
Abstract
Abstract
Objective:
To evaluate the feasibility of regional cramp in laparoscopic partial nephrectomy, we performed partial nephrectomy using a kidney grasper that enabled the application of ischemia to a limited region of the kidney.
Materials and Methods:
The subjects were 5 renal cell carcinoma patients. The mean tumor diameter was 15 mm. There were 2 male and 3 female patients. A transperitoneal approach was used in all cases. Following the standard procedure of laparoscopic partial resection, the hilum of the kidney was confirmed and treated to prepare for rapidly applying clamping with forceps. Tumor resection and suture were then performed under partial warm ischemia using a kidney grasper.
Results:
Surgery could be completed in 4 patients using this method. In the remaining patient, control of bleeding was considered difficult during tumor resection after applying partial ischemia, and so the procedure was switched to renal artery clamping using bulldog forceps. In the 4 patients in whom a kidney grasper was used, the mean partial warm ischemia time was 23.6 minutes (range, 23–25 minutes), and the mean blood loss was 110 mL (range, 20–260 mL).
Conclusions:
This procedure may be a useful option in ischemia for partial nephrectomy.
Background
R
Minimally invasive laparoscopic surgery has also spread, and laparoscopic partial nephrectomy is now performed. Although laparoscopic partial nephrectomy is minimally invasive, ischemia of the renal artery or renal artery and vein is applied to control bleeding in partial resection. On the other hand, to conserve the renal function, it is important to shorten the duration of ischemia. Operators are required to have advanced techniques to perform tumor resection and suturing during a limited ischemia time under laparoscopic conditions.
If ischemia can be limited to a localized region, ischemia of the main renal artery is unnecessary, which may facilitate conservation of the renal function in a secured condition. The laparoscopic Simon clamp (Aesculap AG, Tuttlingen, Germany) is a newly developed laparoscopic clamp with a standard locking handle and an open jaw diameter of 70 mm (Fig. 1). 4
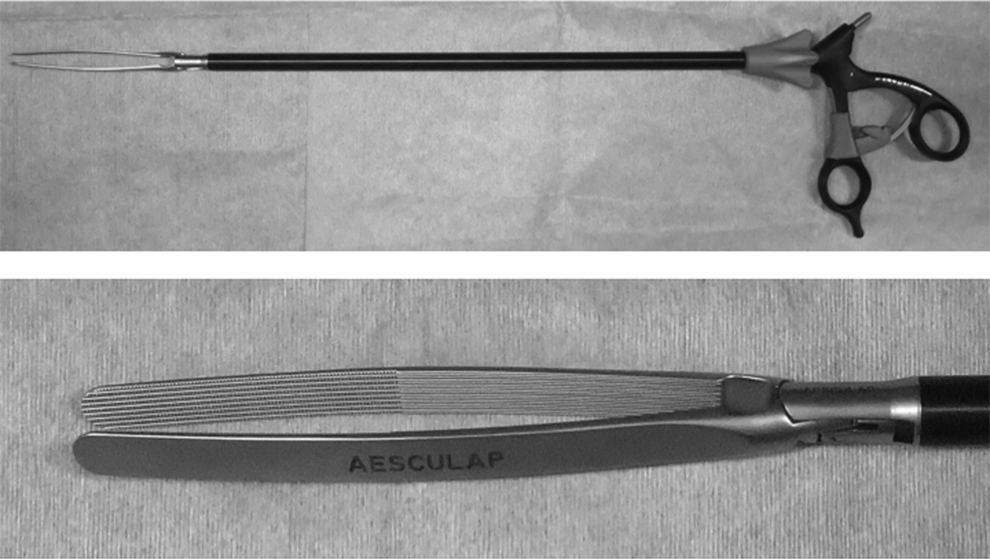
Simon renal pole clamp for selective renal clamping.
Materials and Methods
The subjects were 5 patients with small renal cell carcinoma. There were 2 male and 3 female patients, at a median age of 54 years (range, 46–63 years). The median height was 160 cm (range, 152–167 cm), and the median body mass index was 23.6 kg/m2 (range, 19–26.2 kg/m2). The affected side was right in 4 patients and left in 1 patient, and the median tumor diameter was 15 mm (range, 11–25 mm). Mass location was upper in 1 patient and lower in 4 patients. The median RENAL nephrometry score was 5 (range, 4–5).
Their outcomes were compared with those of 94 patients with a RENAL nephrometry score of 4–6 treated by laparoscopic partial nephrectomy with conventional hilum clamping between 2006 and 2013.
Procedure
After the administration of general anesthesia, the patient was fixed in the lateral decubitus position. A transperitoneal approach was used in all patients. Following the standard procedure of laparoscopic partial resection, the hilum of the kidney was confirmed and treated to prepare for rapid clamping with forceps.
Laparoscopic ultrasonography at 5–10 MHz was used to identify the tumor location and surgical margins. The incision line, which was 5 mm from the tumor margin, was marked circumferentially on the renal capsule using electorocautery monopolar scissors. After the intravenous administration of 25 mg of mannitol, the laparoscopic Simon clamp was introduced through the 12-mm port to allow for closure and placed adequately along the tumor margin.
Once the Simon clamp was closed with self-locking, it allowed rotation of the kidney for optimal tumor visualization and supported excision of the tumor.
After tumor resection using scissor forceps, hemostasis was applied to the resected stump with bipolar grasping forceps, followed by suture of the resected surface. The lesion was filled with rolled Surgicel® bolster (Ethicon, Inc., Somerville, NJ) and then sutured in Cases 2 and 3.
Resection of the tumor in regional ischemia with cold scissors in a bloodless field in Case 3 is shown in Figure 2. Computed tomography revealed a 15-mm tumor located in the lower pole of the left kidney (Fig. 2A for transverse and B for sagittal). The RENAL nephrometry score was 5. The kidney was dissected circumferentially and fully mobilized by the transperitoneal approach. The kidney grasper was introduced through the 12-mm port. The tumor with its margin was kept in regional ischemia by the kidney grasper (Fig. 2C). The tumor was dissected with cold scissors (Fig. 2D and E). After complete excision, the tumor bed was coagulated by the bipolar grasper and sutured (Fig. 2F). Rolled Surgicel bolster was then applied to the tumor bed, and parenchymal sutures were added.
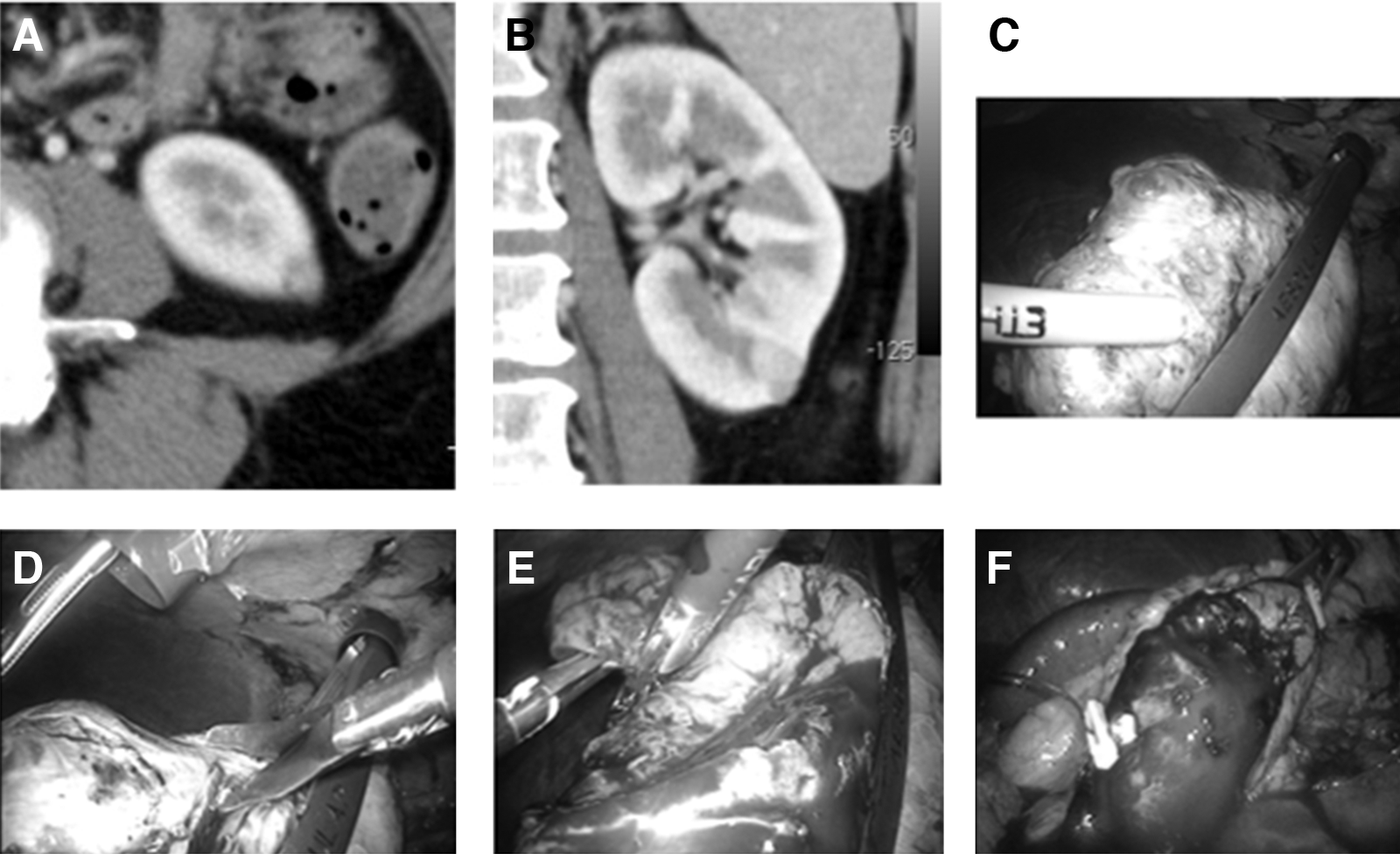
Resection of the tumor in regional ischemia with cold scissors in a bloodless field in Case 3. Computed tomography revealed a 15-mm tumor located in the lower pole of the left kidney:
Results
This procedure was used in 5 patients between June 2011 and August 2012, and surgery could be completed in 4 patients. In the first case, control of bleeding was considered difficult during tumor resection under partial ischemia, and the procedure was switched to renal artery clamping using bulldog forceps. The blood loss was 150 mL.
The results of surgery attempting the use of a kidney grasper are summarized in Table 1. The median total operative time was 220 minutes (range, 175–239 minutes), and the mean clamping time was 23.6 minutes (range, 23–26 minutes). The median blood loss was 50 mL (range, 10–260 mL), and no blood transfusion was performed. No opening of the renal pelvis was noted in any patient. No postoperative complication occurred. The histopathological diagnosis was renal cell carcinoma clear cell, and the resected stump was negative in all patients. The median serum creatinine level was 0.6 (range, 0.5–0.81) mg/dL before surgery and 0.69 (range, 0.52–0.86) mg/dL 6 months after surgery. The median estimated glomerular filtration rate was 85.01 (range, 76–97.4) mL/minute/1.73 m2 before surgery and 79.76 (range, 68.4–90) mL/minute/1.73 m2 6 months after surgery. There were no Clavien–Dindo complications at the 90-day follow-up. At a mean follow-up of 17 months no recurrence was noted.
Data are median values (range).
Peri- and postoperative parameters of clamping were compared with those of conventional clamping in our institute (Table 1). No significant differences were observed in total operative time (220 minutes versus 235 minutes), median blood loss (50 mL versus 100 mL), and serum creatinine percentage change (serum creatinine level preoperatively versus 6 months after surgery, 15% versus 9.51%).
Discussion
The concept of trifecta outcomes during robot/laparoscopic partial nephrectomy, with the three key outcomes of a negative cancer margin, minimal function decrease, and no urological complications, has been realized. 5 To minimize reduction of the renal function, it may be necessary to minimize the warm ischemia time, for which cooling, a nonischemic method, or limited range of ischemia is considered.
Sufficient cooling of the clamped renal artery and vein may be useful. This procedure is widely used in open surgery and may be applicable for laparoscopic surgery using a retroperitoneal approach, 6 but effective cooling is technically difficult for surgery through a peritoneal approach. Thus, this procedure may be not useful.
Partial ischemia procedures using various energy devices have been investigated, including an ultrasonically activated bending scalpel, 7 water-jet dissector, 8 diode laser, 9 floating-ball radiofrequency dissector, 10 microwaves, 11 and radiofrequency coagulation. 12 These are very useful for intraoperative hemostasis, and bleeding may be controlled with them. However, the margin cannot be readily decided because differentiation between normal renal tissue and the tumor is difficult. Thus, heat damage to the surrounding tissue, such as arteries, veins, and the calix, is of concern. Actually, unexpected collateral thermal damage to the surrounding structures, especially the collecting system, may cause urinoma, pelvicalyceal stenosis, and renal arteriovenous fistula.11,13,14 Because these complications have been reported, the indication may be limited to small protruding tumors.
The main problem in partial nephrectomy under ischemia is that accurate resection and suture have to be performed within a limited time, placing mental pressure on operators. With an open jaw diameter of 70 mm, the Simon clamp is novel in that it has a standard ratchet handle that can be locked into place, thereby preventing clamp sliding, while curved jaws evenly distribute a constant and uniform pressure. 4 As previously reported, partial ischemia using a kidney grasper requires no skilled laparoscopic technique, while ischemic damage of renal nephrons can be minimized, which may be the main advantage.15,16 For solitary kidney cases, damage to the renal function by surgery is a more serious concern, and it has been stated that partial ischemia is more appropriate than the method of applying complete ischemia to the hilum of the kidney. 17 We think that the applicability of partial ischemia using this procedure should be judged in sufficient consideration of the tumor location and diameter. In addition, reconsideration of the positioning of an insertion port may also be necessary. However, application may be difficult depending on the tumor location, and tumors located in the superior or inferior pole (i.e., 25-mm or smaller protruding tumors located at the superior or inferior pole) may be favorable indications. This procedure may be a useful option in ischemia for partial nephrectomy.
In our experiences, the procedure was switched to arterial ischemia in one of the 5 patients. Because the patient was the first case undergoing this procedure, we switched to arterial ischemia in the early phase, but this was considered sufficiently achievable in a later investigation.
Parenchymal regional ischemia has been attempted using other methods, and the utility was reported. Previously reported methods of laparoscopic regional ischemia have ranged from a loop tourniquet or bands to commonly used vascular clamps. Parenchymal regional ischemia has been used to avoid complete vascular occlusion during partial nephrectomy.18–21 Zero ischemia using a clip for neurosurgery has been reported. 22 There has been no report from other institutions, and this procedure may be used only at very limited facilities. This anatomical vascular microdissection of the artery first and then the tumor allows even complex tumors to be excised without hilar clamping. Compared with these, the Simon clamp may be easy to handle.
Conclusions
Selective renal parenchymal clamping during laparoscopic partial nephrectomy is feasible and an effective method to perform maximal nephron-sparing surgery without the need for warm ischemia for selective cases.
Footnotes
Disclosure Statement
No competing financial interests exist.