
Abstract
Abstract
Background:
Laparoscopic cholecystectomy (LC) has been performed clinically for more than 20 years. However, the incidence of bile duct injury (BDI) remains high despite attempts to prevent and reduce it. The aim of this study was to use an intraoperative unfavorable factors ratings system to identify unfavorable intraoperative factors and evaluate the effectiveness of application of the system in reducing BDI during LC.
Patients and Methods:
Between January 2009 and December 2010, 780 patients who underwent LC were reviewed retrospectively, including 384 LC patients without graded treatment of intraoperative unfavorable factors (GTIUF) during 2009 and 396 LC patients with routine GTIUF during 2010.
Results:
BDI was decreased significantly after routine GTIUF (5 cases without GTIUF versus 0 cases with routine GTIUF; P=.029). There was no significant difference in postoperative morbidity and mortality between the two groups. The mean operation duration of the routine GTIUF group was prolonged significantly (P<.0001). Laparoscopic cholecystitis grading, GTIUF, and doctor's experience were important factors affecting the duration of operation (P<.0001, P<.0001, and P<.0001, respectively).
Conclusions:
GTIUF is an effective method that emphasizes identification of the course of the extrahepatic bile duct and reduces the occurrence of BDI, especially for inexperienced operators.
Introduction
L
Apart from the LC “learning curve,” important risk factors contributing to BDI in LC include acute cholecystitis, acute biliary pancreatitis, bleeding in the triangle of Calot, a severely scarred or shrunken gallbladder, and large impacted gallstones in Hartmann's pouch.10,11 In addition, abnormal biliary anatomy is a common reason for BDI after LC.12,13 Other risk factors include male sex, history of abdominal surgery, gallbladder atrophy, cirrhosis, and long surgical duration (longer than 150 minutes).13–17 There are few reports describing strategies to reduce these risk factors in preventing BDI.
Factors that may cause BDI during LC are called intraoperative unfavorable factors (IUF). The purpose of the present study was to validate the effect of graded treatment of IUF (GTIUF) in preventing BDI during LC and its influence on surgical duration.
Patients and Methods
General data
Among 797 patients who underwent laparoscopic biliary surgery in our hospital from January 2009 to December 2010, 780 were included, after excluding 17 in whom surgery other than LC was performed. During 2009, 384 cases of LC were performed without GTIUF by four surgeons whose experience was 15 years, 7 years, 3 years, and less than 1 year, respectively. GTIUF for LC was introduced beginning January 1, 2010 for the purpose of decreasing BDI and as a guide for management of unexpected and unfavorable intraoperative events. By the end of 2010, 396 LCs had been performed using routine GTIUF (Table 1) by five surgeons whose experience was 16, 8, and 4 years and for two less than 1 year, respectively. The cases were divided into those done by inexperienced doctors (<100 LC operations) and those done by experienced doctors (>100 LC operations). Intraoperative cholangiography was performed by a radiological specialist only when needed. Data were collected on age, sex, operative indications, laparoscopic cholecystitis grade, IUF ratings, and complications. The study was approved by the Research Ethics Committee of Shanghai Jiao Tong University Affiliated Sixth People's Hospital (Shanghai, China).
Other benign processes including chronic cholecystitis and adenomyomatosis, which require whole biopsy of the gallbladder for suspected malignancy.
GTIUF, graded treatment of intraoperative unfavorable factors; SD, standard deviation.
Data analysis
The operation duration, the number of intraoperative conversions to open surgery, postoperative BDI, and other postoperative complications of all LC cases were reviewed retrospectively, and the results were analyzed with SPSS version 15.0 software (SPSS, Inc., Chicago, IL) using Student's t test and chi-squared test. P<.05 was considered statistically significant.
Laparoscopic cholecystitis grading
According to laparoscopic cholecystitis grading (LCG), the severity of cholecystitis was classified into four grades. 18 As inflammation around the gallbladder and the laparoscopic surgical field are also factors affecting the difficulty of LC, the severity of cholecystitis was classified into four grades (G0–G3) according to preoperative macroscopic findings: G0, mild adhesion without inflammation of the gallbladder; G1, inflammatory fibrous adhesion without acute inflammation; G2, severe inflammatory thickening of the gallbladder with mild adhesion; and G3, lack of visualization of the gallbladder due to close inflammatory adhesion to the surrounding tissue.
IUF rating
IUF ratings were also classified into four categories (R0–R3) according to the total points of the four IUFs: adhesions around the gallbladder (score 0–3), difficulty in detaching the triangle of Calot (score 0–3), anatomic abnormality in the extrahepatic bile duct (score 0–3), and oozing or bleeding in the surgical field (score 0–3) (Table 2). Late-stage IUF were assessed as R0, R1, R2, and R3 (GTIUF stage) as follows: R0, total points <3; R1, 3≤total points<6; R2, 6≤total points<9; and R3, total points ≥9.
Management of rated IUF
In R0 cases, LC was performed according to the requirements of “the critical view of safety.” 19
In R1 cases, LC was performed according to the requirements of the above-mentioned three aspects first, and then a discussion was held with the assistant. When there was doubt about the structure of the bile duct and gallbladder artery or about the technique to be performed and its safety, help was obtained from experienced laparoscopic surgeons before proceeding with the procedure.
In R2 cases, LC was performed as described above. If there was doubt about the structure of the bile duct and gallbladder artery, intraoperative cholangiography was performed by a radiological specialist who interpreted the cholangiogram together with all operators, and experienced laparoscopic surgeons were consulted before proceeding with the procedure.
In R3 cases, LC was performed as described above. In case doubts remained, LC was converted to open surgery.
Results
During 2009, 92.4% of LC procedures were performed by experienced doctors without using GTIUF (early stage), and in 2010, 34.3% of LCs were performed by inexperienced doctors using GTIUF (late stage). There was no significant difference in anatomic alteration (2.6% versus 4.3%; P=.137) or LCG (P=.095) between the two groups. The only difference was that there were more cases of G2 in the early stage and more cases of G3 in the late stage. In addition, there were significantly more cases of conversion to open surgery in the late stage compared with those in the early stage (P=.043). BDI occurred in 5 cases in the early stage, whereas no BDI occurred in the late stage. The mean operation duration in the late stage was increased by about 14 minutes. The operation duration for senior doctors was significantly shorter than that for junior doctors (P<.0001), and there was a significant difference in intraoperative blood loss between cases done by the two groups of doctors (P=.045) (Table 3).
Data are mean±standard deviation values, n (%), or n as indicated.
GTIUF, graded treatment of intraoperative unfavorable factors.
The operation duration for the late stage using GTIUF was longer than that in the early stage without using GTIUF. Analysis of factors affecting the operation duration in the late stage showed that LCG, GTIUF, and doctor's surgical experience were important factors affecting the operation duration (P<.0001, P<.0001, and P<.0001, respectively) (Table 4). Analysis of the three factors showed that high LCG, inexperience of the doctor, and GTIUF all increased the operation duration (Fig. 1).
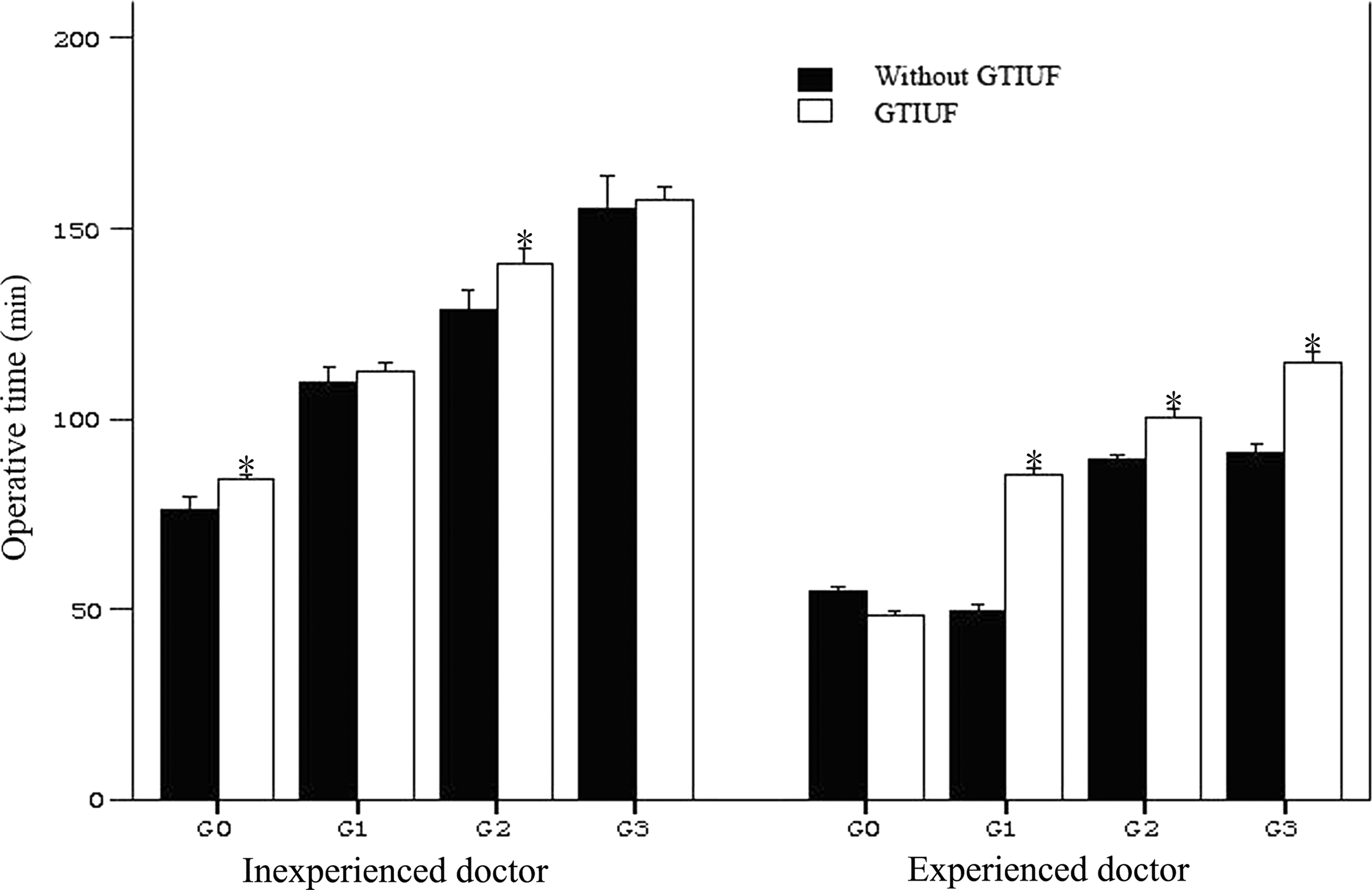
Correlations of the operation duration with laparoscopic cholecystitis grading and the operator. In an analysis of covariance, laparoscopic cholecystitis grading, graded treatment of intraoperative unfavorable factors (GTIUF), and doctor's surgical experience were significant factors affecting operation duration (P<.0001, P<.0001, and P<.0001, respectively). Operation time with GTIUF was significantly increased for junior surgeons (all P<.01). Operation time for junior surgeons by the laparoscopic cholecystitis grading stage was significantly increased (*P<.01), regardless of laparoscopic cholecystitis grading, thus requiring approximately double the time in comparison with that of senior surgeons.
GTIUF, graded treatment of intraoperative unfavorable factors; LCG, laparoscopic cholecystitis grading.
Although more operations were performed by less experienced doctors later, there was no significant difference in rates of postoperative complications, the re-operation, and operative mortality between the two groups. No BDI occurred in the late stage (P=.029). In addition, the mean hospital stay was shorter, and no bile duct stenosis occurred (Table 5).
Data are n (%) or mean±standard deviation value as indicated.
Of the 3 patients who died, 2 died of postoperative myocardial infarction, and the other died of postoperative pulmonary infection. Surgery was smooth in all three cases without bile duct injury (BDI).
GTIUF, graded treatment of intraoperative unfavorable factors.
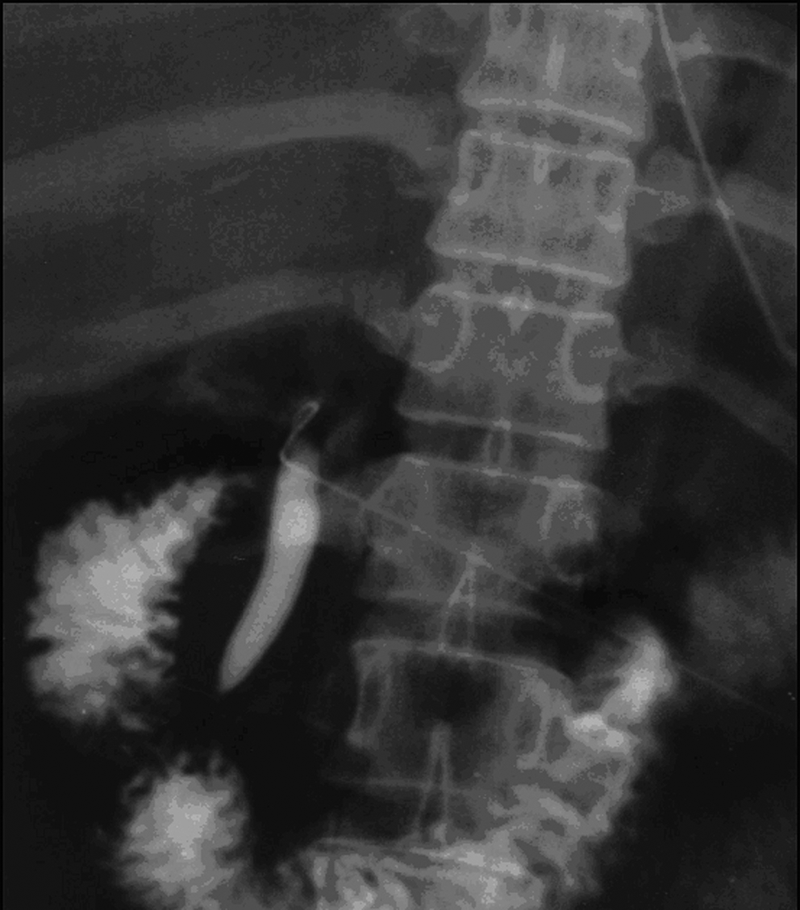
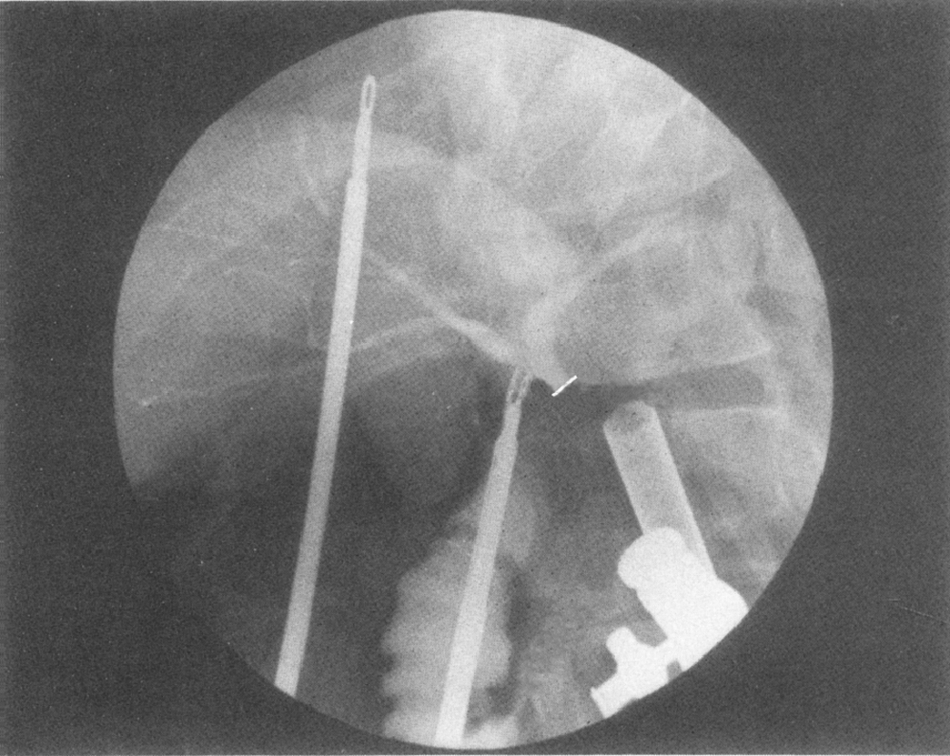
All the cases of early-stage BDI and cases of anatomical duct variants were evaluated by cholangiography during the operation and managed surgically. In the first case of BDI, the common bile duct was mistaken for the cystic duct and transected because of alteration in the cystic duct course (Fig. 2). In the second case of BDI, the common bile duct was mistaken for the cystic duct and transected because of overstretching of the gallbladder (Fig. 3). The third case of BDI was due to anatomic alteration of the cystic duct running into the right hepatic duct (Fig. 4). The fourth case of BDI was a patient with severe cholecystitis, in whom the common hepatic duct was burned during electrocoagulation in the triangle of Calot, causing bile leakage (Fig. 5). Another case of BDI was converted to open surgery for suturing a tear of the conjunction of the cystic duct with the common bile duct due to a severe inflammatory adhesion (Fig. 6 and Table 6).

The common bile duct was mistaken for the cystic duct and transected because of alteration in the cystic duct course.
The common bile duct was mistaken for the cystic duct and transected because of overstretching of the gallbladder.
The common bile duct was transected because of anatomic alteration of the cystic duct running into the right hepatic duct.

The common hepatic duct was burned during electrocoagulation in the triangle of Calot, causing bile leakage.

The common bile duct injury was due to a tear of the conjunction of the cystic duct with the common bile duct.
The cystic duct passes behind the common bile duct and enters from the left wall.
The cystic duct runs directly into the right hepatic duct.
F, female; LCG, laparoscopic cholecystitis grading; M, male.
Discussion
Although LC has been used clinically for more than 20 years, the incidence of BDI remains high. The exact reasons remain unclear. 20
Reduce intraoperative BDI by selecting an appropriate LC strategy
After much investigation and discussion, the “critical view of safety” has been generally accepted as a good method of avoiding BDI.19,21 This technique emphasizes extensive isolation within the triangle of Calot without anatomizing the common bile duct, gallbladder ampulla, and gallbladder plate. Only two structures (the cystic duct and the gallbladder artery) are seen entering the gallbladder after the fat and fibrous tissues are removed. This significantly increases the safety of the surgical procedure in managing the gallbladder artery and the cystic duct.20,22 However, although “the critical view of safety” technique has been applied for years, the incidence of BDI is still higher than that of open surgery. 1
Reduce BDI by intensifying intraoperative visualization of the extrahepatic bile duct during LC
Misjudgment is one of the important factors contributing to BDI. The most common misjudgment is mistaking the common bile duct for the cystic duct, causing BDI and classic injury in LC. 23
Although intraoperative ultrasound can reduce the occurrence of BDI, it requires specialized training. 24 Dissection of the triangle of Calot is a delicate procedure, and BDI is still likely to occur even when the structure of the extrahepatic bile duct is clearly displayed by intraoperative ultrasound. 17 Some researchers have used duodenoscopy as a cold light source to illuminate the extrahepatic bile duct and delineate its course in an attempt to reduce BDI. However, this manipulation is complex, and its effectiveness in reducing BDI has not been conclusive. 25
The incidence of BDI in LC remains higher than that in open surgery despite the use of the “critical view of safety,” intraoperative cholangiography, and intraoperative ultrasound. However, some researchers found that a cautious and continuous learning attitude of the doctor, sophisticated surgical techniques, and a low threshold for conversion to open surgery are beneficial to the prevention of BDI.10,14 Nordin et al. 20 have reported that BDI is avoidable in LC as long as factors contributing to BDI are compared and analyzed carefully.
GTIUF decreased the incidence of BDI, especially for junior doctors, because they could make an initial judgment about IUF and then decide on appropriate strategies with the help of intraoperative cholangiography and consultation from senior endoscopists. As a result, GTIUF should be useful for assisting junior doctors surmount the “learning curve” of LC.
In summary, cholecystectomy, especially LC, is a high-risk surgical procedure. GTIUF is an effective method of preventing BDI during LC in that it helps identify the course of the extrahepatic bile duct and prevents intraoperative errors, especially for inexperienced operators.
Footnotes
Acknowledgments
We acknowledge Zhi-Li Yang, MD, PhD, for helpful discussions.
Disclosure Statement
No competing financial interests exist.