
Abstract
Abstract
Purpose:
The aim of this study was the comparison of single-port and multiport laparoscopic methods for the treatment of inguinal hernia in children during the first 3 months of life.
Subjects and Methods:
Between January 2002 and December 2012, we performed 260 laparoscopic operations in neonates and infants with the diagnosis of inguinal hernia. Surgical procedures were single-port endoscopic herniorraphy (Group I; 180 patients) and multiport laparoscopic herniorraphy (Group II; 80 patients). The two groups were compared for demographics of patients, operative report, and early and late postoperative outcomes.
Results:
We applied the single-port laparoscopic method for correction of inguinal hernia in small babies. The mean operative time (duration of one-sided and bilateral repair) in Group I was 16 minutes, whereas the mean duration of the operation in Group II was 15.73 minutes. The number of doses of postoperative analgesia was 1.19 and 1.22, respectively. The length of hospital stay was 8.12 hours in Group I and 8.27 hours in Group II. No differences between the two groups were recorded in the follow-up period: no recurrence in either group and hydrocele formation in only 1 patient in Group II.
Conclusions:
There are similar functional results in treatment of inguinal hernia in babies during the first 3 months of the life using single- and multiport laparoscopy. Scarless cosmetic results are seen in the single-incision laparoscopic surgery group.
Introduction
T
With the intent to make surgery scarless, laparoscopy is constantly evolved. The search for new approaches has led to the new single-port technologies of laparoscopic treatment of an inguinal hernia. Currently, there is a relatively small number of scientific articles in the world literature devoted to the application of single-port laparoscopic surgery in small babies with inguinal hernia.2–4 The aim of our study is to demonstrate the results of single-incision herniorrhaphy and provide details comparing two laparoscopic methods (single-port and multiport) in the treatment of inguinal hernia in children of the youngest age group.
Subjects and Methods
Single-incision herniorrhaphy was performed in 180 of 260 patients up to 3 months of age who underwent minimally invasive treatment for inguinal hernia in the period between January 1, 2002 and December 31, 2012. The patients were divided into two groups. Group I consisted of patients who underwent single-port herniorrhaphy. The remaining 80 patients who underwent ligation of the hernia sac with application of an additional laparoport were included in Group II.
Technically, laparoscopic ligation of the hernia sac consisted of the preperitoneal passing and subcutaneous tying of polypropylene suture placed around the internal inguinal ring, regardless of the number of laparoscopic ports placed. Ozdegiz et al. 5 were the first to make public this treatment technology, termed subcutaneous endoscopically assisted ligation (SEAL). The modification of the method we proposed was in the application of a surgical Tuohy needle that is intended for epidural anesthesia.
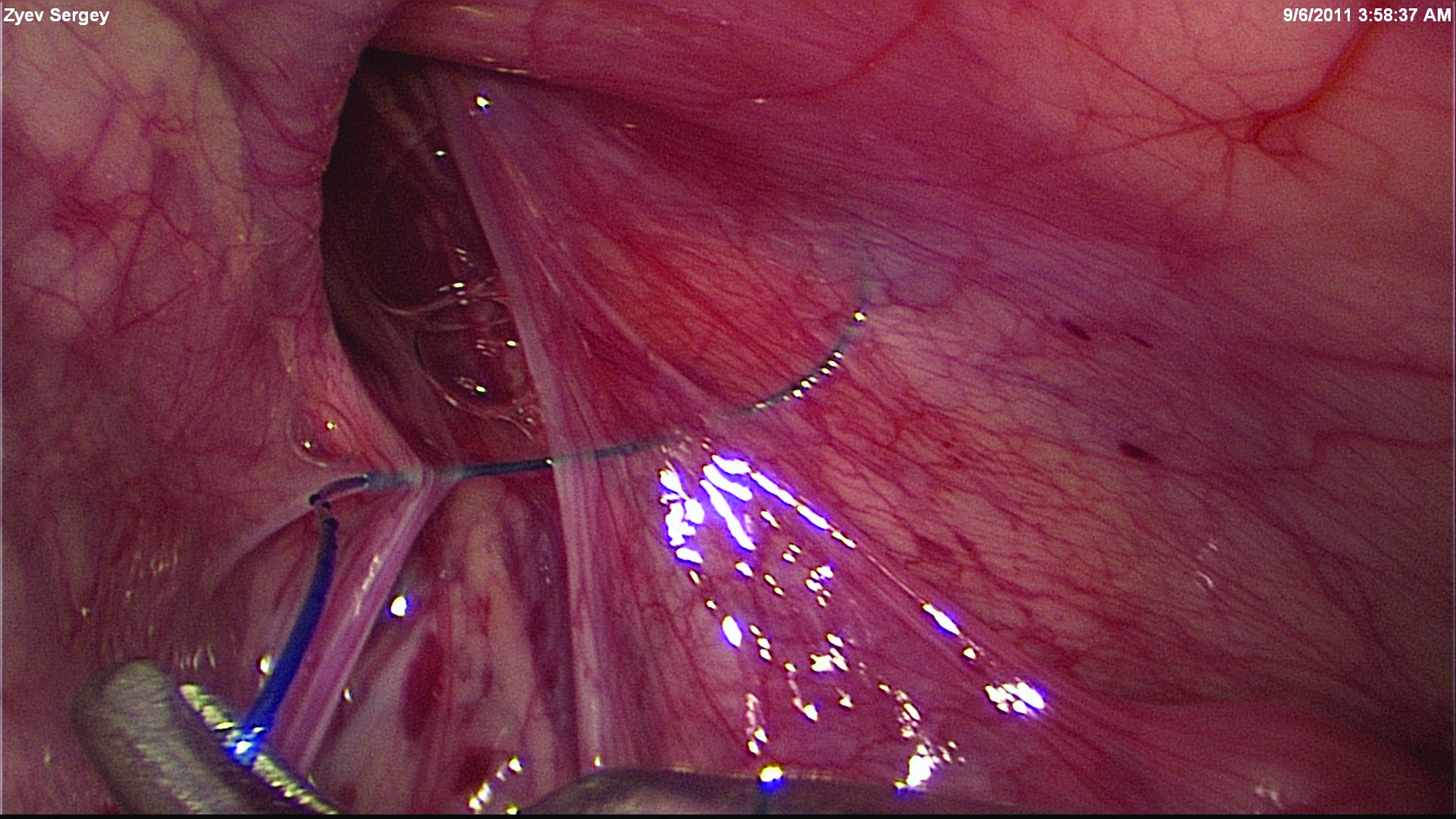
General anesthesia was accomplished using inhalation of the anesthetic (sevoflurane) with cannulation of the trachea and neuraxial blockade. The patient was positioned at the surgical table with the head of the bed inclined 15° in the Trendelenburg position. Carboperitoneum was performed with a Veress needle using flexible parameters, but starting at a flow of 2 L/minute and a pressure of 8 mm Hg. The first laparoscopic port was placed through the umbilicus, where the optical system with a diameter of 3.9 mm or 5 mm with a high-resolution camera was introduced. The Tuohy needle was inserted percutaneously in the view of the lateral edge of the abdominal ring under direct vision of the preperitoneal position (Fig. 1). Then, the end of the needle was moved under the parietal layer of the peritoneum medially with the utmost delicacy and thoroughness, especially around the elements of the spermatic cord (spermatic vessels and spermatic cord) or the round ligament of the uterus. The end of the Tuohy needle is perfectly suited for dissection of the preperitoneal space. A suture made of 2/0 or 3/0 nonabsorbable material (polypropylene [Prolene®; Ethicon, Somerville, NJ]) was threaded into the needle's lumen, before it appears at the distal end of the appliance. The needle was removed, leaving the tip of the suture in the abdominal cavity.

Position of the single port and the Tuohy needle.
The same needle with a catcher loop in the form of a “lasso” was then introduced to extract the suture. The ending of the preperitoneally placed suture was positioned through the loop, and it was extracted (Fig. 2). Under optical monitoring, the subcutaneous knotting was performed using a circular suture with simultaneous displacing of residual air from the distal portion of the hernia sac at the level of the internal inguinal ring. The laparoscopic port was removed, and suturing or gluing of laparocentesis wounds with Dermabond Advanced™ (Ethicon) glue was carried out.
Intraoperative view of the extraperitoneal ligation of the hernia sac.
The laparoscopic hernia sac ligation technique was performed using one or two ports. The additional surgical instrument—a Kelly-type grasper—was placed into the right half of the abdominal cavity slightly above the umbilicus, and it served to hold the suture at the moment of needle extraction and to put the ligature into the loop.
Postoperative complications were monitored during the hospital stay of patients, and repeated checkups were performed at 1, 3, 6, and 12 months after discharge from the pediatric hospital.
During the final stage of the investigation, two groups of patients who underwent laparoscopic treatment of inguinal hernia were compared. We analyzed patients' demographics (gender, weight, and age), operative time, and postoperative complications in the form of recurrent inguinal hernia and hydrocele formation. Intra- and postoperative parameters (operative time, duration of the hospital stay, and number of doses of the postoperative analgesia) were subjected to statistical analysis using the Mann–Whitney U test. A value of P<.05 was accepted as significant. To assess the categorical variables we used Yates's corrected chi-squared test or Fisher's exact test.
Results
Tables 1 and 2 give details of the study patients and procedures.
Group I underwent single-port laparoscopic herniorraphy; Group II underwent multiport laparoscopic herniorraphy.
By Mann–Whitney U test.
SD, standard deviation; SEM, standard error of the mean.
Group I patients underwent single-port laparoscopic herniorraphy; Group II patients underwent multiport laparoscopic herniorraphy.
By Yates's corrected chi-squared test.
By Fisher's exact test.
L, left; R, right.
We analyzed the perioperative data of neonates and infants during the first 3 months of life with a diagnosis of inguinal hernia. We found no differences between preoperative characteristics of patients of the two groups concerning the age of the patient prior to surgery, body weight at the time of surgery, gender, and affected side. The average weight and age of Group I patients were 4225 g and 49.2 days, respectively. In comparison, the average weight and age of Group II patients were 4194 g and 56.0 days, respectively (P>.05). Location of an anomaly of the inguinal canal was recorded as part of the study. Results of distribution of patients in groups according to the side of hernia localization (one-sided/bilateral) were as follows: Group I, 116/64; Group II, 53/ 27 (P=.89).
After data analysis, we determined some new facts that contradict the general concepts about the application of the single-port method. We found no differences in intra- and postoperative characteristics of patients, namely, concerning the duration of the operation, number of doses of the analgesia, and duration of the hospital stay. The average duration of the operation in Group I patients was 14.15 minutes for unilateral hernia repair and 19.36 minutes for bilateral repair. In Group II patients, the operative times were 14.06 minutes for unilateral hernia localization and 19 minutes for the bilateral defect. The number of doses of postoperative analgesia (1.19 versus 1.22) was not different between the two groups, which is indirect evidence for an identical level of postoperative pain. The number of hours for hospital stay among Group I patients (single-port method of inguinal hernia treatment) was 8.12 hours, whereas among Group II patients (multiport laparoscopic methods of inguinal hernia treatment) it was 8.27 hours (P=.12).
There were no complications in the early postoperative period after laparoscopic herniorraphy in both groups. We did not record any cases of postoperative wound infection or early recurrence of inguinal hernia.
Patient follow-up for at least 6 months after surgery demonstrated the almost complete absence of late postoperative complications except for the occurrence of development of a hydrocele in 1 Group II patient (multiport surgery) (P=.3); there was no difference in hernia recurrence, with no case in either group (P=1.0). The degree of complications was statistically the same in both groups. The single umbilical scar was invisible after a few weeks. The evidence of use of the additional instrumental laparoport was visible at repeated surveys of the abdominal wall. Long-term follow-up revealed an uneventful postoperative period and complete lack of recurrence regardless of the method used, which confirmed the reliability of the common principle of herniorraphy—preperitoneal placement of a hernial ligature.
The analysis of perioperative data demonstrated comparable parameters of minimally invasive treatment of inguinal hernias in neonates and infants during the first 3 months of life by means of single-port and multiport laparoscopic approaches. However, patients in the single-port laparoscopy group demonstrated better cosmetic results than patients in the multiport laparoscopy group, who still had visible scars.
Discussion
Modern treatment of inguinal hernia in infants is achieved by suturing the hernial sac at the level of the internal inguinal ring. There are two fundamentally different methods of laparoscopic herniorrhaphy: intracorporeal suturing of the hernia sac and preperitoneal repair of the processus vaginalis. Shheben'kov 1 from the Russian Federation was the first to perform laparoscopic herniorraphy by using a purse-string suture. Subsequently, Schier6,7 modified the intracorporeal suture and began to use the N-and Z-shaped stitches. Time has shown that the methods of extraperitoneal placement and subcutaneous knotting of hernia ligature are better because elements of the spermatic cord and the round ligament of the uterus are left absolutely intact from mechanical impact, and these methods usually provide 100% hermeticity of hernia sac closure.
Development of the minimally invasive approach for the treatment of inguinal hernia in infants is the result of an attempt at reducing the number and size of skin incisions. Use of the extracorporeal technique of ligation of the abdominal inguinal ring is an alternative. Finally, the extracorporeal technique of hernia sac ligation can be performed using a single umbilical access port.
The method of single-port access in the treatment of inguinal hernias has been described in various techniques, where the main principle is preperitoneal dissection and ligature holding without instruments. Methods known as laparoscopic percutaneous extraperitoneal closure,8,9 SEAL, 5 and percutaneous internal ring suturing 10 perform the extraperitoneal ligation of the hernia sac without insertion of an additional port. However, some of them have disadvantages. For example, the laparoscopic percutaneous extraperitoneal closure method requires the use of a special laparoscopic percutaneous extraperitoneal closure needle, which is not suitable for surgery in premature and low birth weight infants. When the percutaneous internal ring suturing method is used, closure of the full peritoneal circumference is not achieved because the part of the peritoneum over the spermatic cord and spermatic vessels is generally spared. This may predispose to recurrence and hydrocele formation. The SEAL method is one of the preferable modifications of preperitoneal hernia repair in babies; it eliminates the need for special devices, uses only an accepted Tuohy needle, and allows a full preperitoneal hernia sac closure to be realized, which helps to prevent occurrence of hydrocele. 11
Application of the SEAL method makes surgery scarless. It is the so-called stealth-surgery or keyhole incision surgery. This approach currently is especially popular in the United States and Asia, as it provides the ultimate cosmetic result and no visible signs of surgery.
Our skills in operating with a Tuohy needle under endoscopic monitoring have advanced with time and have allowed us to perform SEAL herniorrhaphy without the use of additional ports. Performing this technique with only one umbilical incision, hidden deep in the umbilical ring, allowed us to eliminate visible scars from the abdominal wall.
We placed additional instruments in circumstances like a strangulated hernia or when performing additional simultaneous procedures, such as Nissen fundoplication or pyloromyotomy. If there was a necessity to use an additional instrument, we placed it next to the optical cannula through the same incision or in the right half of the abdomen at the level of the umbilicus. 12
Currently, we have found several comparative studies of single-port and multiport laparoscopic methods in the treatment of inguinal hernia in children. One Indian study 13 compared results of the two discussed methods of endoscopic treatment of inguinal hernias and demonstrated the superiority of a single-port laparoscopic method in the form of reduced operation time (15 minutes versus 25 minutes in cases of unilateral localization). However, this study has a very serious limitation in that different techniques of herniorrhaphy—extracorporeal and intracorporeal—were used for the control group and the comparison group, respectively, which led to such discouraging results and the finding of a lack of superiority of the single-port method in treatment of inguinal hernias.
Other scientific publications evaluating the results of a single-port laparoscopic method of treatment of inguinal hernias in children have been done without comparison with other operating endoscopic methods. We present here the first comparative study of minimally invasive treatment of inguinal hernias in infants using single-port and multiport methods that is based on the same technique of herniorraphy: extracorporeal ligation of the hernia sac.
Conclusions
The advantages of laparoscopic treatment of inguinal hernias have led to minimized trauma to the hernia sac elements (spermatic cord, round ligament of the uterus) and excellent cosmetic results. Single-port herniorrhaphy demonstrates intra- and postoperative results that are comparable with those of the multiport approach. Impeccable cosmesis is the one main advantage of the single-incision laparoscopic method because the scar is hidden in the depths of the umbilical ring and is therefore completely invisible.
Footnotes
Acknowledgments
We would like to thank Oliver Muensterer, MD, PhD, from the New York Medical College for editorial assistance and support of this work.
Disclosure Statement
No competing financial interests exist.