surgical technique
A 10-mm umbilical incision, a 10-mm incision below the xiphoid process, a 5-mm incision in the suprapubic area, and a 5-mm incision in the right abdomen were made in the LC&A procedure. The surgical technique was the same as conventional laparoscopic cholecystectomy and laparoscopic appendectomy. Both specimens were delivered out of the body via the enlarged subxiphoid incision.
Statistical analysis
The results of patients who underwent SILSC&A and LC&A were compared. Continuous data are presented as mean±standard deviation values, median values, and the range. Categorical variables are expressed as numbers and percentages for the group from which they were derived. The t test and the Mann–Whitney U test were used for the comparison of continuous variables, and the chi-squared test was used for categorical variables. Results were considered statistically significant for P<.05.
Results
No significant differences were identified in the preoperative patient characteristics between the two groups. No case was converted to multi-incision laparoscopic surgery or open surgery in the SILSC&A group. Two cases were switched to open appendectomy after successful laparoscopic cholecystectomy because of severe adhesions around the appendix. SILSC&A was associated with a shorter operative time (62.2±19.7 versus 77.5±21.4 minutes, respectively; P=.005) and better cosmetic results (4.6±0.7 versus 4.1±0.6, respectively; P=.004). Although the postoperative VAS pain score was lower (2.4±0.9 versus 2.9±1.1, respectively; P=.066) in Group 1 than in Group 2, this did not reach statistical significance. There were no significant differences between the two groups with respect to other postoperative variables. No significant postoperative complications occurred in either group (Table 1).
BMI, body mass index; LC&A, conventional combined laparoscopic cholecystectomy and appendectomy; SILSC&A, single-incision laparoscopic surgery combined cholecystectomy and appendectomy; VAS, visual analog scale.
Discussion
During the last several years, one of the most significant advances in the field of laparoscopic surgery is the continued evolution of minimally invasive technologies, among which SILS is the most important part. Although specific benefits may vary according to the precise nature of the procedure, SILS is widely recognized as an improvement over conventional laparoscopic surgery, with some additional benefits such as reduced postoperative pain and superior cosmesis.8–11 Although single-incision laparoscopic cholecystectomy or appendectomy has been accepted as an effective technique,12–14 documentation about applying SILS in combined cholecystectomy and appendectomy remains rare. What is more, most of these studies are case reports or small case series for the purpose of introducing a new practice. No comparison with conventional laparoscopic procedures has been made in the literature to the best of our knowledge.
This study contributes to the literature on SILS as the first retrospective comparative trial to describe specific outcomes for patients who underwent SILSC&A. The most important finding of the present study was a better cosmetic result in the SILSC&A group compared with the conventional LC&A group. In the present study, no differences in blood loss, first flatus time, and hospital stay were observed between the two groups. The SILSC&A group had a lower postoperative VAS pain score than the LC&A group (2.4±0.9 versus 2.9±1.1, respectively; P=.066) in this study, but the difference failed to achieve statistical significance. The operation time was significantly shorter in Group 1 than in Group 2, which was rather beyond our expection.
It is generally accepted that SILS is technically more challenging than conventional laparoscopic procedures, which is usually translated into a longer operation time. The shorter operation time in the SILSC&A group is difficult to interpret and may reflect different operative speeds among individual surgeons. The operating time for SILSC&A was made faster by the fact that the surgeons had extensive experience with performing challenging SILS procedures, especially laparoscopic surgery of the biliary system, and adapted to performing SILSC&A quickly. Moreover, this study enrolled a small number of patients, and difficult cases were preferentially selected for LC&A during the early period of experience with SILSC&A in our institution. There were five technically difficult operations in the LC&A group in which operation time exceeded 100 minutes, whereas there were only two such operations in the SILSC&A group. A higher percentage of severely inflamed gallbladder or appendix in LC&A group could negatively affect the mean operative time.
However, the authors witnessed a clear trend toward reduction in operation time for SILSC&A with the accumulation of cases. Although SILSC&A is technically more challenging than LC&A, we cannot exclude the possibility that with increasing experience and training, the operation time of SILSC&A would decrease to that of LC&A levels.
The umbilicus is an important esthetic feature in the middle of the abdominal wall, and loss of this structure may represent a source of psychological distress. Umbilical reconstruction after SILS represents a challenging procedure for surgeons, especially when the umbilicus is deep and irregular in shape. However, approaches to incisional suture and cosmesis are technically immature compared with the rapid development in SILS applications. The problem with the incision suture in SILS seems too insignificant to be discussed, but it is of vital importance for the spirit of stealthy surgery. Various techniques, such as everting the umbilicus and making a “yin-yang” incision, have been described for peritoneal access and incision design during the procedure,15,16 pointing out the difficulty with this aspect of SILS. So herein we describe a simple method for umbilical reconstruction after transumbilical single-incision laparoscopic surgery that can produce a natural-looking umbilicus. Two anchor sutures are the key skills during umbilical reconstruction. Our method of incision suture allows the umbilicus to be reconstructed in a routine and cosmetic fashion.
Besides cosmesis, our method of umbilical reconstruction is also developed to cope with the problem of an incision hernia. SILS is suspected to increase the risk of umbilical hernia because a more sizable umbilical incision is required. A prospective randomized comparative study by Marks et al. 17 suggested that single-incision laparoscopic cholecystectomy is associated with improved cosmesis scoring at the cost of significantly higher hernia rates. However, some studies revealed that the hernia rate after SILS is acceptably low in the hands of experienced laparoscopic surgeons.18–20 It was revealed that factors associated with the wound complications included higher patient body mass index, longer skin incisions, multiport SILS, and a learning curve effect. The technique of umbilical reconstruction is related to the incidence rate of umbilical hernia. Differences exist in incision design and umbilical repair among laparoscopic surgeons, which are seldom discussed in the literature regarding SILS. We believe that a uniform method of incision design and suture can decrease the hernia rate and obviate a disfigurement of the umbilicus. The fact that we had no patients with umbilical hernia in this series supports our opinion.
This study has several limitations. First, the retrospective design may lead to an unintended selection bias of patients particularly suited for SILSC&A. Although not statistically significant, the acute onset of cholecystitis or appendicitis was more frequently seen in the LC&A group. The heterogeneity in the severity of disease between the two groups does not allow for an exact evaluation of surgical outcomes. Second, LC&A was performed earlier than SILSC&A at our institution, suggesting a difference in operating experience between SILSC&A and LC&A, thus inevitably increasing the risk of bias. A prospective randomized trial could more conclusively demonstrate any equivalences or superiority that may exist for the less invasive technique. Last, this study examined the results of experienced laparoscopic surgeons; the outcomes may not be representative of those obtained by the general surgeon population. Nevertheless, the study does demonstrate that the procedure can be safely performed by experienced laparoscopic surgeons.
In conclusion, the present study suggests that SILSC&A is as safe and feasible as LC&A for the treatment of concomitant benign gallbladder and appendix disease when performed by experienced laparoscopic surgeons. A uniform method of umbilical reconstruction is helpful in improving cosmesis and decreasing the hernia rate. Subsequent prospective randomized trials are in the planning stage at our institution to clarify the potential benefits of SILSC&A other than the cosmetic advantage.
Footnotes
Disclosure Statement
No competing financial interests exist.