
Abstract
Abstract
Background:
The laparoscopic approach would be difficult to perform without causing deformation of the stomach in managing gastrointestinal stromal tumors (GISTs) of the intraluminal type, especially in those that are located in the posterior gastric wall or around the gastroesophageal junction and the pylorus, because intraluminal GISTs usually require an excessive resection of the gastric wall for cure. We present a novel surgical technique for successful management of intraluminal gastric GISTs that minimizes deformation of the stomach regardless of tumor location.
Materials and Methods:
The operating surgeon handles the tumor by holding tissue surrounding the tumor and performs seromyotomy using an ultrasonically activated device along the outer edge of the tumor. The tumor gradually protrudes like an extraluminal tumor as the seromyotomy proceeds. When seromyotomy along the tumor comes up to the point where the tumor sufficiently turns over the gastric serosa, the tumor looks like a pedunculated extraluminal GIST. Two seromuscular sutures are applied to close the exfoliated seromuscular layer. The tips of two seromuscular sutures are held and then pulled up toward the ventral side so that the staple line is aligned in line with the minor axis of the stomach. Finally, complete tumor removal with minimal seromuscular resection is accomplished by applying a linear stapler.
Results:
All patients resumed oral ingestion on the day after surgery and showed no signs of anastomotic constriction or obstruction.
Conclusions:
Our laparoscopic procedure for gastric GISTs is simple and allows us easy and precise removal of the tumor and closure of the gastric wall with minimum necessary resection, regardless of the location and growth form of the tumors.
Introduction
G
Although several surgical procedures using traditional open surgery are available for gastric GISTs, laparoscopic approaches are limited. Recently, several laparoscopic approaches for gastric GISTs have been reported. The method varies significantly depending on location and growth form of the tumors (i.e., intraluminal or extraluminal). When a GIST shows an extraluminal growth, it is easy to perform a laparoscopic gastric wedge resection for the tumor by using linear staplers. 4 In contrast, the laparoscopic approach would be difficult to perform without causing deformation of the stomach in managing GISTs of an intraluminal type, especially those that are located in a posterior gastric wall or around the gastroesophageal junction and the pylorus, because intraluminal GISTs usually require an excessive resection of the gastric wall for a cure. Deformation of the stomach around the gastroesophageal junction and the pylorus may result in a troublesome problem after surgery. A fundusectomy or distal gastrectomy is a treatment of choice for such GISTs, but limited gastric resection is ideal for a localized small gastric GIST around these regions.
In this report, we present a novel surgical technique for successful management of intraluminal gastric GISTs that allows easy tumor resection and minimizes deformation of the stomach regardless of tumor location.
Materials and Methods
Operative indication
The safety of laparoscopic surgery for gastric GISTs smaller than 5 cm in size is now widely accepted.5–8 However, in gastric GISTs larger than 5 cm, laparoscopic surgery is, at present, not recommended because of the risk of pseudocapsule injury and subsequent intraabdominal spread of tumor cells. 9 In this study, the laparoscopic approach was thus indicated for gastric GISTs less than 5 cm in size.
An intraluminal and intramural gastric GIST, as well as an extraluminal type, is a good indication for our laparoscopic wedge resection. Because our surgical procedure has evolved to minimize deformation of the stomach after surgery for lesions close to the gastroesophageal junction and the pylorus ring, it can be indicated for various lesions regardless of tumor location. In any event, the lesions should be carefully handled without directly gripping the tumor during resection.
Patient positioning and placement of the trocars
The patient is in a supine position with legs spread apart. When the GIST is located proximal to the gastric angle, the operating surgeon stands on the left side of the patient. However, if the lesion is distal to the gastric angle, the surgeon stands on the right side of the patient. The assistant stands on the opposite side from the operating surgeon, and the scopist stands between the legs of the patient to perform the procedure.
For the placement of trocars, a 12-mm trocar is inserted by the open method in the umbilical region as a port for the camera, and pneumoperitoneum is then performed using 8 mm Hg of carbon dioxide. A 12-mm trocar is inserted as the surgeon's right-hand port, and a 5-mm trocar is inserted as the left-hand port; these ports are placed below the costal arch and in the flank of the patient on the side where the surgeon is standing. For the assistant, a 5-mm trocar is inserted in the flank of the patient on the side where the assistant is standing.
Surgical technique
The gastric content should be aspirated sufficiently to allow us to clearly recognize the contour of the tumor even in cases of intraluminal GIST (Fig. 1). The operating surgeon handles the tumor by holding tissue surrounding the tumor and performs seromyotomy using an electric scalpel or ultrasonically activated device along the outer edge of the tumor (Fig. 2). During this procedure, a direct grip on the tumor should be avoided as far as possible to remove the tumor and its surrounding pseudocapsule without rupturing it.
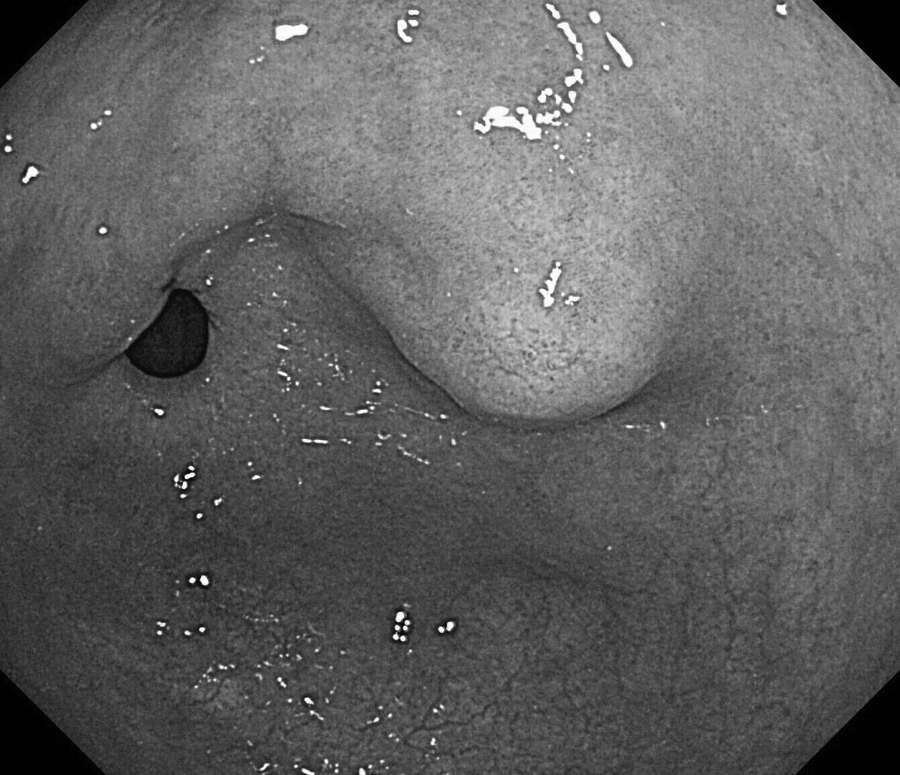
Upper gastrointestinal endoscopy demonstrates an intraluminal gastric gastrointestinal stromal tumor close to the pylorus ring.

The contour of the tumor, the same tumor as in Figure 1, is clear after a sufficient aspiration of gastric content. Laparoscopic seromyotomy around the outer edge of the tumor is performed using an electric scalpel or ultrasonically activated device.
The tumor gradually protrudes like an extraluminal tumor as seromyotomy proceeds; it is important to start with seromyotomy on the caudal side of the tumor toward the cranial side (Fig. 3).

The intraluminal gastric gastrointestinal stromal tumor gradually protrudes like an extraluminal tumor as the seromyotomy proceeds.
Although only one trocar is usually arranged on the assistant's side at the start of operation, an additional one should be placed for the assistant when exposure of the surgical field is inadequate.
When seromyotomy along the tumor comes up to the point where the tumor sufficiently turns over the gastric serosa, the tumor looks like a pedunculated extraluminal GIST.
After having confirmation of a complete hemostasis on the exfoliated surface of the gastric wall, two traction sutures are placed on the stomach lateral to the dissection lines for the tumor (Fig. 4), and two seromuscular sutures using 3-0 polyglactin 910 (Vicryl®; Ethicon Endo-Surgery, Cincinnati, OH) are applied to close the exfoliated seromuscular layer (Fig. 5).

Two traction sutures are applied to the outer edge of the tumor.
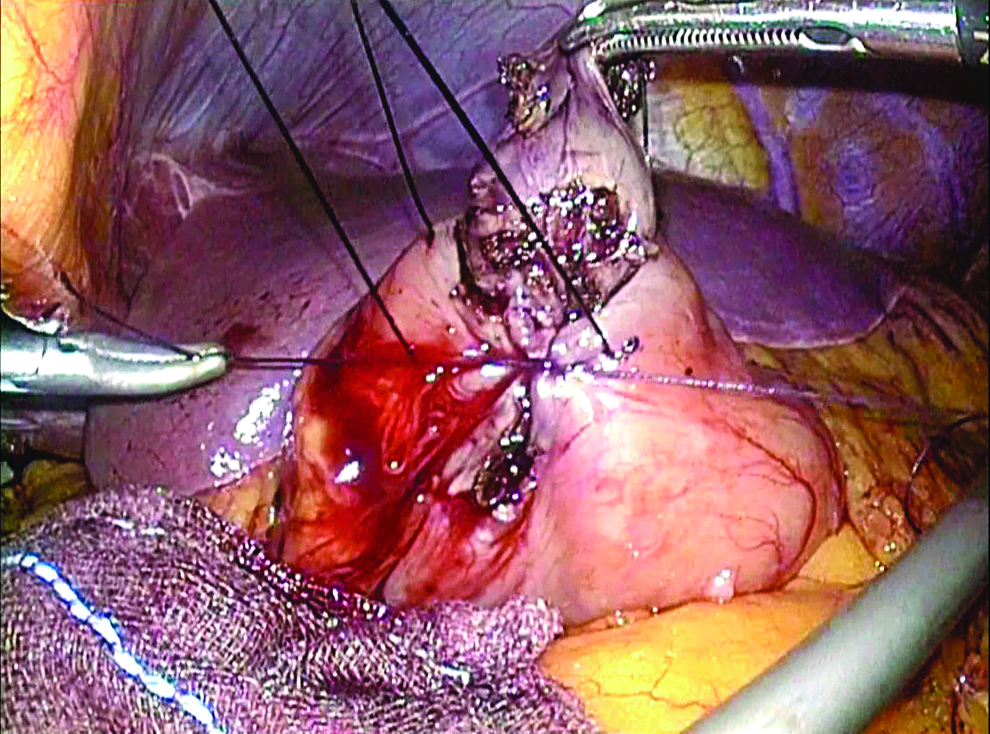
A seromuscular suture is placed to close the exfoliated seromuscular layer.
Finally, a complete tumor removal with minimal seromuscular resection is accomplished by applying Endo GIA™ (Covidien, Norwalk, CT) (Fig. 6). At this time, the tips of two seromuscular sutures are held, by using forceps in the operating surgeon's left hand and that of the assistant, and then pulled up toward the ventral side so that the staple line is aligned in line with the minor axis of the stomach. If it is likely that a considerable deformation or stenosis of the stomach occurs, an intraoperative endoscope examination should be used to avoid such complication before firing the endoscopic stapler, or the tumor resection and subsequent seromuscular sutures should be performed manually. The procedure is completed after checking that there is no hemorrhage in the surgical field (Fig. 7).
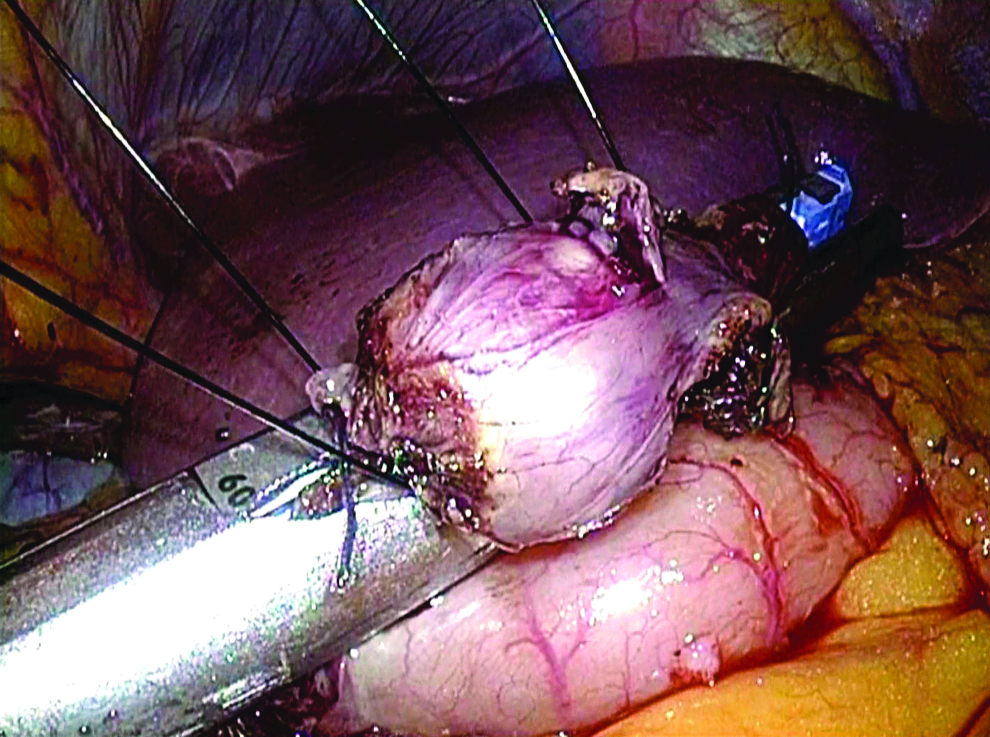
Resection of the tumor and closure of the gastric seromuscular layer are performed simultaneously by applying Endo GIA.

The procedure is completed with no placement of abdominal drains.
Results
This laparoscopic procedure was performed on 5 patients with gastric GIST: 4 men and 1 woman. The patients ranged in age from 49 to 73 years, with a mean of 59 years. Three tumors were located close to the gastroesophageal junction, no more than 3 cm at the junction, and two tumors were located near the pylorus ring, within less than 4 cm at the pylorus ring. All tumors were of an intraluminal growth type. The operative time averaged 98 minutes, ranging from 78 to 121 minutes. Blood loss during the operation was 2 mL on average and ranged from 0 mL to 5 mL. The operation required one trocar in 2 patients and two trocars in 3 patients for the assistant.
The average tumor size was 2.4 cm in diameter, ranging from 1.7 cm to 3.2 cm. A complete tumor clearance with negative microscopic margins was achieved in all patients. Immunohistochemical examination revealed that all tumors were at low risk.
All patients resumed oral ingestion on the day after surgery and showed no signs of postoperative hemorrhage, anastomotic constriction or obstruction, or gastric stasis.
Discussion
Laparoscopic partial gastrectomy has been developed as a minimally invasive surgery for submucosal tumor and early cancer of the stomach, but the difficulty in performing the procedure depends heavily on the location, size, and growth pattern of the tumors. 10
Extraluminal gastric GISTs are a good indication for laparoscopic surgery and can be easily managed by a laparoscopic simple wedge resection using a linear stapler. 11 In contrast, intraluminal gastric GISTs and tumors located close to the gastroesophageal junction or pylorus ring are challenging in performing a laparoscopic surgery because simple wedge resection using a linear stapler usually requires an excessive resection of the gastric wall, resulting in deformation and stenosis of the stomach. Various laparoscopic procedures for intraluminal tumors have thus been reported.12–15 For example, there has been a report of a hybrid technique that involves applying the endoscopic submucosal dissection technique to make a full-thickness incision in the stomach under laparoscopic guidance, extending the full-thickness incision along the outer edge of the tumor, and resecting the tumor.11,12 The lesion lifting method has been developed as a variation to minimize the postoperative deformation of the stomach when dealing with intraluminal gastric tumors. This method is extremely useful and creative, but it has some drawbacks, including an excessive resection of the gastric wall. 13 Intragastric surgery has evolved to overcome this drawback, and an accurate tumor resection has become possible by this procedure. It is disappointing that intragastric surgery also has its drawbacks, namely, (1) its indication is restricted to the posterior wall lesions, (2) the working space inside the stomach is narrow, and (3) it is extremely difficult to treat tumors around the gastroesophageal junction or pylorus. 16
With respect to laparoscopic surgery for GISTs, the 2012 NCCN Guidelines state that (1) the tumor must be removed without damaging it and that (2) the resected specimen must be collected in a plastic bag to prevent port-site recurrence, but the Guidelines fail to specify the details of how to deal with gastric GISTs in accordance with the size, location, and growth pattern of the individual tumors. 17 With recent advances in laparoscopic techniques and development of various surgical devices, several clinical trials have been conducted to clarify whether laparoscopic surgery would be equivalent to open surgery for gastric GISTs.5–8
Our laparoscopic procedure for gastric GISTs is simple and allows us easy and precise removal of tumor and closure of the gastric wall with a minimum necessary resection, regardless of location and growth form of the tumors. Because tumors can be excised without opening the gastric lumen, even in patients with ulcers on the mucosal surface of the tumor, the risk of tumor seeding, port-site recurrence, and surgical-site infection could be avoided. Our procedure may thus lead to a breakthrough in laparoscopic surgery, especially for intraluminal gastric GISTs and tumors nearby the gastroesophageal junction or pylorus ring.
The indication for our technique should be restricted to GISTs smaller than 5 cm in size because large tumors may result in postoperative gastric deformation. In addition, the surgeon should carefully handle the tumor without an inadvertent grip on the tumor and neighboring gastric wall, as the pseudocapsule is fragile. It is also important to pay attention not to cut through the tumor with the laparoscopic linear stapler. An intraoperative luminal endoscopy is useful to avoid such a serious complication. A plastic bag for collecting the resected specimens is indispensable to prevent injury to the pseudocapsule and subsequent spread of tumor cells.
The number of patients with GIST is increasing with recent advances in imaging studies, and the number of patients requiring surgery is also expected to rise. Further accumulation of patients and evaluation of long-term outcome are needed to clarify the advantage of laparoscopic surgery for GISTs.
Footnotes
Disclosure Statement
No competing financial interests exist.