
Abstract
Abstract
Purpose:
There is a lack of experience with fully covered self-expandable metal stents (SEMSs) for benign esophageal disorders in children.
Patients and Methods:
Eleven children (six boys, five girls) with a median age of 30.5 months (range, 1 month–11 years) who underwent treatment with SEMSs for a benign esophageal condition between February 2006 and January 2014 were recruited to this retrospective study. Etiologies included esophageal atresia with postoperative stricture (n=4), recurrent fistula (n=1), and/or anastomotic leak (n=1), as well as iatrogenic perforation of the esophagus following endoscopy (n=4) or laparoscopic fundoplication (n=1). As part of an interdisciplinary cooperation patients were jointly managed from the Department of Pediatric Surgery and Central Interdisciplinary Endoscopy at our institution.
Results:
Median duration of individual stent placement was 29 days (range, 17–91 days). In 4 cases up to four different SEMSs were placed successively over time. There were no complications noted at stent insertion or removal. At follow-up, 6 patients (55%) were successfully treated without further intervention. Two children each (18%) underwent one single dilatation after stent removal and remained well afterward. Three patients (27%) did not improve following stenting and required definite surgery. Minor stent-related complications were noted in 5 cases (45%), including gastroesophageal reflux (n=2), silent stent migration (n=2), and pneumonia (n=1).
Conclusions:
SEMSs for benign esophageal disorders in children can be used safely and effectively in selected cases, including esophageal anastomotic strictures, esophageal leaks following primary surgery, or perforations postdilatation. An SEMS can be applied either as an emergency procedure or as an adjuvant treatment further to endoscopy or previous surgery. Establishment of a standardized approach in the pediatric population is mandatory.
Introduction
E
Benign indications in which SEMSs have been used more or less successfully in adults are iatrogenic and spontaneous esophageal perforations, tracheoesophageal fistulas, and anastomotic leaks, as well as strictures from caustic and idiopathic causes.2,3
Children may develop esophageal sequelae from a variety of causes, including ingestion of corrosives, gastroesophageal reflux (GER), eosinophilic esophagitis, drug injuries, sclerotherapy, radiation, fibrotic healing after surgical repair of esophageal atresia (EA), idiopathic conditions, and iatrogenic injuries. 4 Physicians dealing with this group of patients have begun to explore the use of stents. However, data are limited to case reports and small series only, particularly regarding the application of SEMSs in children.5–7
Because commercially available esophageal stents are generally inappropriate in size for pediatric patients, customized stents or devices that are approved for other organ systems (e.g., airway stents) have been used previously.8–10 At present, esophageal stents are not widely used as a standard treatment in children and are usually considered when medical and endoscopic treatment fails. 11
We report our interdisciplinary experience with fully covered SEMSs for the treatment of benign esophageal conditions in children.
Patients and Methods
Eleven children (six boys, five girls) who underwent treatment with an SEMS for a benign esophageal condition between February 2006 and January 2014 were recruited to this retrospective study (Table 1). As part of an interdisciplinary approach patients were jointly managed from the Department of Pediatric Surgery and Central Interdisciplinary Endoscopy at our institution. The overall median age at stent placement was 30.5 months (range, 1 month–11 years).
The patient died 12 months after stenting caused by comorbidity.
A second stent (10/40) was placed into the first stent in order to provide adequate overlap of the perforation site/fistula.
An attempt was made elsewhere to close a recurrent tracheoesophageal fistula using fibrin glue.
A second stent was placed to treat a stricture that developed following initial stenting of an esophageal perforation.
Distal migration of the stent was noted on chest X-ray or during stent removal, although the patient remained clinically well.
EA, esophageal atresia; F, female; GER, gastroesophageal reflux; M, male; PEG, percutaneous endoscopic gastrostomy.
Proximal esophageal lesion
This study includes seven infants (four boys, three girls) with a median age of 10 months (range, 1–32 months) who were treated for a proximal esophageal lesion following repair of EA. The vast majority of patients (6 out of 7) developed a postoperative anastomotic stricture that was associated with significant dysphagia. Of these patients, 5 had undergone a primary esophageal repair previously. One child (patient 2) suffered from a stricture after gastric transposition for a long-gap EA. In another case, a boy (patient 6) developed an anastomotic leak resulting in severe mediastinitis following thoracoscopic repair of a type Vogt IIIb EA.
In 3 cases an SEMS was placed primarily without previous intervention (Fig. 1). Three other patients had recurrent endoscopies prior to stent placement, including 1 patient who had undergone more than 10 dilatations and subsequent treatment with mitomycin C and triamcinolone.
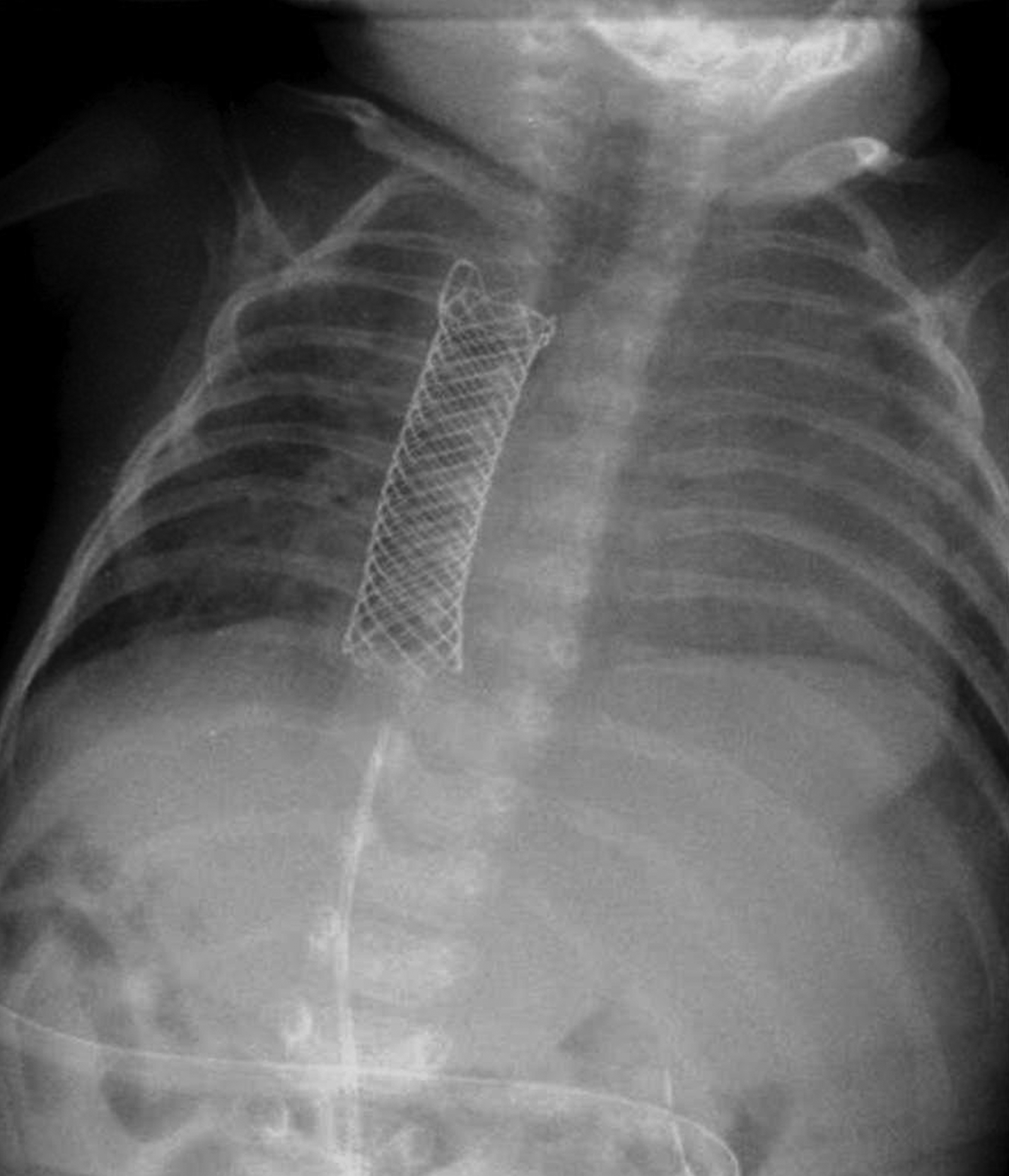
Stent covering a proximal esophageal stricture (patient 5) (chest X-ray).
A 3-month-old girl (patient 7) underwent stenting for a proximal esophageal stricture as well as for a recurrent tracheoesophageal fistula. She was referred to our center from another hospital, where an attempt failed to close the fistula endoscopically by using fibrin glue.
Mid-esophageal lesion
A 17-month-old girl with an underlying neurological disorder developed mediastinitis and septicemia following insertion of a percutaneous endoscopic gastrostomy tube in another hospital. Subsequently, a contrast study revealed a mid-esophageal perforation. An SEMS was inserted, and during the same anesthesia procedure a thoracic abscess was drained.
Distal esophageal lesion
Three older children (two boys, one girl), 25 months, 7 years, and 11 years old, suffered from a leak of the distal esophagus. In 2 patients with achalasia and GER, respectively, a perforation occurred on endoscopy and was treated primarily with an SEMS (Fig. 2). An 11-year-old boy (patient 11) underwent laparoscopic fundoplication for severe GER in another hospital during which the distal esophagus was perforated; in a second operation a drain was placed laparoscopically, and the patient was transferred to our institution, where an SEMS was inserted under endoscopic guidance.
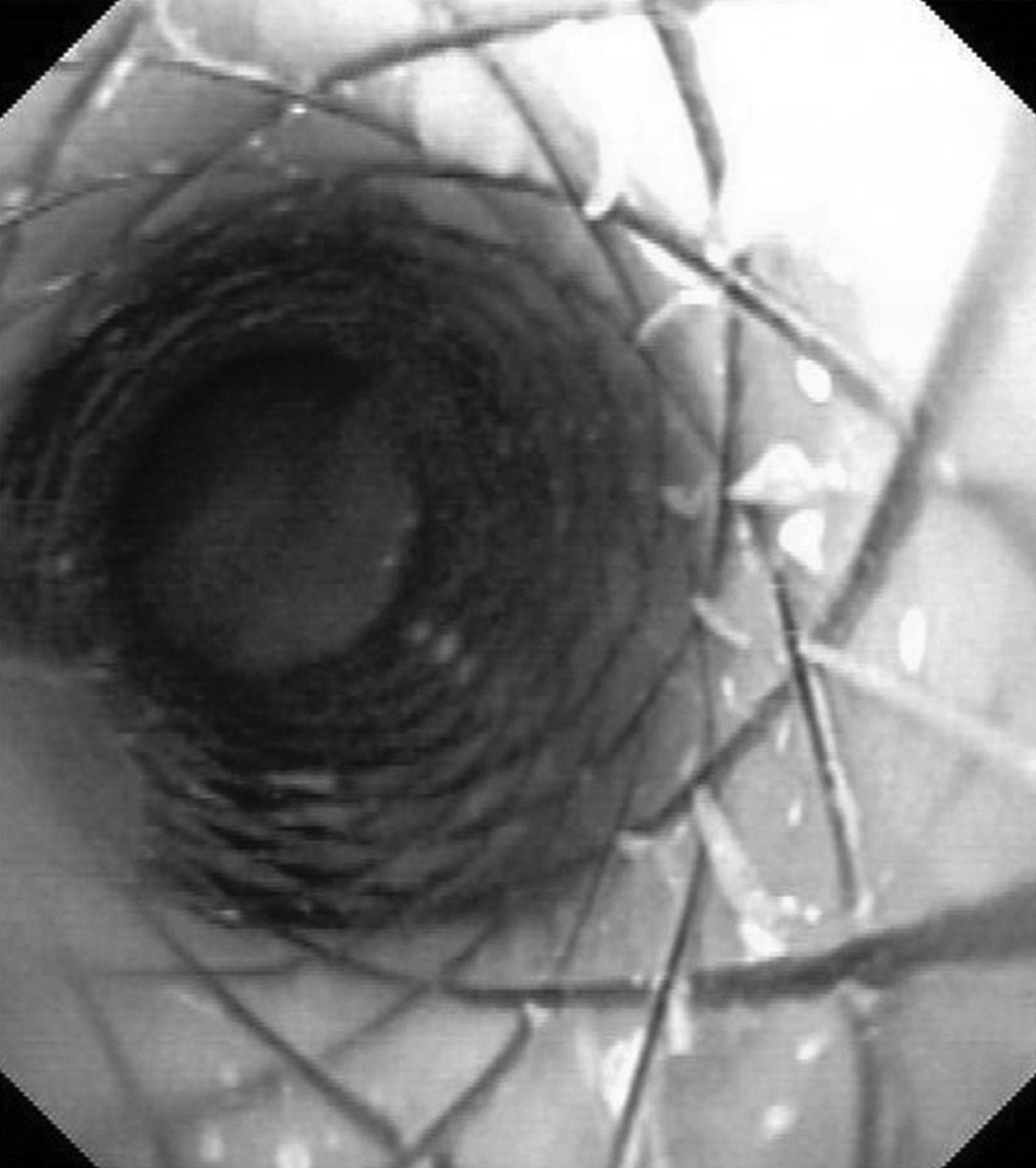
Stent covering a distal esophageal perforation (patient 10) (endoscopic view).
In 9 patients biliary SEMSs (WallFlex®; Boston Scientific Corp., Natick, MA) were used. Over time, in one of these children (patient 7) a biliary stent was changed to a wider bronchial stent (Hanarostent®; Mi.I. Tech, Seoul, South Korea). In 2 other cases (patients 1 and 11) a Precision Colonic Ultraflex stent system (WallFlex) or a bronchial stent (Hanarostent) was used. Depending on the patient's age and the location of the esophageal lesion, the stent diameter varied from 10 and 16 mm with a length between 40 and 100 mm.
All stents were inserted via endoscopic guidance with the patient under general anesthesia. Simultaneous fluoroscopy was not required in any case. The stents were coated with silicone and had radio-opaque markers. In each patient a chest X-ray was taken 24 hours postoperatively to confirm the position. In general, the children were fed orally according to age as tolerated (i.e., breast or formula milk in infants and solids in children). Those patients who required an alternative feeding approach because of their underlying illness (e.g., impaired swallowing, neurological disorders) were partly fed via a gastrostomy or jejunostomy tube that was already in place prior to stenting.
The children were discharged from the hospital once they had recovered with the stent being in situ and were regularly followed up as outpatients. No further investigation was performed until stent removal, which was carried out using a flexible endoscope and a biopsy forceps. On Day 1 after removal, a contrast study was carried out generally to confirm whether the treatment had been successful. Simultaneously the patient was assessed clinically, particularly for signs of dysphagia and GER. All children received omeprazole (0.7 mg/kg/day) while the stent was in place.
The median follow-up following stent removal was 18 months (range, 1–67 months).
Results
The median duration of individual stent placement was 29 days (range, 17–91 days). Seven out of 11 patients were treated with one stent only. In 4 cases up to four different SEMSs were successively placed. Therefore the absolute stenting time increased up to 189 days.
One girl (patient 8) was primarily treated with an SEMS for a mid-esophageal perforation following percutaneous endoscopic gastrostomy tube insertion. Following stent removal after 29 days, the lesion was closed on endoscopy. Subsequently the patient developed dysphagia, and a contrast study revealed a stricture at the level of the previous perforation. A second stent was placed and left for another 28 days.
Two children each had a total of three stents inserted: 1 patient with a severe proximal stricture (patient 1) was treated with three colonic stents for 21, 17, and 28 days, respectively. In another boy (patient 6) a biliary stent was placed over a proximal anastomotic leak; on Day 8 a second stent was inserted into the first in order to provide adequate seal of the perforation site (Fig. 3). Both stents were removed and replaced by a longer and wider biliary stent on Day 50 because the perforation had not fully healed at that time.
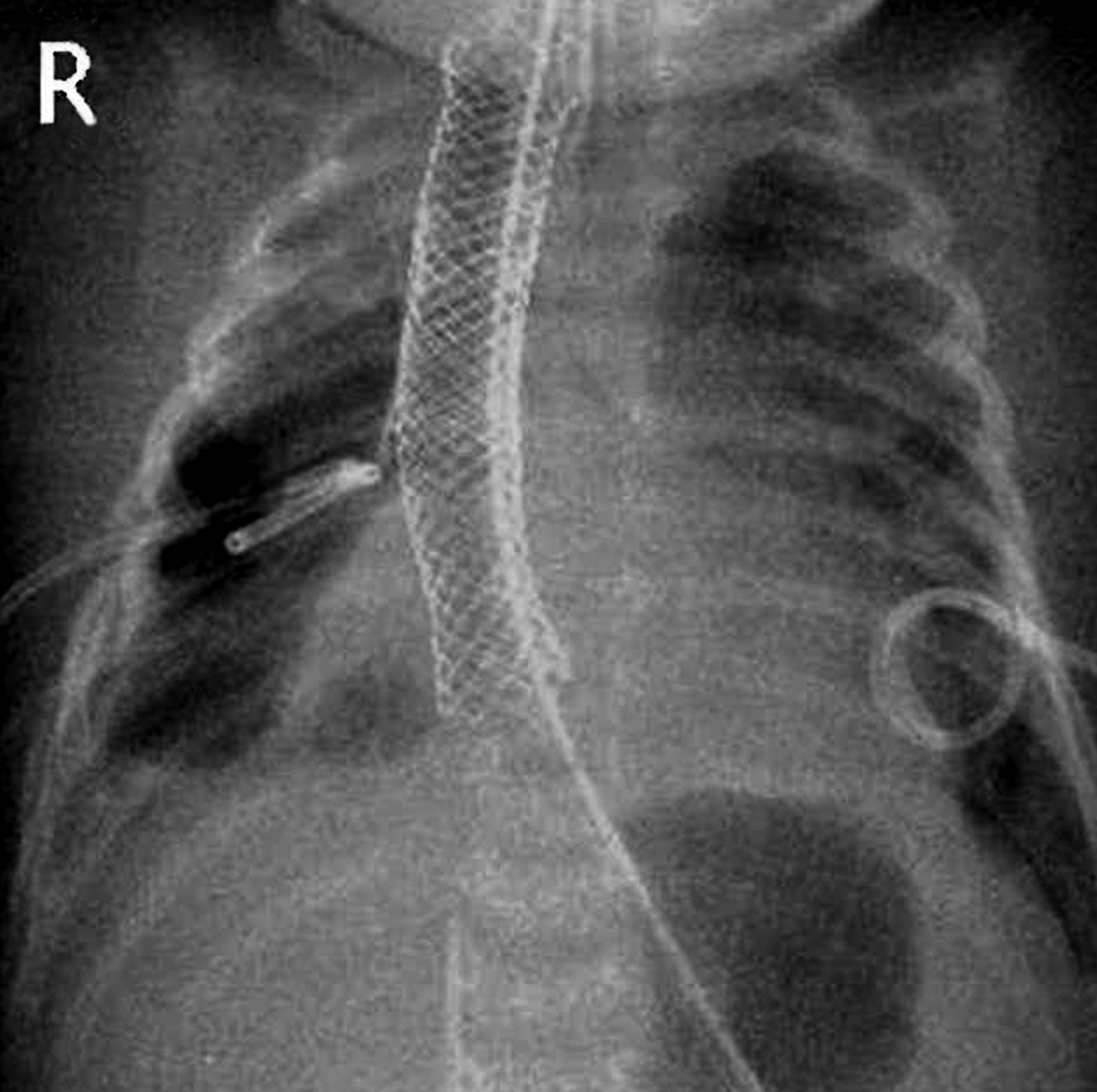
Telescoping of a second stent into the first stent in order to provide adequate overlap of the lesion (patient 6) (chest X-ray).
A 3-month-old girl with a proximal stricture following EA and a recurrent tracheoesophageal fistula (patient 7) had a total of four stents inserted. In the course of treatment two overlapping biliary stents were replaced by a wider bronchial stent. Finally an attempt was made to close the persistent fistula with fibrin glue and another biliary SEMS.
Two patients with a stricture after EA repair (patients 3 and 4) developed mild GER in the course of treatment, which settled after stent removal. In another two children (patients 9 and 10) the stents had migrated distally into the stomach. The migration was “silent” and was noted only accidentally during stent removal. These children remained clinically stable without any signs of GER or dysphagia, and there were no complications noted with stent placement or removal in both cases. The girl who was treated for a proximal stricture and recurrent tracheoesophageal fistula developed aspiration pneumonia because the first stent did not provide a sufficient overlap of the fistula site. The patient settled on antibiotics and remained stable after the stent had been replaced with a wider device. Therefore the overall complication rate with a stent in situ was 45% (5 out of 11 patients).
Nine out of 11 patients underwent a contrast study following stent removal. Of these, 4 patients had a good result and remained subsequently well. In 2 other patients an esophageal stricture and a leak, respectively, could not be detected anymore. However, the contrast showed GER associated with the underlying condition (patient 4 with congenital diaphragmatic hernia and patient 11 with cerebral palsy). In 3 cases the contrast revealed a persistent pathological finding (patients 1, 7, and 9). The latter finally underwent surgery.
Two other patients had an endoscopy at the time of stent removal during which no further stricture was detected. These two children (patients 3 and 10) had been clinically well throughout stenting. Therefore they were not given a further contrast meal.
Overall, 6 out of 11 patients (55%) remained well at last follow-up without problems and the need for further treatment. Two children each (18%) underwent one dilatation after stent removal. One female infant (patient 3) with a proximal stenosis following EA repair and stricture resection required another dilatation 11 months after stent removal for mild dysphagia. Subsequently she remained well, and endoscopy at the age of 2 years was normal. The girl who had been treated for an esophageal leak and had a second stent inserted for a newly developed stricture (patient 8) suffered still from mild dysphagia. One month following stent removal she underwent esophageal dilatation once and improved.
Three patients (27%) did not improve following stenting and underwent surgery. Patient 1, who already had had numerous dilatations and medical treatment prior to stenting, underwent stricture resection and end-to-end anastomosis; subsequently the patient improved without further treatment. Another girl (patient 9) with achalasia continued having dysphagia after stenting. She improved following Heller's myotomy and since then has remained well. The girl with a proximal stricture and recurrent fistula following EA repair (patient 7) underwent a re-thoracotomy with excision of the persistent fistula and had been well at last follow-up.
There were no complications noted related to stent placement or to stent removal.
One child (patient 4), who suffered also from bronchopulmonary dysplasia associated with congenital diaphragmatic hernia, died 8 months after stent removal due to respiratory failure.
Discussion
Fully covered SEMSs offer several advantages over traditional dilatation techniques, including continuous, radially oriented dilatation over a certain period and preservation of tissue ingrowth by a polyurethane covering.4,7,11 Nevertheless, the use of SEMSs for benign esophageal disorders in children is still being discussed in the literature. At present, stent placement is only considered in children when medical and endoscopic treatment fails. 11
In contrast to the advances in materials and technology, specially designed esophageal stents for children relative to their age and size are not available. As commercially available esophageal SEMSs are usually inappropriate in size, polypropylene stents, 12 biodegradable stents,6,13 bronchial plastic stents, 8 customized stents, 10 or airway stents 7 have been previously used. In the United States esophageal SEMSs are not approved by the Food and Drug Administration for late removal or temporary use for leaks and fistulas. 3 Placement of stents that are originally designed for other organs, such as the trachea, bronchus, biliary tract, or colon, in the esophagus is still an “off-label” technique in the pediatric population.8,11,14
In our study, in the vast majority of patients an expandable biliary metal stent was used. In 2 cases a second biliary stent was placed simultaneously (telescope technique) because of an inadequate overlap of an anastomotic leak or fistula. We have chosen this technique also because of the fact that by the time of re-scoping no other (i.e., longer) commercial stent was available. Best et al. 4 reported on benign esophageal strictures combined with fistulas or leakage after EA in infants. They applied a fully covered tracheobronchial nitinol stent in their series, but also considered expandable biliary metal stents as an alternative for the use in small children. Rollins and Barnhart 7 described three children with persistent esophageal leaks resistant to nonoperative therapy: a 5-month-old male infant was treated with a fully covered tracheobronchial stent, whereas two other children, 23 and 36 months old, had esophageal nitinol stents inserted. A telescope technique was used as well. 7
In this study the number of stents applied in each patient ranged between one single SEMS only and four different stents that were placed in one girl suffering from a stricture and recurrent tracheoesophageal fistula after EA repair. This is in accordance with other authors: Best et al. 4 reported on the subsequent placement of up to four different stents in their series, and Rollins and Barnhart 7 used two stents in two children each. In our opinion major factors that contribute to the fact that multiple stents are required in some patients are the lack of adequate commercial available SEMSs at the time of stenting and the uncertainty regarding the maximum stenting time before experiencing adverse effects such as formation of granulation tissue or migration.
Approximately 8%–52% of infants with EA develop a postanastomotic fibrotic stricture caused by predisposing factors.4,11 Esophageal dilatation is the treatment of choice with a 58%–96% success rate. 11 However, major complications have been reported with this method, including perforation, anastomotic leakage, and recurrent fistula. 11 Moreover, sociopsychological morbidity caused by the number of dilatations must not be underestimated in this context. Therefore esophageal stenting has become an attractive alternative for the treatment of postanastomotic strictures. 11
Other well-known sequelae associated with EA repair are esophageal perforations and anastomotic leaks. In such cases Rollins and Barnhart 7 preferred a nonoperative management and recommended stent placement when conservative therapy (i.e., keeping the child nothing by mouth, administration of antibiotics, drainage) fails. However, there might be a delay of treatment with prolonged hospital stay, increasing risk of developing comorbidities and higher costs, once conservative management fails. Immediate SEMS placement may offer an effective alternative.7,8,11 To the best of our knowledge this is the first study using primary stent placement as an emergency treatment option in children. In this study stenting was performed immediately in 6 out of 11 patients (55%), 2 of whom suffered from an anastomotic stricture and 4 of whom suffered from an esophageal perforation. In 5 other patients, stent placement followed a previous therapy, such as dilatation with or without injection of mitomycin C and triamcinolone, closure of a fistula with fibrin glue, or drainage.
Overall, our complication rate was 45%, including stent migration, GER despite omeprazole therapy, and aspiration pneumonia caused by a persistent tracheoesophageal fistula. Similarly, Best et al. 4 reported an overall complication rate of 43% in their series, including stent migration, gagging, and respiratory distress. Rollins and Barnhart 7 observed a stent migration in 1 out of 3 patients.
Further complications that were noted following esophageal stenting in children included tissue overgrowth at the end of the stent, obstruction, perforation, bleeding from erosion into an adjacent vessel, and an incarcerated prosthesis resulting in severe ulcerative esophagitis.4,8,15 However, we did not notice such problems in our series.
In this cohort, in contrast to other authors,5,11 in our study there was no need for intraoperative fluoroscopy at the time of stenting because the SEMSs were coated with silicone and had radio-opaque markers. As described by others,5,7 a chest X-ray was taken on Day 1 after stent insertion to confirm the correct position and expansion of the stent. Subsequently we neither routinely confirmed the position of the stents with water-soluble contrast media nor performed recurrent esophagoscopies in order to check for erosions as suggested in the literature.4,7
This study is limited by its retrospective approach and the small number of patients. Moreover, we did not formally compare stent placement with our previous treatment (e.g., balloon dilatation, drainage) and can therefore make no conclusion regarding which treatment is superior. Nevertheless, follow-up revealed clinical success in 6 out of 11 patients (55%); after stent removal these children, including one boy with a stricture following gastric transposition, had fully recovered. Even in newborns suffering from critical illness, stent placement was able to stabilize the patient and to avoid further surgery.
Of the 3 patients who failed treatment (27%), one boy, who had undergone already numerous dilatations including application of local chemotherapy prior to stenting, subsequently required open stricture resection. In this context we agree with Foschia et al., 10 who stated that an esophageal stricture with transmural fibrosis caused by dilatations, mitomycin C, and triamcinolone is a negative prognostic factor for stent placement. Another girl who did not improve following stenting suffered from primary undiagnosed achalasia. She recovered only once Heller's myotomy was performed. In adults the application of stents in patients with achalasia has been reported as an alternative, effective, safe method of treatment.16,17 However, in this regard we are not aware of any studies related to the pediatric population.
In a third patient, in whom a wide tracheoesophageal fistula was resistant to fibrin glue and stenting, definite surgery was also required. In adults with tracheoesophageal fistulas associated with esophageal cancer, stenting is used as a palliative tool. 18 Clearly, there is a lack of experience with applying stents for congenital tracheoesophageal fistulas in infants. In this context SEMSs may play an important role as an adjuvant treatment measure, particularly in those children who are clinically instable and suffer from other associated conditions. Nevertheless, based on our experience, surgical excision is recommended in cases with recurrent tracheoesophageal fistulas.
Duration of stent placement is still being discussed controversially in the literature. In our study the median time until stent removal was 29 days (range, 17–91 days). In contrast to other authors,4,7,15 we did not observe significant granulation tissue, and contrary to the manufacturer's guidelines, we extended the time of stenting up to 3 months. With a view to the literature, Best et al. 4 reported a median time of stent duration of only 7.2 days (range, 3–15 days). Another case series with three children between 5 months and 3 years of age revealed a maximum stenting time between 3 and 4 weeks. 7 We are only aware of one 12-year-old boy with a peptic stenosis in whom the stent remained in situ for 3 months before it was removed successfully. 19
In conclusion, the use of SEMSs for benign esophageal disorders is safe and often successful with only one single application even in infants and small children. Based on our experience, primary stent placement seems to be a promising tool for the treatment of esophageal anastomotic strictures and leaks following EA repair as well as for perforations following esophageal dilatation. Moreover, in selected cases, stent insertion may gain some time in order to optimize the patient's condition prior to definite surgery. Our data revealed that children with recurrent tracheoesophageal fistula formation and achalasia seem to benefit less from stent treatment. Because of the absence of commercially manufactured, age-related stents, biliary, bronchial, or colonic SEMSs can be used as an alternative. Establishment of a standardized approach in the pediatric population is mandatory.
Footnotes
Disclosure Statement
F.K. has received research support from Erbe Elektromedizin Tübingen, Karl Storz Endoskope Tuttlingen, and Boston Scientific Corp. International. B.L., R.K., and L.M.W. declare no competing financial interests exist.