
Abstract
Abstract
The current rate of bile duct injury (BDI) after laparoscopic cholecystectomy is 0.4%, which is an unacceptable outcome. Several surgical approaches have been suggested to mitigate the occurrence of this dreaded complication. We propose a standardized approach, using Calot's node as a critical anatomical landmark to guide gallbladder dissection and avoid BDI. We retrospectively analyzed a prospectively gathered database of 907 laparoscopic cholecystectomies using this standardized approach in our practice over a 5-year period. To date we have had no BDI and no cystic duct leak. Therefore, we suggest identification of Calot's node as an additional method to avoid BDI during laparoscopic cholecystectomy.
Introduction
B
Many operative techniques have been described that are intended to help guide the surgeon to better identify the extrahepatic biliary anatomy to prevent BDI. In this study, we introduce a novel landmark, the node of Calot, that, when used appropriately, should help reduce the occurrence of BDI in laparoscopic cholecystectomy. Furthermore, we present our standardized approach to laparoscopic cholecystectomy, which greatly aids in visualization of the critical anatomy of the operation and that systematically approaches the dissection in a safe manner, allowing us to accomplish our low BDI rate.
Materials and Methods
We retrospectively analyzed a prospectively gathered database of laparoscopic cholecystectomies using a standardized approach in our practice over a 5-year period. Partial cholecystectomies were excluded from the analysis. All cases were defined as “acute” or “non-acute,” based on final pathology records of the amount of inflammation. The level of inflammation, timing of operation, and any complications were recorded to assess the outcomes of our technique.
Our standard technique involves insufflation of the abdomen with a Veress needle, allowing optimal placement of the optical port at a variable point between the umbilicus and the xiphoid process (determined by the patient's body habitus) (Fig. 1). Our trocar placement, although standardized, does not lock the surgeon into the umbilicus for placement of the optical port. In this way, we optimize, by at least 30°, the ability to visualize the critical anatomy essential to proceeding with a safe dissection. The camera line of vision will cross above the transverse colon and directly face the triangle of Calot. The key element of our standardized technique is the identification of the lymph node of Calot, which is used as a landmark to avoid close dissection to and injury of the common bile duct. Reliably, the node rests superior to the cystic duct, lateral to the common hepatic duct, and anterior to the cystic artery. Once the node is identified, the end of the gallbladder or infundibulum is marked anteriorly.
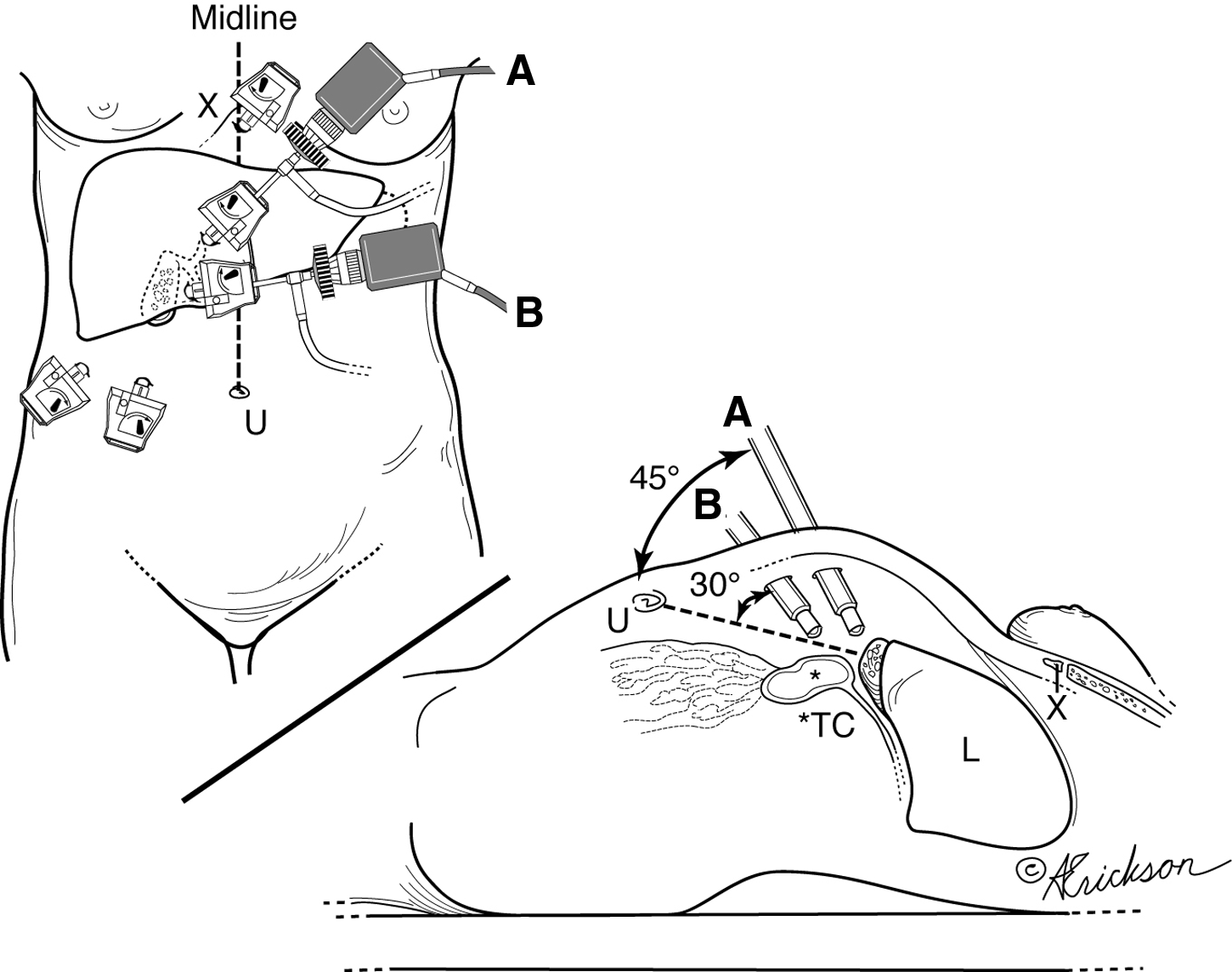
Camera placement options for safe gallbladder dissection (3 cm to the right of the midline). A, alternate site, with camera placement halfway between the umbilicus (U) and the xiphoid (X); B, regular camera site placement one-third of the way between U and X. L, liver; TC, transverse colon.
Dissection then proceeds to divide the peritoneal layer behind the infundibulum. The distal gallbladder is pulled (rotated) medially and cephalad, and the peritoneum is sharply and bluntly dissected posterolaterally as high as possible on the gallbladder along a line 1 cm away and parallel to the liver bordering the lateral wall of the gallbladder (Fig. 2). This posterior dissection will often identify the posterior cystic artery. In this case the plane of dissection must remain anterior to the cystic artery, separating it from the gallbladder wall. This will avoid injury to the liver bed. A thorough and extensive posterior dissection will reduce the tissue resistance to the anterior circumferential dissection (Fig. 2, inset) and may on rare occasions create a complete circumferential window.
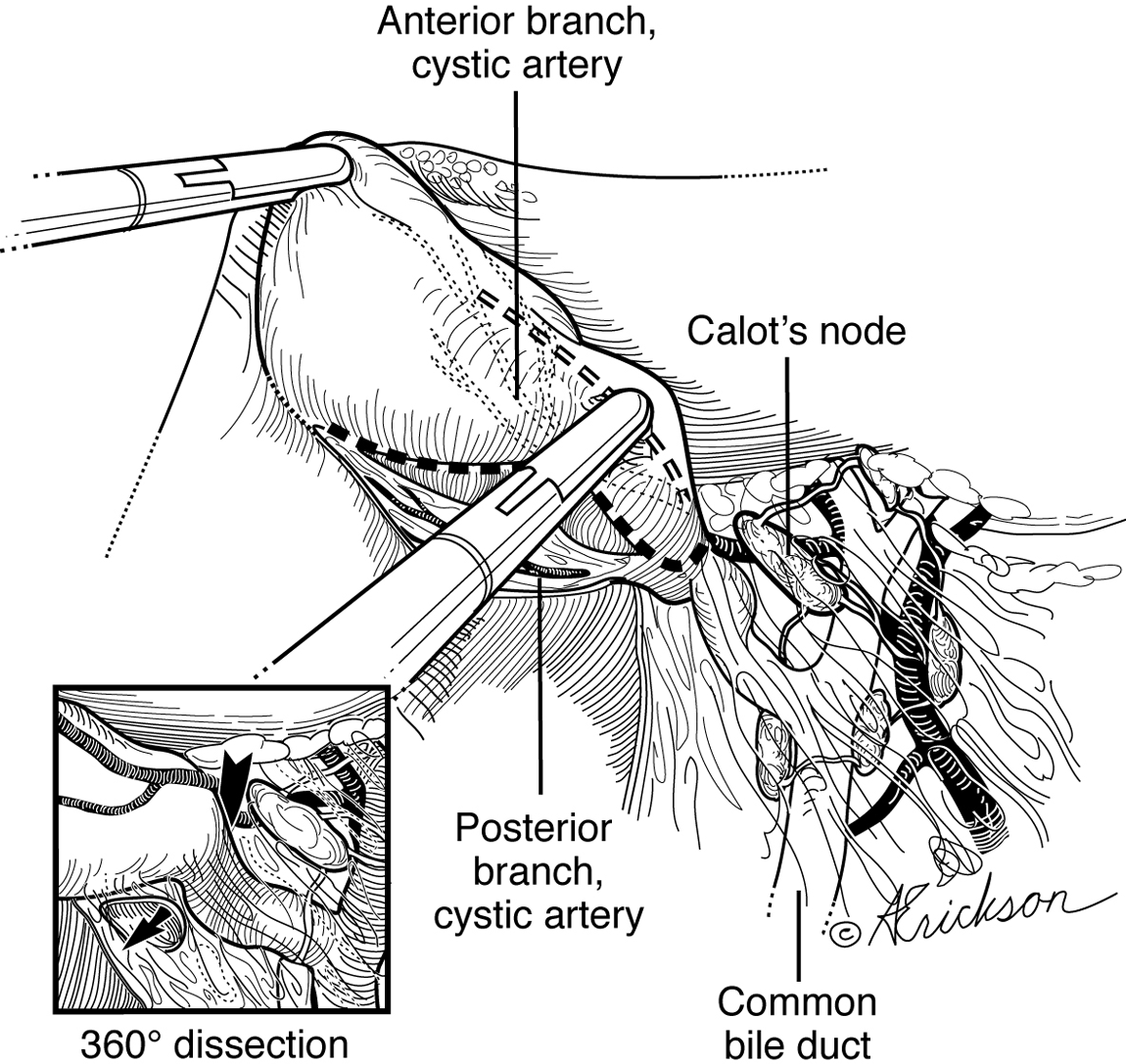
The distal gallbladder is pulled (rotated) medially and cephalad, and the peritoneum is sharply and bluntly dissected posterolaterally as high as possible on the gallbladder along a (dotted) line 1 cm away and parallel to the liver bordering the lateral wall of the gallbladder.
Anteriorly, the next fundamental step in the technique is to stay caudad and lateral to the node when beginning the dissection near the infundibulum (Fig. 3). In that area one stays safely away from the common hepatic duct, common bile duct, and right hepatic artery, which are, by definition, cephalad and on the other side of the node. The cystic artery is exposed and, once the critical view of safety has been achieved (two structures), can be clipped as it exits from underneath Calot's node and lateral to it, far from its origin on the right hepatic artery, thereby minimizing misperception of the two vessels (Fig. 3). The anterior line of dissection will complete the “parabola” started by the posterior line. The tubular structure that remains must be either the cystic duct or the infundibulum, which is fully revealed after then developing the critical view of safety (Fig. 2, inset). Dissection of the gallbladder off of the liver proceeds in the usual fashion, preferably dissecting on either side rather than from underneath, to minimize the risk of injury to the liver bed.
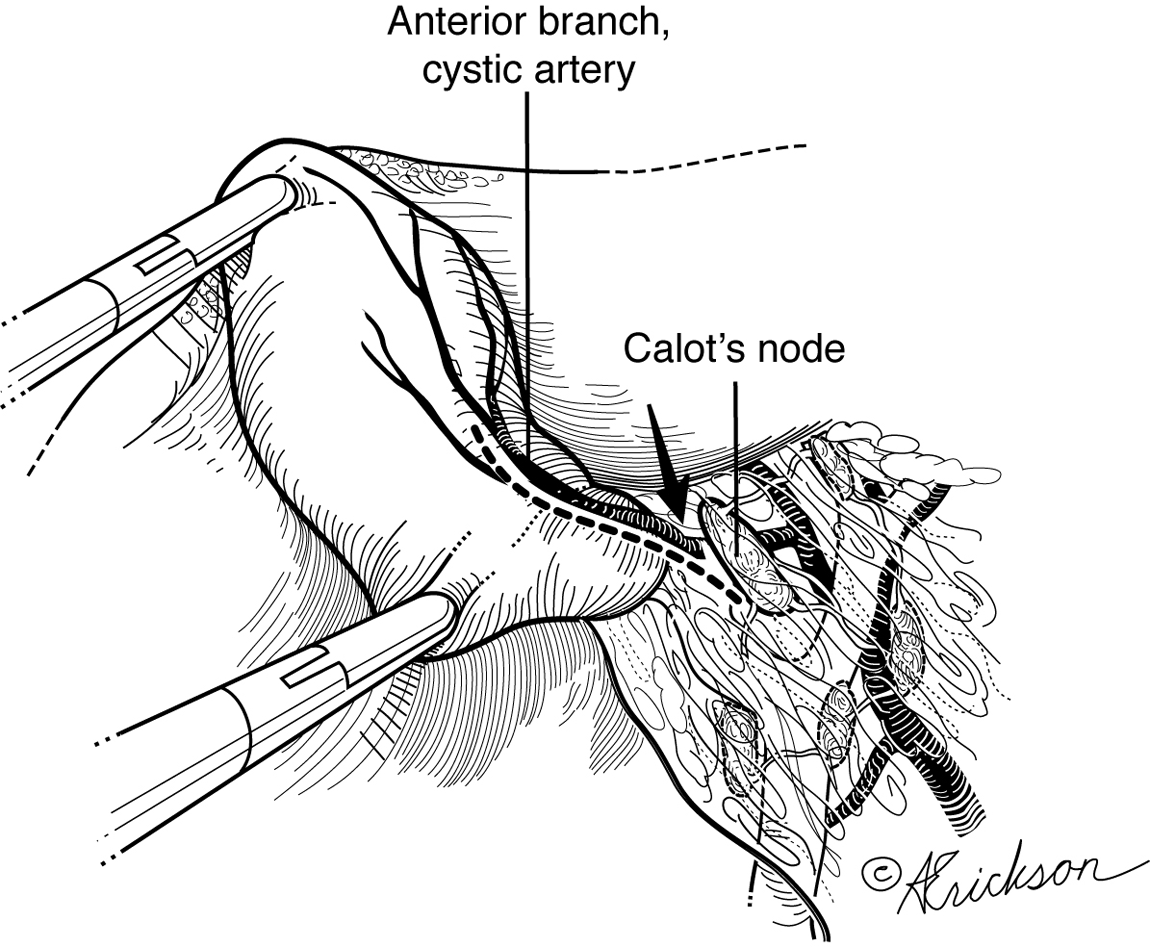
The anterior line of dissection (dotted line) completes the “parabola” started by the posterior line. The cystic artery is exposed and, once the critical view of safety has been achieved (two structures), can be clipped as it exits from underneath Calot's node and lateral to it, far from its origin on the right hepatic artery.
Results
Between January 2009 and December 2013, we performed 907 laparoscopic cholecystectomies using the standard steps described above with emphasis on recognition of the node of Calot as a landmark to avoid BDI. The patient population included 743 women and 164 men, with a mean age of 60.9 years (range, 12–90 years). Two surgeons performed all the operations. Of the 907 cholecystectomies, 117 underwent emergency operations, whereas 790 were scheduled on an elective basis. Of these, 813 were non-acute, whereas 94 were found to be acute. Two patients had Mirizzi's syndrome.
There were no specimens with malignancy. To date we have had no BDI and no cystic duct leak.
Discussion
The literature has suggested that the main cause of BDI is due to misidentification of the hepatobiliary structures, and not necessarily due to other patient, surgeon, or institution factors.2,3,11–14 In order to better identify the extrahepatic biliary anatomy, many approaches have been described. The role of intraoperative cholangiography has shown in some studies to help decrease the incidence of BDI.1,15,16 However, given other contradictory findings, the added time of the procedure, and perception of it being cumbersome, a consensus regarding the use of intraoperative cholangiography for prevention of BDI is still lacking. 17 Indeed, the use of routine intraoperative cholangiography has been shown to be only 44.6%. 18 More recently, techniques using florescence cholangiography have been suggested as being useful in delineating the anatomy; however, this approach is still being standardized and requires new equipment and injection of a chemical preoperatively. 19 A recent review of nine techniques to delineate this anatomy highlights the heightened interest and efforts being made to solve this problem. 20
Rather than using tools to help visualized the anatomy, many operative techniques have been described in order to minimize the risk of BDI. To better identify the biliary anatomy during laparoscopic cholecystectomy, a lot of attention has been paid to the so-called “critical view of safety,” as described by Strasberg et al. 21 This method describes achieving a 360° view of the infundibulum and body of the gallbladder in order to help identify a single duct entering the gallbladder from the region of the porta hepatis as, indeed, being the cystic duct. Although this technique has shown success and is becoming a standardized approach to laparoscopic cholecystectomy,20,22,23 many times this dissection is difficult to achieve in the face of anatomic variations and severe acute or chronic inflammation. Because of this, modifications have been described, such as the “endovesicular” technique 24 or using the subserosal dissection plane in challenging cases. 25 Laparoscopic partial cholecystectomy, by leaving the posterior wall of the gallbladder attached to the liver, has been shown to be effective as well. 26 The retrograde, or “fundus first,” laparoscopic cholecystectomy has been shown to be a viable option, particularly in obese patients. 27 In high-risk patients or those whose comorbidities or gallbladder disease is thought to be so severe that the fear of BDI outweighs the benefits of removing the gallbladder, percutaneous cholecystostomy tube drainage has been developed and has been shown to be an acceptable, temporizing modality.28,29 This procedure also promotes the proven beneficial multidisciplinary approach to this disease. 9
The critical view of safety is essentially ensuring correct identification of the structures of the triangle of Calot. A commonly identified, yet rarely talked about, landmark in identifying the structures of the triangle of Calot is the sentinel lymph node, referred to as Lunds's node, Mascagni's lymph node, or, as is here, Calot's node. Calot's node is present in all gallbladders directly within the hepatocystic triangle as described by Calot as the space between the common hepatic duct medially, the cystic duct laterally, and the cystic artery superiorly. Regardless of the amount of inflammation, this node is readily identified. At our institution, we regard Calot's node as the import landmark to ensure safe scoring of the peritoneum and to advance to deeper tissue planes. Using the technique described ensures the anatomic triangle cephalad to the Calot's node, delineated medially by the common hepatic duct and cephalad by the liver plate (Fig. 4) is not violated. Therefore, safe clipping and ligation of the cystic duct and artery are achieved far from their branching points off the common hepatic duct and right hepatic artery, which exist in that triangle. It is at this level of dissection and avoidance of this dangerous anatomic triangle that this technique becomes an essential adjunct to the “critical view of safety.”
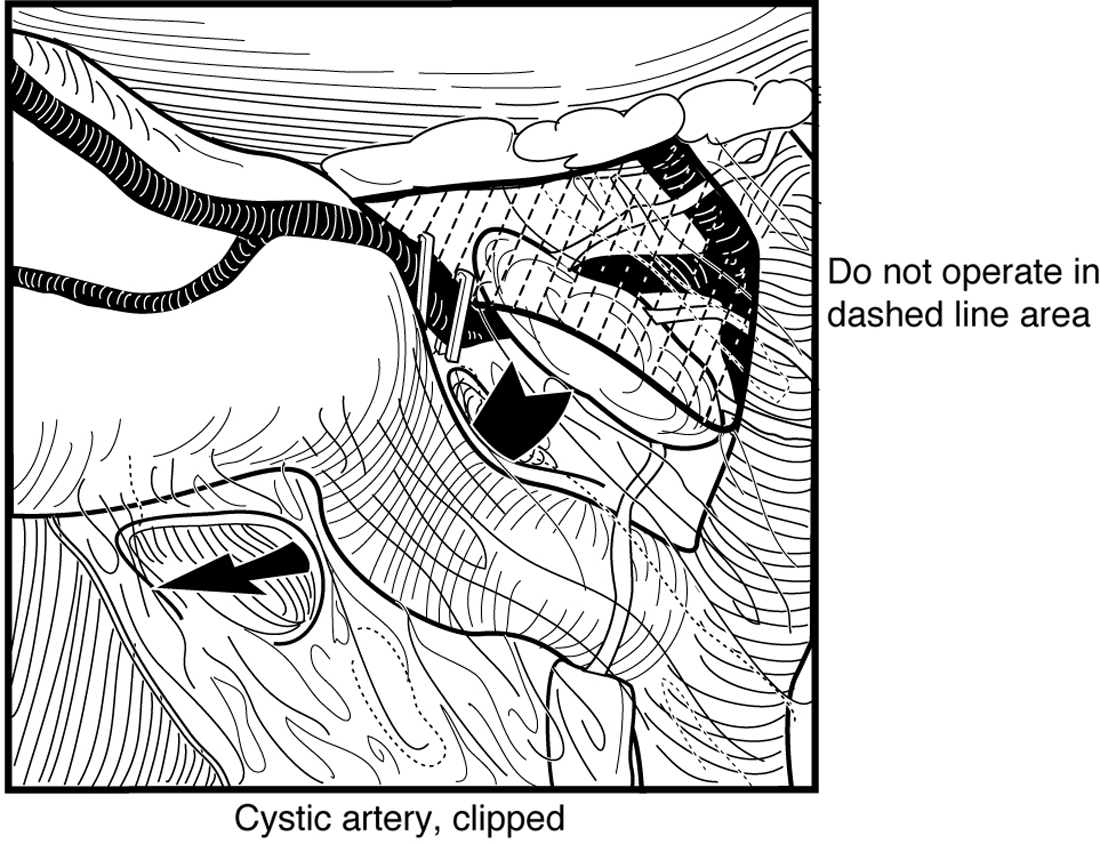
The anatomic triangle cephalad to the Calot's node, delineated medially by the common hepatic duct and cephalad by the liver plate, is not violated.
Because the node “rides” the cystic artery, when it presents itself on the inferior (caudal) aspect of the triangle of Calot, this indicates a transposition of the cystic artery with the cystic duct. The surgeon in this case should be even more careful in the dissection.
After 24 years of laparoscopic cholecystectomy being described for symptomatic gallbladder disease, the average rate of BDI of 0.4%, resulting in about 3000 cases, cannot been considered an acceptable outcome. In response, a duct injury mitigation has been suggested to standardize the surgical approach in hopes of improving this costly result. 30
Conclusions
The main cause of BDI is due to misidentification of the hepatobiliary structures. Numerous operative and imaging techniques have been described to avoid BDI with varying degrees of acceptance and success. Given the overall paucity of use of intraoperative imaging techniques and the success of critical view of safety, we propose the addition of recognizing the anatomical landmark of Calot's node to guide gallbladder dissection and enhance the safety, practicality, and effectiveness of dissection of the triangle of Calot in straightforward to difficult cases of laparoscopic cholecystectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.