
Abstract
Abstract
Background:
Although laparoscopic appendectomy (LA) has been performed widely, the role of LA for complicated appendicitis remains controversial, and its role for periappendiceal abscess (PA) remains undefined. This study compared the clinical outcomes of LA and open appendectomy (OA) for PA diagnosed by radiologic investigation.
Patients and Methods:
We conducted a retrospective review of 84 patients who underwent surgery for PA diagnosed by radiologic investigation between 2010 and 2013. Twenty-five patients underwent LA, and the remaining patients underwent OA. Patient characteristics, operative outcomes, and surgical complications were compared between the two groups.
Results:
Three patients required conversion from LA to OA (12%). There were no significant differences in the overall complication (28% versus 25.4%; P=.8), wound infection (15.3% versus 4%; P=.27), stump leakage (4% versus 1.7%; P=.51), and postoperative ileus (4% versus 8.5%; P=.66) rates between the groups. The incidence of intraabdominal abscess (IAA) was significantly higher in the LA group (20% versus 3.4%; P=.02). In multivariate analysis, the risk factors for IAA were duration of drainage (P=.04) and type of operation (P=.006). The major complications rate was 2.4% in the total cohort, and the rate was significantly higher in the LA group (8% versus 0%; P=.02).
Conclusions:
For patients with PA, the rates of overall complications, wound infection, stump leakage, and postoperative ileus were similar for both procedures. However, LA resulted in a significantly higher incidence of IAA and major complications than OA.
Introduction
S
One of the main controversies surrounding LA is its application in the setting of complicated appendicitis. Some studies demonstrated that LA for complicated appendicitis may be associated with an increased rate of IAA compared with OA.9–12 Conversely, other studies proved the safety and efficacy of the laparoscopic technique for complicated appendicitis.13–19 However, there are few series that discussed the use of the laparoscopic approach for periappendiceal abscess (PA).
Although our study is small, it describes a specific subgroup of acute appendicitis (only PA diagnosed by radiologic investigation). The aim of this study was to compare the clinical outcomes of LA versus OA for PA diagnosed by radiologic investigation.
Patients and Methods
Study populations
A retrospective chart review was performed for all 1525 patients who underwent surgery for appendicitis in Eulji General Hospital (Seoul, South Korea) between January 2010 and December 2013 (Fig. 1). First, we selected 89 patients who were diagnosed with PA based on radiologic findings. Ultrasonography (US) or computed tomography (CT) was used to confirm the presence of PA. US or CT scans were then re-reviewed by a single radiologist who was blinded to the patient outcome. Of the 1525 patients, only 39 patients (2.5%) did not undergo a radiologic investigation. Finally, PA was confirmed by the operative and pathologic findings. Of the 89 selected patients, 5 patients were excluded from this study because of various reasons (e.g., tumor identified by pathology, no abscess identified intraoperatively, and use of another surgical procedure). In total, 84 patients were enrolled. We retrospectively analyzed the clinical records of these patients who had undergone appendectomy for PA. The patients were divided into two groups: LA or OA. Twenty-five patients underwent LA, and the remaining 59 patients underwent OA. Three of the 25 patients were converted to the open procedure after laparoscopy. These patients were included in the LA group.
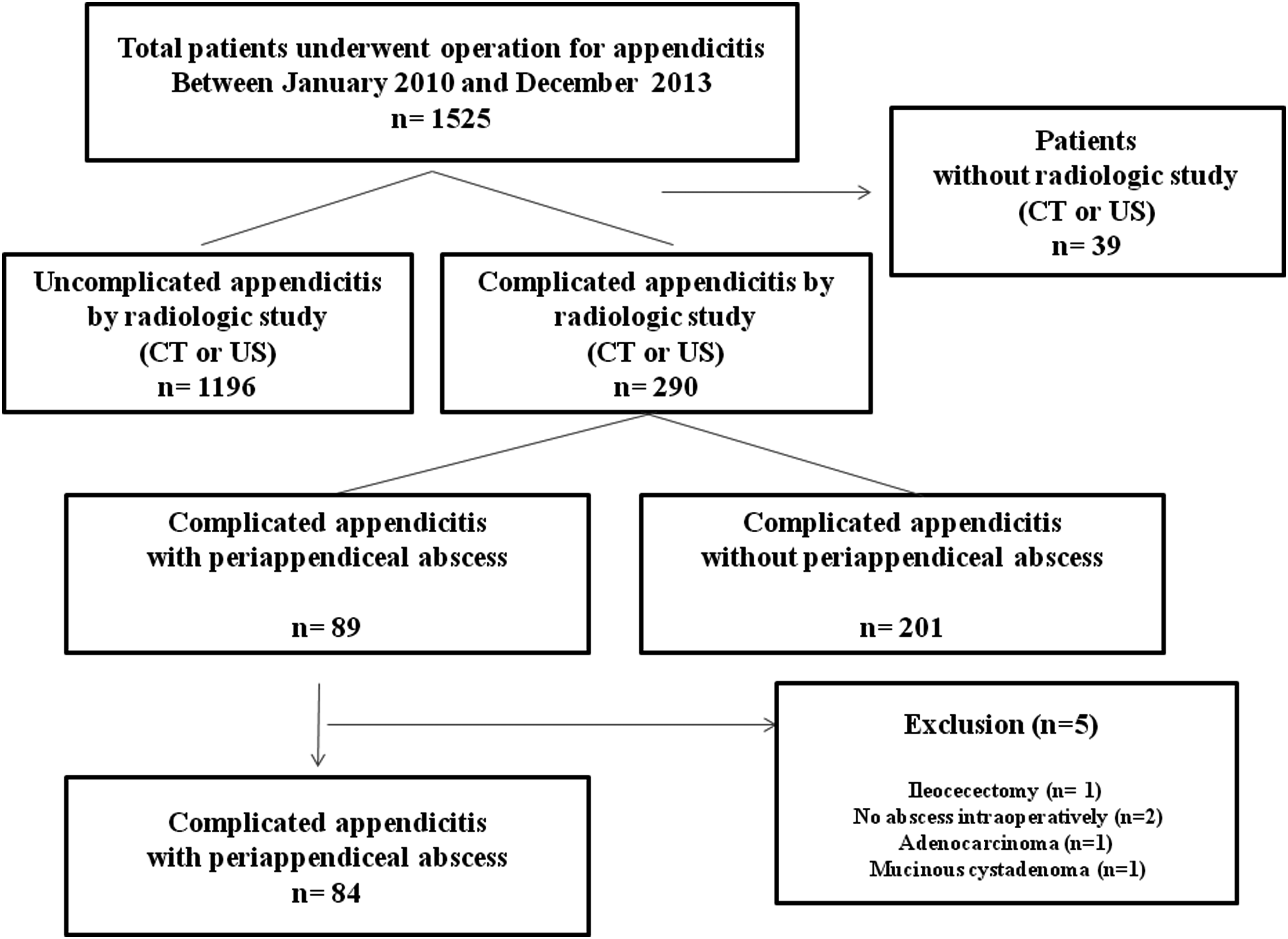
Flowchart of patient selection. CT, computed tomography; US, ultrasonography.
Data collection
Demographics and clinical characteristics (age, sex, American Society of Anesthesiologists class, body mass index, comorbidity, onset of symptom, body temperature, white blood cell count, preoperative C-reactive protein score, duration and type of antibiotic treatment, and size of the PA) were evaluated. Operative outcomes (conversion to open procedure, operative time, type and duration of drainage, time to oral intake, and length of hospital stay) were assessed. Surgical complications were defined as complications occurring within 30 days after surgery. Wound infection, stump leakage, IAA, and postoperative ileus were assessed as surgical complications. Wound infection was defined as a superficial and deep surgical-site infection according to the surgical-site infection criteria of the U.S. Centers for Disease Control and Prevention. 20 IAA was defined as intraabdominal fluid collection as determined by radiologic investigation with systemic or localized signs of infection. Surgical complications were reclassified using the Clavien–Dindo classification. 21 The total numbers of postoperative complications were counted for all cases with morbidity. Major complications were defined as those with a grade of III and higher on the Clavien–Dindo classification. These parameters were compared between the two groups.
The decision regarding whether to attempt LA was based on the attending surgeon's preference. All LAs were performed by six surgeons with sufficient experience in laparoscopic surgery. Two other surgeons, in addition to the aforementioned six surgeons, were involved in OA. Of the two surgeons, only one surgeon did not have sufficient experience in laparoscopic surgery. This study was approved by the Institutional Review Board of Eulji General Hospital.
Standardized care protocol
We have a clear policy about the management of PA. Conservative treatment (such as percutaneous drainage and intravenous antibiotics) for PA was not initially performed in our institution. All patients underwent definitive surgery, and a standard regimen of intravenous antibiotics (a second-generation cephalosporin and metronidazole) was delivered before surgery. Postoperatively, antibiotic treatment was continued until the white blood cell count was within normal limits and the temperature was less than 37.9°C for 48 hours. Oral intake was started postoperatively as soon the patient could tolerate it. Patients were discharged once bowel function and oral intake were adequate.
Surgical technique of LA or OA for PA
OA was performed through a McBurney incision. Dissection, vessel ligation, and irrigation were performed via conventional methods. A purse-string suture was not used for stump closure, and pus drainage was performed by incision and suction. Closed or open drains were placed in the encountered abscess cavity. All appendix specimens were sent for pathologic examination.
LA was performed with the three-trocar approach (two 5-mm, one 10-mm). Pus drainage was performed by suction. The mesoappendix was dissected using a Maryland dissector via monopolar electrocautery. The appendiceal artery was ligated with an Endo-clip. Endo-loops (Ethicon, Somerville, NJ) were usually used for stump closure. The Endo GIA™ (Covidien, Mansfield, MA) stapling device was used for 1 patient with a friable stump. All specimens were removed in an endo-bag. Closed or open drains were placed in the encountered abscess cavity. In 4 patients, appendix specimens were not sent for pathologic examinations because of severe necrotic change.
Statistical analysis
Data were analyzed using the SPSS statistical program (Statistical Product and Service Solution 18 for Windows; SPSS Inc., Chicago, IL). Student's t test was used for continuous variables, whereas categorical variables were analyzed using the chi-squared test or Fisher's exact test. Converted cases were considered on an intention-to-treat basis. Factors that might affect postoperative IAA were evaluated by univariate and multivariate logistic regression analysis. A P value of <.05 was considered statistically significant.
Results
Demographic and clinical characteristics
Table 1 directly compares the demographics and clinical characteristics of the two groups. There were no significant differences in the distributions of age, sex, American Society of Anesthesiologists class, body mass index, duration and type of antibiotic treatment, and comorbidity between the groups. Although there was no significant difference in white blood cell counts and C-reactive protein scores, there were significant differences in the onset of symptoms and body temperature.
Data are mean±standard deviation values.
Coronary heart disease, history of myocardial infarction, valvular heart disease, or congestive heart failure.
Chronic obstructive pulmonary disease, asthma, emphysema, or pulmonary hypertension.
Hepatitis or liver cirrhosis.
Renal failure.
ASA, American Society of Anesthesiologists; BMI, body mass index; CRP, C-reactive protein; LA, laparoscopic appendectomy; OA, open appendectomy; WBC, white blood cell.
Operative outcomes (Table 2)
In the LA group, 3 patients required conversion to an open procedure (12%). The reason of conversion was difficult dissection in all patients. There was no significant difference in the operative time, time to oral intake, and length of hospital stay between the two groups. Although there was no significant difference in the duration of drainage, the type of drainage was significantly different between the groups (closed drain: 92% in the LA group versus 66.1% in the OA group; P=.02). The length of hospital stay (in days) was shorter for the LA group, but this difference was not significant (P=.17).
Data are mean±standard deviation values unless indicated otherwise.
LA, laparoscopic appendectomy; OA, open appendectomy.
Surgical complications
Among the total cohort (n=84), 22 patients experienced 25 postoperative complications after appendectomy, and there were no mortalities (Table 3). Their surgical morbidity and mortality rates were 26.2% and 0%, respectively. The most common complication was wound infection (n=10, 11.9%). Other complications included IAA (n=7, 8.3%), postoperative ileus (n=6, 7.1%), and stump leakage (n=2, 2.4%).
Data are number (%) unless indicated otherwise.
IAA, intra-abdominal abscess; LA, laparoscopic appendectomy; OA, open appendectomy.
There was no significant difference in the overall complication rates (28% in the LA group versus 25.4% in the OA group; P=.8). Although there was a reduced tendency for wound infection in the LA group compared with the OA group, this difference was not statistically significant (15.3% versus 4%; P=.27). There were also no significant differences in the stump leakage (4% versus 1.7%; P=.51) and postoperative ileus (4% versus 8.5%; P=.66) rates between the LA and OA groups. The incidence of IAA was significantly higher in the LA group than in the OA group (20% versus 3.4%; P=.02). All patients with IAA were treated successfully with antibiotics or US-guided percutaneous drainage when the collection was encapsulated. Among the 5 patients who developed IAA after LA, 2 were treated with US-guided percutaneous drainage, and 3 were managed with antibiotics alone. Both patients who developed IAA after OA were managed conservatively with antibiotics alone. No patients required re-exploration for any of the complications.
The rate of major complications was 2.4% in the total cohort (2 patients with IAA in only the LA group). There were significant differences in the major complications rate between the LA and OA groups (8% versus 0%; P=.02). Re-admission occurred only in 1 patient in the LA group. The reason for re-admission was IAA.
Risk factors of postoperative intraabdominal abscess
In univariate analysis, risk factors that influenced postoperative IAA were the type of drainage, duration of drainage, and type of operation (Table 4). Age, sex, American Society of Anesthesiologists score, body mass index, onset of symptom, white blood cell count, C-reactive protein score, and operative time were not risk factors for IAA in univariate analysis. In multivariate analysis, the risk factors for IAA were duration of drainage (P=.04, odds ratio=20.844) and type of operation (P=.006, odds ratio=24.361).
ASA, American Society of Anesthesiologists; BMI, body mass index; CI, confidence interval; CRP, C-reactive protein, IAA, intraabdominal abscess; LA, laparoscopic appendectomy; OA, open appendectomy; OR, odds ratio; WBC, white blood cell.
Discussion
In 2001, Wullstein et al. 18 first reported a retrospective study establishing the objective advantages of LA for complicated appendicitis. Since that study, many studies have been published on the use of LA for complicated appendicitis.6,11,13–19,22 These studies revealed that LA for complicated appendicitis is safe and offers patients faster recovery with a lower risk of infectious complications. However, the benefits of LA in the management of complicated appendicitis are controversial, especially regarding the rate of postoperative complications, such as IAA.11,12
Previous studies displayed some variation in the definition of complicated appendicitis. Complicated appendicitis includes various disease entities, ranging from gangrenous change to diffuse peritonitis with abscess formation. Most studies defined complicated appendicitis as a perforated appendicitis with or without abscess formation. Many studies include histological gangrenous appendicitis in complicated appendicitis because it is difficult clinically to distinguish between a perforated and a nonperforated gangrenous appendicitis. Markides et al. 22 also mentioned that the case definition for complicated appendicitis is one of the problems in the appraisal of studies in their meta-analysis.
To avoid this problem, we confined our study population to patients with PA in a preoperative radiologic investigation. We excluded the presence of gangrene, perforation, or micro-abscess confirmed only by pathologic examination. The shortcoming of our setting was that patients with perforation that cannot be diagnosed by radiologic investigation were excluded. Although this shortcoming can create another selection bias, this setting can provide an objective comparison between LA and OA in terms of the severity of complicated appendicitis. In our hospital, preoperative radiologic studies (US or CT) were routinely performed with a clinical history and physical examination in patients with suspected appendicitis. Because of this policy, 1486 (97.5%) of 1525 patients underwent radiologic studies.
The principal finding of this study was that the incidence of IAA in the LA group was higher than that in the OA group among patients with PA. This significantly higher incidence of IAA also resulted in a higher rate of major complications in the LA group. Some retrospective studies similarly reported that the incidence of IAA was higher in the LA group than in the OA group among patients with complicated appendicitis.11,12 However, many retrospective studies and a meta‐analysis identified no significant difference in the incidence of IAA between the two groups.13–18,22,23 The great majority of previous studies did not classify patients in terms of the presence of an abscess. Park et al. 23 classified patients into two subgroups in their study: (1) complicated appendicitis without abscess and (2) complicated appendicitis with abscess. They concluded that LA may be a safe, effective treatment for complicated appendicitis, even in the presence of abscess. Their results differ from our results in that there was significant difference in the incidence of IAA between the two groups. However, the definition of complicated appendicitis with abscess was based on radiologic, operative, and pathologic findings in their study. Patents with micro-abscesses confirmed only by pathologic examination might have also been included in the complicated appendicitis with abscess group. This point might be one cause of the differences between the study results.
In our study, the higher incidence of IAA in the LA group may have been due to the difference of peritoneal irrigation. Irrigation fluid may cause contamination in clean areas of the peritoneal cavity. Surgeons performing LA tended to apply irrigation more liberally, and this could partially be associated with the higher incidence of postoperative IAA in the LA group. The debate over the efficacy of peritoneal irrigation has long remained unsettled. Despite a multitude of studies24,25 attempting to address this issue, the debate has continued, with surgeons either advocating or condemning irrigation.
Open drains were more commonly used in the OA group in our study. The type of drainage might be also associated with the difference in the incidence of IAA between the two groups. However, the type of drainage was not a significant risk factor for IAA in univariate and multivariate analyses.
This study uncovered no significant differences in the rates of overall complications, stump leakage, and postoperative ileus. The rate of wound infection was higher in the LA group than in the OA group, but the difference did not reach statistical significance. The lack of a significant difference is likely related to the insufficient sample size of the study. Most previous studies demonstrated that LA significantly improved the wound infection rate in patients with complicated appendicitis.13–18 On the contrary, some studies concluded that there was no significant difference in the wound infection rate between the OA and LA groups.11,19 However, the great majority of studies agree that LA is associated with a reduced rate of wound infection.
There is controversy over the operative time of laparoscopy and open surgery for complicated appendicitis. Many studies suggested that there is no significant statistical difference in the operative time between the techniques.13,14,19 Our study also found no significant difference, although the operative time tended to be longer in the LA group.
LA can serve as a diagnostic and therapeutic tool in patients with suspected appendicitis. However, LA did not have great diagnostic significance for definite PA diagnosed by preoperative radiologic investigation. In fact, appendectomy was positive in all 89 patients who were diagnosed with PA based on radiologic findings (Fig. 1). Only 4 patients (4.5%) underwent appendectomy due to other pathology. Two patients (2.2%) underwent OAs for uncomplicated appendicitis. Two patients (2.2%) were finally confirmed to have appendiceal tumors. In patients with definite PA, the value of LA must be assessed only in terms of the therapeutic effect. The postoperative complication rate is an important parameter, especially considering the therapeutic effect after benign surgery.
In our study, we attempted to clarify whether clinical outcomes would be similar between the two procedures in terms of the postoperative complication rate. Because postoperative complications are usually considered an assessment of a procedure's safety, this is an inevitable question to justify the adoption of the laparoscopic approach for PA. According to our results, the answer is no. This is because the rate of major complications and the incidence of IAA were significantly higher in the LA group than in the OA group.
No firm conclusions can be drawn concerning whether LA is a safe procedure for patients with PA, as few series discussed the laparoscopic approach for PA. In addition, the only study that investigated the question had a retrospective design. 23 Our study was also retrospectively designed, indicating that our study cannot be free from the fundamental limitation of retrospective analysis.
Our study included several limitations that were not controlled evenly between the groups. The first limitation is patient-related factors, including demographic and clinical characteristics. Baseline clinical differences between the two groups were included the onset of symptoms, body temperature, and type of drainage. However, none of these variables was a significant risk factor for postoperative IAA in univariate analysis. The duration of drainage and the type of operation were significant risk factors for IAA in multivariate analysis. The second limitation was surgeon-related factors related to his or her preference concerning the surgical approach for PA. The lack of defined selection criteria for the operative approach for PA is a drawback of our study. The unclear selection criteria resulted in decisions based on the surgeons' preferences. This may be an important selection bias. Therefore, biases in relation to the selection of the surgical approach may have affected the results. The third limitation is the difference in surgical experience. Figure 2 shows the percentage of procedures performed for patients with PA each year. Until 2011, LA rarely performed in patients with PA. Since 2012, LA has been increasingly performed. The level of surgical experience and the learning curve are important factors that can affect outcomes. Although the six surgeons performing LA had sufficient experience with laparoscopic surgery, they are clearly at the start of the learning curve in performing LA for patients with PA. This could result in a higher rate of IAA in the LA group. The fourth limitation was the relatively small sample size. Previous studies indicated that more than 2000 patients with perforated appendicitis should be enrolled to achieve statistical significance in analyses of the IAA rate.26,27 However, this is an impractical task for a single-institution study.
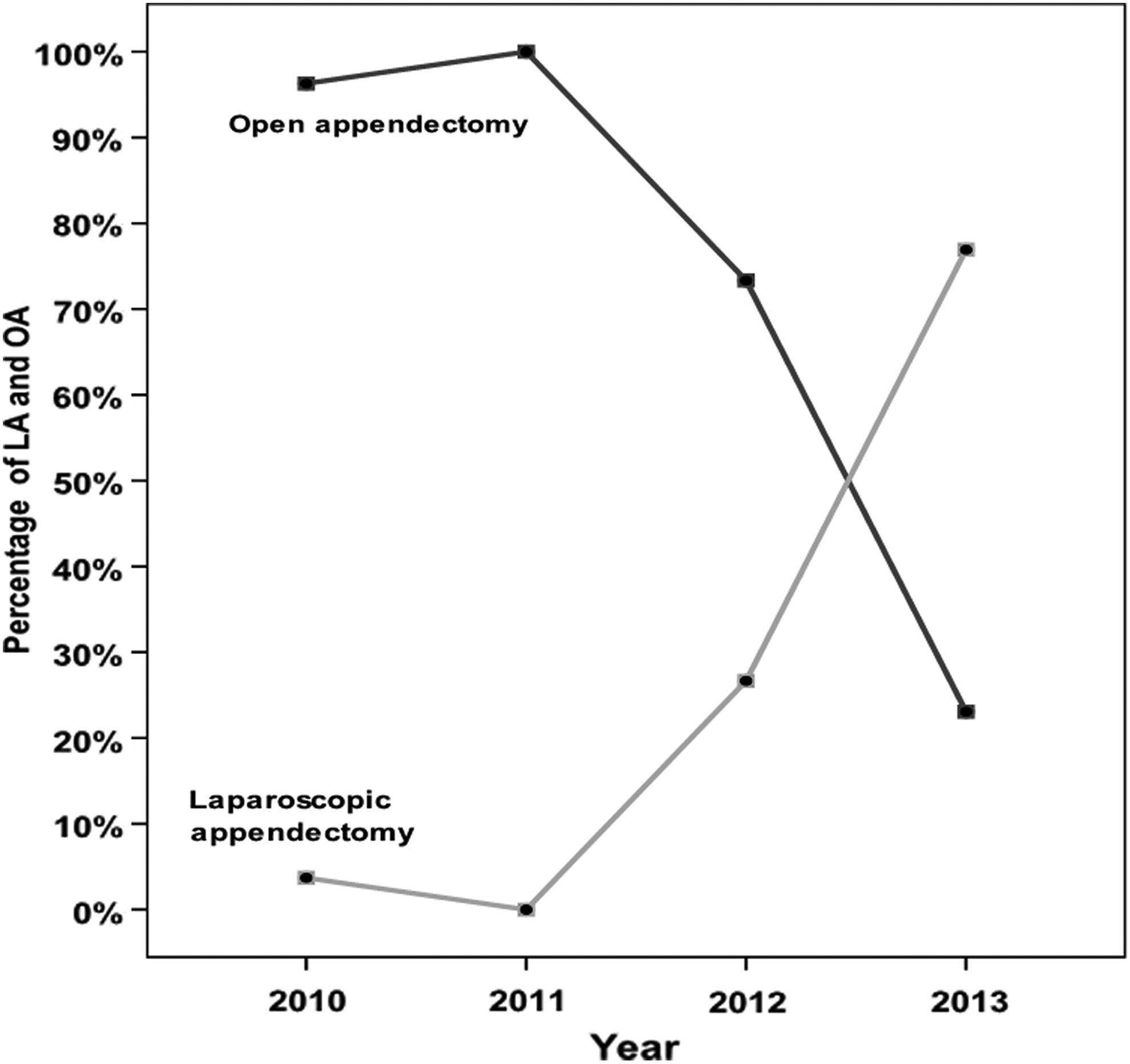
Percentages of patients with periappendiceal abscess (n=84) who underwent laparoscopic and open procedures performed each year. LA, laparoscopic appendectomy; OA, open appendectomy.
In summary, our study identified no significant difference in overall complication rates between LA and OA. However, LA for patients with PA resulted in a significantly higher incidence of IAA and major complications. The risk of IAA formation appears to be associated with the type of surgical approach. Because of the limitations of retrospective analyses, no firm conclusions can be drawn concerning the safety of LA for patients with PA. Future large-scale, prospective, randomized controlled studies are needed to confirm these results.
Footnotes
Disclosure Statement
No competing financial interests exist.