
Abstract
Abstract
Purpose:
Thoracoscopic plication of the diaphragm is an alternative to conventional surgical treatment of diaphragmatic evisceration via thoracotomy in neonates and infants. The aim of this study is to compare results of treatment by these two methods in the past 11 years.
Materials and Methods:
We studied the data of 35 neonates who underwent standard posterolateral thoracotomy (18 patients; Group I) or video-assisted thoracoscopic surgery (17 patients; Group II) for diaphragmatic plication. The two groups were compared for patient demographics, operative reports, and postoperative parameters.
Results:
The groups were similar in terms of demographics and preoperative parameters. There was a significant difference in mean operative time between the open and thoracoscopic procedure (71.67 minutes versus 51.76 minutes; P<.05). Duration of care in the neonatal intensive unit and length of hospital stay were significantly shorter in Group II (5.89 days versus 3.23 days [P<.05] and 13.06 days versus 9.88 days [P<.05]). Early postoperative complications (hemothorax, pneumothorax) were frequent in the thoracotomy group (Group I) (16.67% versus 0%; P>.05). Recurrence of diaphragmatic evisceration was observed only in the thoracotomy group (11.11% versus 0%; P=.486).
Conclusions:
Thoracoscopic plication of the diaphragm in infants in the first 3 months of life demonstrates better results than open surgery.
Introduction
N
At our institution thoracoscopic plication of the diaphragm has become a favored and effective method of treatment. Between 2002 and 2012 we extensively used thoracoscopic plication in neonates and infants in the first 3 months of life. Comparative results of open and thoracoscopic methods of treatment of diaphragmatic evisceration provided the basis of this study.
Materials and Methods
We demonstrate our own experience in thoracoscopy in neonates with eventration of the diaphragm arising from a muscular anomaly of the diaphragm or birth trauma. Since 2002, in our Department of Neonatal Surgery, surgical treatment has been given to 35 patients with diaphragmatic evisceration caused by congenital muscular malformation or paralysis occurring after birth. The study divided these patients into two groups: Group I consisted of 18 infants who underwent diaphragmatic repair using open surgery, and Group II consisted of 17 patients with diaphragmatic reconstruction by means of thoracoscopy. Patients requiring open repair belong to the historical cohort and were operated on before the start of minimally invasive surgery in our hospital.
All patients had respiratory disorders of various degrees before the operation. We applied artificial lung ventilation (ALV) in patients with acute respiratory compromise. The remaining patients required noninvasive breathing support, and appropriate gas exchange for them was provided by oxygen supply through a nasal cannula or mask. The preoperative chest X-ray confirmed the high position of the hemidiaphragm requiring plication.
Open plication
The patient was placed on the operating table in the lateral position opposite to the affected side. Posterolateral thoracotomy was performed in the eighth intercostal space. After cranial retraction of the lung tissue, we performed descending of the surplus of the degraded portion of the diaphragm with gradual movement of the liver, bowels, stomach, and spleen into the abdominal cavity. After evaluation of the diaphragm tissue structure, we approximated the edges of the muscular part and firmly fixed them by interrupted sutures. Occasionally, in the case of any risk of bleeding after surgery, we inserted a drainage tube into the pleural cavity. The surgical intervention was completed with wound suturing of the chest.
Thoracoscopic plication
The thoracoscopic plication procedure is illustrated in Figures 1–3. Surgical intervention was performed with the patient under general anesthesia with the use of artificial pulmonary ventilation. The patient was placed on the operating table in the lateral position with the body rotated up to 90°. We used carbothorax with soft parameters: pressure of 4–5 mm Hg and flow rate of 0.5 L/minute. Rarely, to facilitate repositioning of the organs into the abdominal cavity, the pressure of carbon dioxide was raised for a short time to 7–8 mm Hg. Next, three thoracoports were installed. We placed the trocars as high as possible. The first trocar for the thoracoscope was placed into the second or third intercostal space; the other two trocars were interposed into the fourth intercostal space through the mammillary line and posterior axillary line. Such arrangement of the thoracoports creates quite a large working space to perform maneuvers for plication of the diaphragm. Working space for surgery would be much narrower if the trocars were placed much lower. Stretched like a membrane, the cupula of the diaphragm under the influence of carbothorax becomes flat.

Eventration of the right hemidiaphragm: the general view at the beginning of plication.
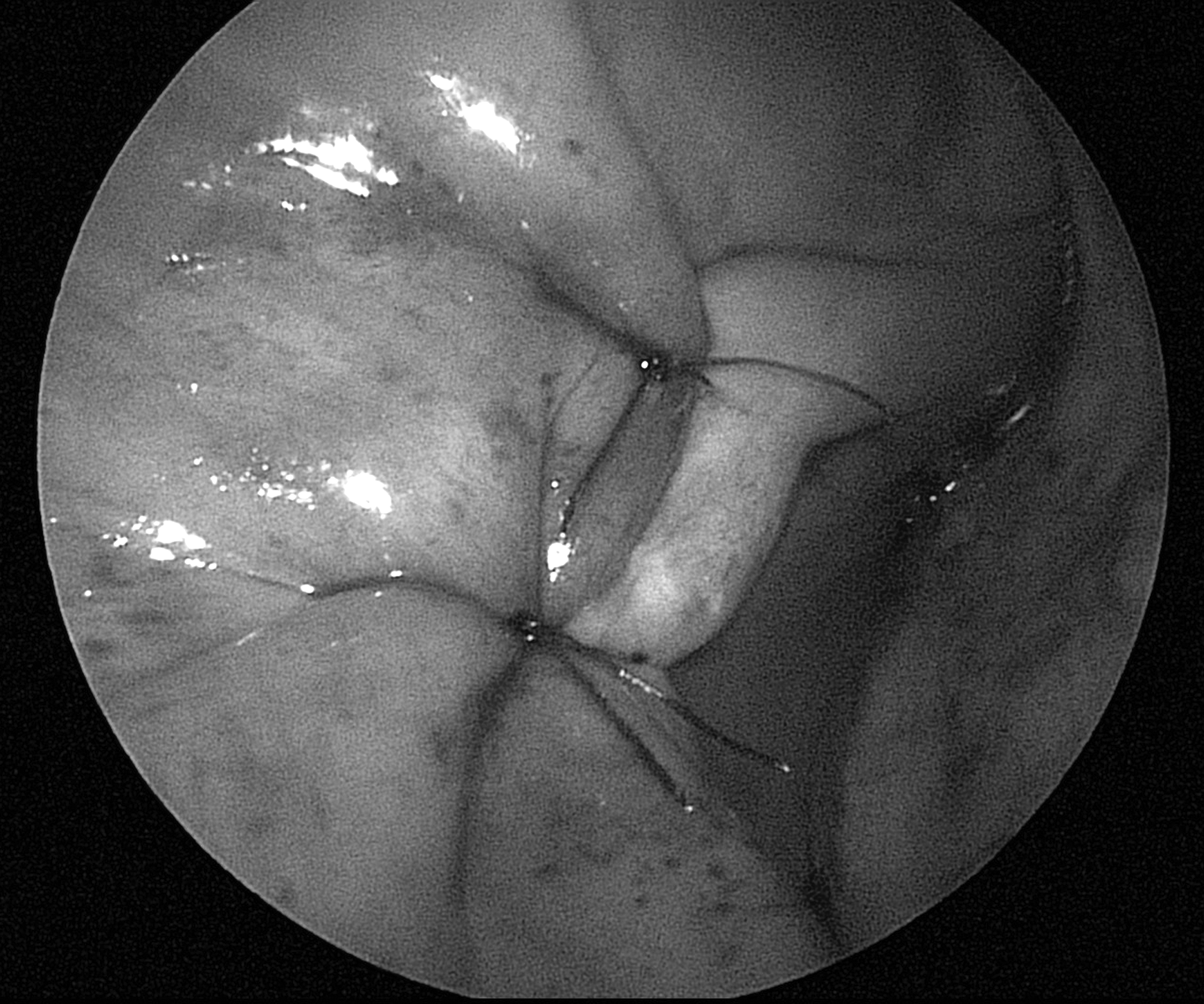
The stage of invagination of the diaphragmatic dome and suturing with single-stay sutures.
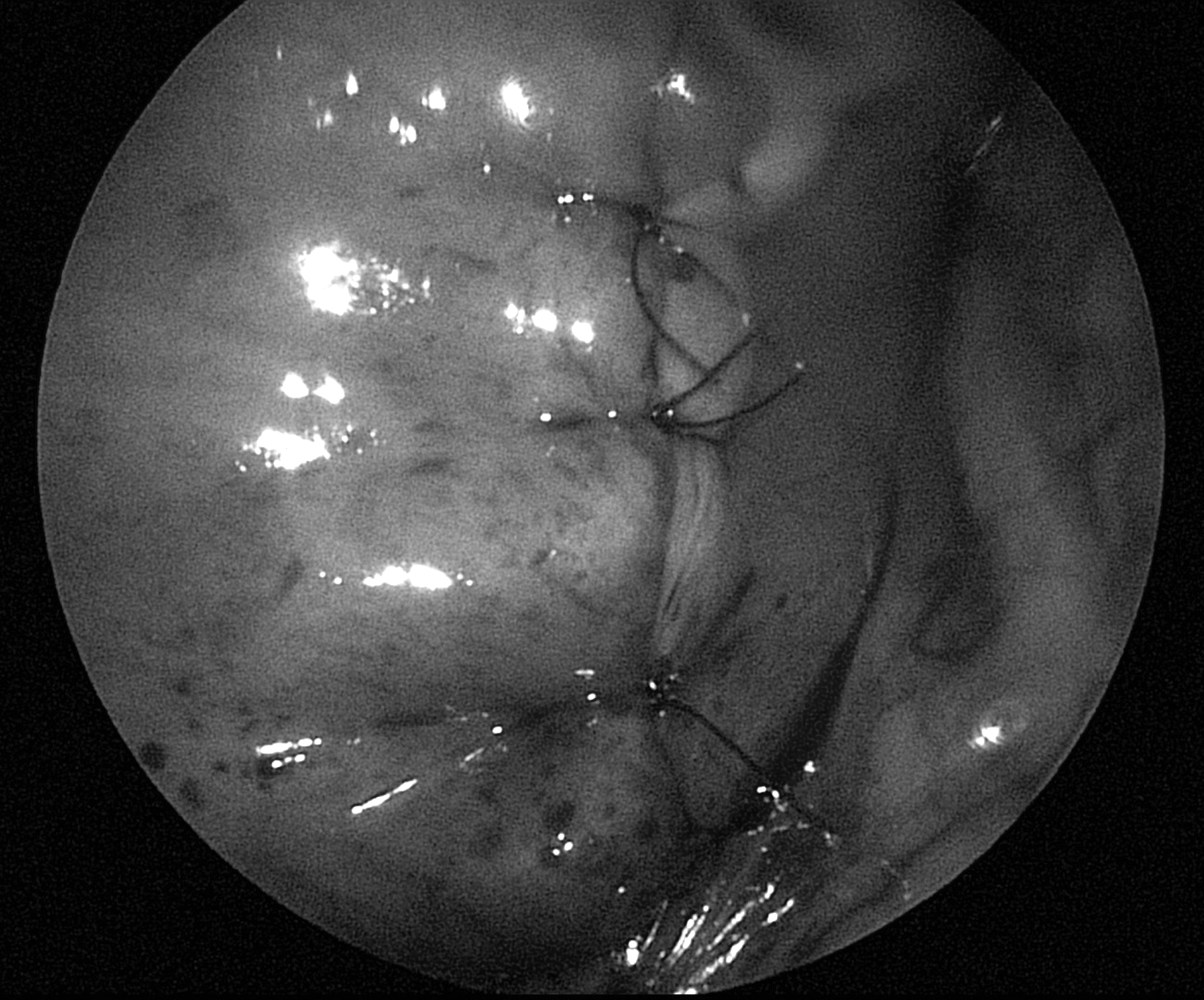
View of the diaphragm after plication.
In the direction from the periphery to the center of the mediastinum, transversely to the pericardial–diaphragmatic sinus, we performed descending of the surplus of the diaphragm into the abdominal cavity and sutured the interrupted, nonabsorbable stitches (3/0 or 4/0 polypropylene [Prolene®; Ethicon, Somerville, NJ]) on the edges of the muscle tissue remaining after the invagination. Sutures were tied outside the chest. Rarely, through the posterior instrumental port we installed a drainage tube (8 French), which was joined with the aspiration system. Next, the lung was re-expanded, and the thoracoports were extracted. Skin incisions were covered with adhesive strips (SteriStrip™; 3M, St. Paul, MN).
After surgery, all infants underwent radiographic and ultrasound investigations of the chest to check the level of the diaphragm. Later, diagnostic methods became necessary only in cases when symptoms of fluid or air accumulation in the pleural cavity appeared. Avoiding ALV became possible because of the effective recovery of spontaneous breathing. After stabilization of their respiratory and hemodynamic status, patients were transferred to the neonatal intensive care unit (NICU). Monitoring of postoperative complications was carried out during the patients' hospital stay and during repeated outpatient visits at 3, 6, and 12 months after discharge from the surgical center.
In the final stage of the study we made a comparison of demographic data, the number of concomitant anomalies, intra- and postoperative characteristics, and immediate and long-term results of surgical interventions. The groups of patients were subjected to statistical comparison. We analyzed preoperative parameters (sex, body weight, and age at time of surgery, affected side, ALV application before surgery, and the presence of concomitant malformations). We also compared intra- and postoperative parameters: duration of the operation, duration of postoperative ALV, duration of NICU and hospital stay, and early and late postoperative complications. To estimate the average parameters in the groups, we used the Mann–Whitney U test. The value of P<.05 was accepted as the confidence level of significance. To rate the categorical variables, we used the Yates' corrected chi-squared test or Fisher's exact test.
Results
Preoperative parameters
The preoperative parameters of the two groups of patients are given in Tables 1 and 2. It was found that there were no significant differences between the groups in weight, age, sex, or frequency of concomitant pathology. Paralysis of the diaphragm was revealed in infants of both Group I and Group II with almost identical rates (27.78% and 29.41%, respectively). The average weight of infants in the thoracoscopic group was 3504.82 g (range, 1200–6700 g), which was slightly lower than that of the open treatment patients (3660.56 g; range, 1560–6885 g). There were equal proportions of male and female patients. At the time of operation, the average age of infants was 31 days in Group I and 32.88 days in Group II. Pulmonary artery pressure before surgery was 25.37 and 28.12 mm Hg in Groups I and II, respectively, and the difference was not statistically significant (P>.05). Right-sided eventration was much more frequent than left-sided eventration in both groups (72.22% and 64.71%, respectively). Respiratory support before the operation was applied in an equal number of patients in both groups. ALV was necessary for 61.11% of Group I infants and 58.82% of Group II infants. Concomitant anomalies (cardiac malformations and genetic malformations) were present in almost equal proportions of patients (38.89% versus 35.29%, respectively).
Group I patients received thoracotomy; Group II patients received thoracoscopy.
By Mann–Whitney U test.
ALV, artificial lung ventilation; NICU, neonatal intensive care unit; POD, postoperative day; SD, standard deviation; SEM, standard error of the mean.
Group I patients received thoracotomy; Group II patients received thoracoscopy. Data are number of patients (%).
By Yates' corrected chi-squared test.
By Fisher's text.
ALV, artificial lung ventilation.
Intraoperative parameters
The comparative analysis of patients' characteristics revealed the presence of significant differences between the groups relating to duration of the operation. Duration of thoracoscopic surgery was 52±8 minutes (range, 40–70 minutes). Duration of open surgery was significantly higher, at 72±9 minutes (range, 60–90 minutes). There were significant differences between the groups (P<.05) in the use of the pleural tube (94.44% vs. 29.41%).
Postoperative results
Comparative study of patients' characteristics showed significant differences in postoperative parameters between the groups regarding duration of ALV, stay in the NICU, and surgical hospital stay.
Duration of postoperative ALV was lower in the group receiving thoracoscopic treatment (4.4 versus 1.76 days), as was the postoperative NICU stay (5.89 versus 3.23 days). Mean pulmonary arterial pressure in the postoperative period efficiently came down and was 20 mm Hg and 22.75 mm Hg, respectively, on Day 5 after surgery. Postoperative hospital stay was much shorter in patients in the minimally invasive treatment group (9.88 days versus 13.06 days). There was no mortality in the thoracoscopic group. Two (11.11%) patients of the thoracotomy group died, but death was connected with a genetic disorder (Edward's syndrome).
Early postoperative complications such as hemothorax and pneumothorax were found only in patients of Group I (n=16, 67%). In all cases of accumulation of blood and air, re-operation was not required, and the problem disappeared within a few days after hemostatic therapy and long-term thoracostomy.
Results of postoperative monitoring over a period of 3 months to 7 years were available in all infants of Group I and Group II. In our region there is only one pediatric hospital, and therefore we had a 100% opportunity to observe all children after operation. Relapse occurred only in patients of the open treatment group (11.11%). Gastroesophageal reflux was found in equal proportions of patients (16.67% and 17.65%, respectively) in the postoperative period.
The analysis of perioperative data demonstrated the principal qualities of minimally invasive treatment of diaphragmatic evisceration in neonates. They consisted in the reduction of operative time, reduction of the time of ALV, reduction of patients' stay in the NICU and hospital due to the decrease in incidence of postoperative complications (accumulation of blood and air, recurrence), and the absence of early and late postoperative mortality.
Discussion
Evisceration (eventration, paralysis) of the diaphragm in children is a rare and serious surgical condition. The etiology of diaphragmatic dysfunction may be primary, in consequence of diaphragmatic eventration with atrophy and absence of the muscular part of the diaphragm, or secondary, as a result of phrenic nerve injury.11–15 Neural injuries in neonates are often caused by tension and damage of the phrenic nerve during birth or may be iatrogenic, as a result of direct nerve trauma during cardiothoracic operations. In children undergoing cardiac surgery, the frequency of such injuries varies from 1.5% to 10%.11,12,14 When the phrenic nerve loses its function, the dome of the diaphragm displaces into the hemithorax and collapses the lung. Because of functional loss of the phrenic nerve, diaphragm movements become paradoxical; the stretched dome compresses the inferior and middle lobes of the left lung, as well as the upper lobe and, partially, the contralateral lung. Although some patients remain asymptomatic, others have symptoms of respiratory failure. According to studies, the loss of physiological diaphragm movement weakens the respiratory dynamics of adults as well as of children.11–14
Surgical treatment to reduce the stretched dome is necessary for patients with eventration of the diaphragm and dyspnea symptoms, including patients undergoing ALV. The vast majority of studies report on the use of posterolateral thoracotomy and open plication of the excess part of the respiratory muscle. Since 1995, there have been small numbers of reports16–18 about thoracoscopic or video-assisted repair of the stretched portion of the diaphragm by means of different techniques: invagination of the diaphragm and its plication using continuous sutures, 19 mechanical suturing at the bottom of the dome using the endostapler with excision of redundant diaphragm tissue, 20 and the application of multiple U-shaped sutures. 21 The first reported case of thoracoscopic plication in a newborn with congenital eventration of the diaphragm was published by Van Smith et al. 10 Currently, thoracoscopic plication of the diaphragm is a reasonable alternative to the standard thoracotomy. However, despite the obvious advantages, the method of thoracoscopic plication has still not received the complete approval of surgeons. The number of publications about the use of video-assisted plication in infants is limited.1–10 Results of these studies show that if plication is performed using thoracotomy, its effect is postponed because it is hidden owing to the loss of lung function associated with the postthoracotomy pain that retards the postoperative recovery. The effect of thoracoscopic plication, on the other hand, immediately becomes evident, as it is accompanied by minimal influence on pulmonary function due to the minimally invasive nature of the procedure.
There is no common point of view on the best types and methods of sutures to fix the diaphragm. Most surgeons believe that single stitches are better than continuous ones, although there are no convincing arguments that prove this statement5,22 except that a single-suture technique is much simpler, and there is no need for an additional thoracoport for applying continuous sutures.
Abraham et al. 4 reported that the first suture should be placed in the middle of the cupula of the diaphragm and can be applied without excessive effort, providing temporary fixation of the invaginated portion. In our institution, we started to perform plication in the lateral portion of the diaphragmatic dome. We believe that it is better if the suture line is located close to the mediastinum because here the diaphragm is thicker, and it is easier to regulate the tightness of stitches. Sato et al. 8 also recommend performing the plication from the peripheral portion of the diaphragm toward the mediastinum. The reason they gave is that directing the suture line from the periphery to the center prevents injuries of the phrenic nerve. However, it appears to be more logical to preserve the safety of the nerve by performing the plication in the opposite direction.
Currently, the progress made in endoscopic techniques and minimally invasive surgery allows a standard open approach for diaphragmatic plication by means of the endoscopic method. Advantages of minimally invasive surgery for the treatment of diaphragmatic eventration are well known in adult patients in terms of pain, cosmetic results, pulmonary function, and mortality.16,17 It has also been well demonstrated that although the majority of adult patients with postoperative paralysis of the diaphragm remain asymptomatic, sick infants cannot tolerate the loss of one functional lung as a result of diaphragmatic compression.11–14,23 There is a supposition that this poor tolerability is due to differences in lung morphology between children and adults. 24 The authors believe that it is due to a feature of infant lungs that consists in a lower correlation between the surface area of the alveoli and the weight of the lungs. The alveolar surface area increases up to the age of about 8 years and is connected with the rapid development of the alveolar part of the lungs, increasing the surface area of the gas diffusion.
Conclusions
The development of endoscopic technologies has led to the transformation of many thoracic operations into video-assisted procedures. The main argument in favor of endoscopy is the good postoperative lung function as a result of the low level of pain. Further advantages of thoracoscopy over thoracotomy are the absence of postoperative scars, disorders of pulmonary mechanics, and chronic pain. Thus, except in the case of pleuropulmonary adhesions, thoracoscopy has significant advantages and appears to be the preferable technique for the treatment of diaphragmatic eventration in infants.
Our study demonstrates that thoracoscopic plication is feasible in neonates and young children and may be successfully used even in premature neonates. Thus, thoracoscopic repair of the diaphragm for treatment of evisceration should be considered the preferred method for treatment of this condition in infants in the first 3 months of life.
Footnotes
Acknowledgments
We would like to thank Mrs. Anne M. Gale and Professor Vladimir Alexi-Meskishvili from German Heart Institute, Berlin, for editorial assistance and their support of this work.
Disclosure Statement
No competing financial interests exist.