
Abstract
Abstract
Background:
Although laparoscopic liver resection has been gradually adopted as an attractive option, it is still not indicated for large hepatocellular carcinoma (HCC). The aim of this study is to assess the feasibility of laparoscopic liver resection for large HCCs.
Subjects and Methods:
A retrospective comparative study between 20 patients with HCC ≥5 cm and 103 patients with HCC <5 cm who underwent laparoscopic liver resection for hepatocelullar carcinoma from September 2003 until December 2011 at Seoul National University Bundang Hospital was performed.
Results:
In total, 95 men and 28 women with a mean age of 56.92±11.28 years were enrolled in this study. There were no significant differences in preoperative patient demographics and tumor characteristics between the two groups. A major operation was performed more frequently in the large tumor group than in the small tumor group. On the other hand, intraoperative and postoperative outcomes, the rate of conversion, mean operative time, mean blood loss, and mean postoperative hospital stay showed no significant difference between the two groups. Also, there was no significant difference in rate of morbidity and mortality between the two groups. During a median follow-up of 37 months (range, 3–99 months), there was no significant difference in disease-free survival and overall survival.
Conclusions:
Laparoscopic liver resection for an HCC that is larger than 5 cm can be an optional treatment in selective cases.
Introduction
B
The aim of this study was to compare the outcomes of laparoscopic liver resection for HCCs ≥5 cm with those for HCCs <5 cm.
Materials and Methods
Patient selection
The medical records of 123 patients with HCC who underwent laparoscopic liver resection for HCC at Seoul National University Bundang Hospital (Seongnam, Republic of Korea) between September 2003 and December 2011 were retrospectively evaluated. An absence of severe portal hypertension and an adequate hepatic reserve were the prerequisites for surgery. Tumors invading or adjacent to the main portal pedicle, inferior vena cava, or major hepatic veins were considered to be relative contraindications. These patients were classified into two groups according to the size of the tumor: tumor ≥5 cm (Group A, n=20), and tumor <5 cm (Group B, n=113). The size was defined according to the Louisville Statement, where the acceptable size for laparoscopic hepatectomy was indicated as 5 cm or less. 8
Operative techniques
Only totally laparoscopic surgery was performed in every case of this study, and operative techniques for laparoscopic liver resection at our institution have been previously described.3,9,10
Pneumoperitoneum was established through a 10-mm umbilical port, and the pressure was maintained below 12 mm Hg to lower the risk of gas embolism. A 30° or flexible laparoscope was used. Laparoscopic ultrasonography was used to precisely localize the tumor, to demonstrate any satellite nodules of HCC, and to obtain an adequate tumor-free margin. This modality was used to overcome a known drawback of laparoscopy whereby the mass cannot be palpated.
The superficial hepatic parenchyma was transected using the Harmonic® scalpel (Ethicon, Cincinnati, OH) or the SonoSurg™ (Olympus, Tokyo, Japan), and the deeper portion of the parenchyma was dissected using a laparoscopic cavitron ultrasonic surgical aspirator (CUSA; Valleylab, Boulder, CO) to reduce hemorrhage.
For a right-sided resection, the patient was placed in the lithotomy or semilateral position. The liver was mobilized from the inferior vena cava, and multiple short hepatic veins were clipped and divided. Then, the portal pedicles were treated with a Glissonian approach or individual ligations. For individual ligations, the portal branch, arterial branch, and the bile duct were isolated. The portal branch and arterial branches were clipped and divided, and when the portal branch was too large for the clips to be applied, a linear stapler was used. The liver resection was performed next, following the line of ischemic color change.
Hilar dissection was performed to free the right and left Glisson's pedicles at the inferior surface of the quadrate lobe after the cholecystectomy. Then, for a right posterior or anterior sectionectomy, the right Glisson's pedicle was further dissected to visualize the anterior and posterior Glisson's pedicles. For more specific anatomical liver resections, the Glisson's pedicle for the lobe, section, or segment for the resection was ligated and divided using a linear stapler or vascular clips.3,9,10 For a left-sided resection, the patient was routinely placed in the supine position. The left hemihepatectomy was performed in a similar manner to that for the right-sided liver resection. When left lateral sectionectomy was performed, the parenchymal transection was performed just left to the falciform ligament with lateral traction of the round ligament. The Glisson's pedicles to segments II and III were divided either by endovascular gastrointestinal anastomosis or vascular clip, and the left hepatic vein was divided with an endovascular gastrointestinal anastomosis.
Once the specimen was completely detached, it was inserted into a vinyl bag for protecting the wound and preventing tumor seeding. The specimen was extracted through the incision created by extending the port site for small specimens or through an additional suparapubic transverse incision for large ones. After careful hemostasis and irrigation, a fibrin glue sealant (Greenplast®; Green Cross Corp., Seoul, Republic of Korea) was applied to the raw surface. A Silastic® (Dow Corning, Midland, MI) drain was then inserted at the transection plane, and the wound was closed in layers.
Statistical analysis
Normally distributed continuous variables are presented as means±standard deviations, and discontinuous variables are presented as the medians and ranges. Continuous parameters were compared using independent-sample t tests, and categorical parameters were compared using the chi-squared test. Nonparametric analysis was performed using the Mann–Whitney and Fisher's exact tests. Kaplan–Meier plots were used to test differences in time to recurrence and overall survival. The end point for overall survival was death. All analyses were performed using SPSS version 18.0 for Windows software (SPSS Inc., Chicago, IL), and differences were considered statistically significant for P values of <.05.
Results
The study cohort consisted of 95 men and 28 women with a mean age of 56.9 years (range, 26–87 years). The patient demographics, indications, and types of liver resection according to the size of the tumor (Group A, ≥5 cm; Group B, <5 cm) are shown in Table 1. There were significantly more major liver resections in Group A than Group B (P=.02), but no other demographic features were significantly different.
One case with caudate lobectomy.
F, female; M, male; SD, standard deviation.
The locations of the tumors in Group A are shown in Figure 1, and the overall intraoperative and postoperative results are listed in Table 2. There were no significant intergroup differences in the surgical margin (P=.32) and mean operative time (P=.22). Moreover, there were no significant differences in intraoperative blood loss and transfusions (P=.57 and 1.00, respectively). Also, there was no significant difference in postoperative hospital stay (P=.78). Eight patients underwent conversion to an open hepatectomy (Group A, n=2; Group B, n=6), and there was no significant difference in the conversion rate between the two groups (P=.615). Fifteen patients experienced postoperative complications: 3 (9.1%) in Group A and 12 (10.6%) in Group B, and there was also no significant intergroup difference (P=.71). The most frequent complications were biloma, fluid collection, and ascites, and some patients required percutaneous catheter drainage. There was one postoperative death in Group B. This patient was diagnosed with Child–Pugh Class A liver cirrhosis with a 15-minute retention rate for indocyanine green of 13.8%, and he underwent central bisectionectomy. The patient suffered from ascites infection, type 1 hepatorenal syndrome, and massive bleeding from a duodenal ulcer and died 1 month after the surgery.
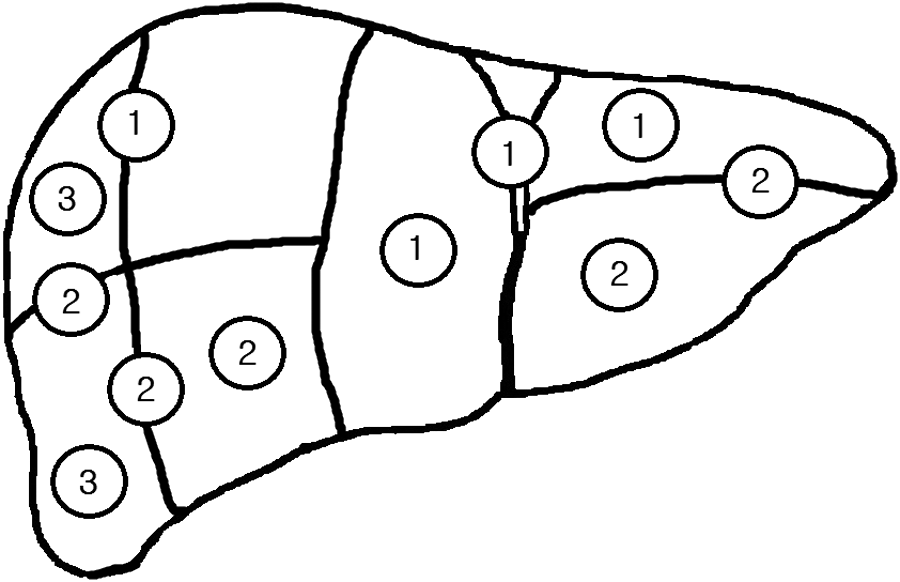
Location of large hepatocellular carcinoma lesions according to Couinaud's classification. The numbers in circles are the number of lesions in each corresponding segment.
SD, standard deviation.
During the mean follow-up of 36 months, there were nine recurrences in Group A and 43 recurrences in Group B, and there was no significant difference in rate of recurrence (P=.81). The median disease-free survival was 33.98±4.69 months for Group A and 57.34±4.55 months for Group B, and this difference was not significant (P=.49) (Fig. 2). The overall survival intervals for Groups A and B were 61.23±8.05 and 81.04±3.78 months, respectively, and this difference was not significant (P=.12) (Fig. 3).
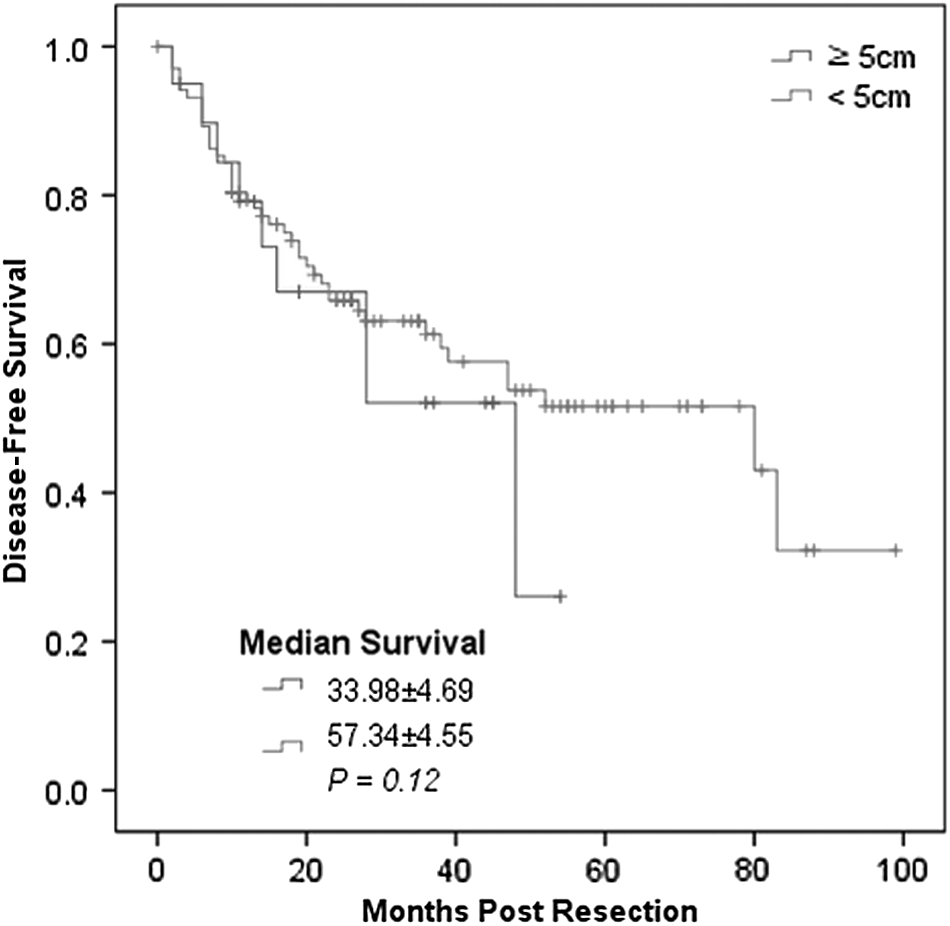
Disease-free survival.
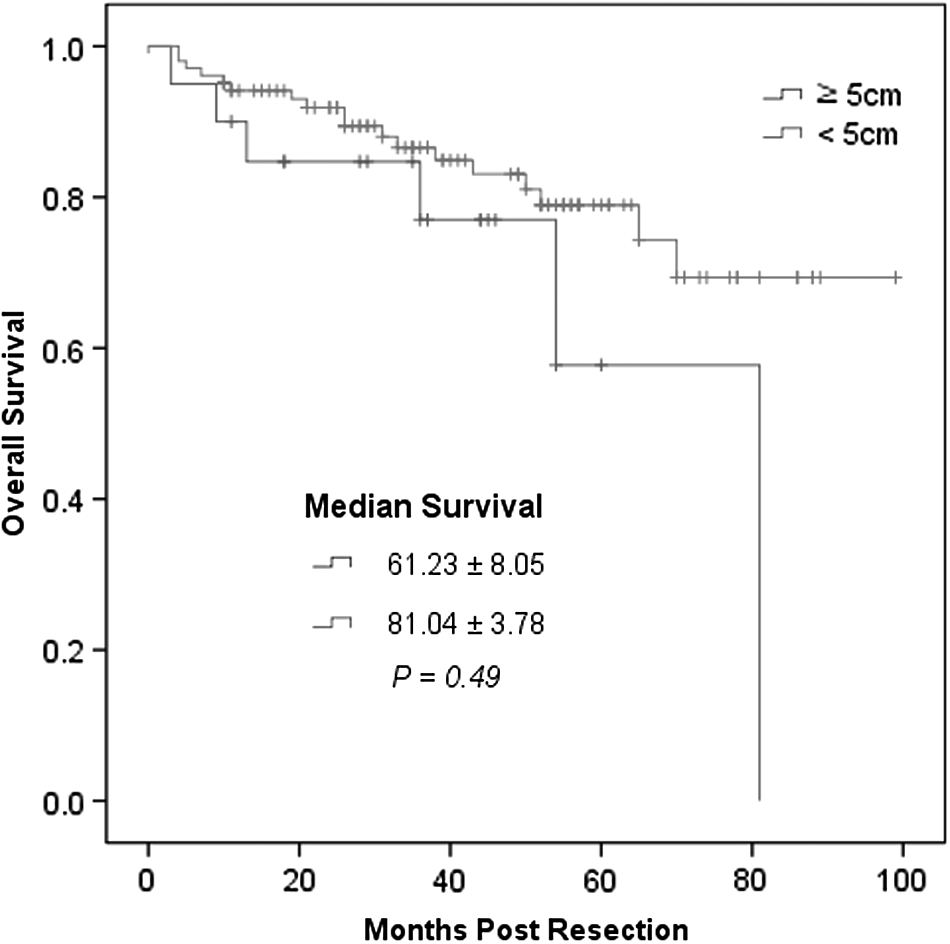
Overall survival.
In Group A, there were four intrahepatic and three extrahepatic recurrences. In 2 patients, recurrence occurred both intra- and extrahepatically. HCC mostly recurred contralaterally (n=7), and in 1 case, HCC recurred at a caudate lobe. There was no ipsilateral recurrence. The tumor tended to recur with multiple tumors (n=7) rather than a single tumor (n=2).
Discussion
Laparoscopic liver resection has advantages over open surgery in terms of less pain, reduced morbidity, shorter length of hospital stay, and potential improvements to immunologic outcomes. Furthermore, the accumulation of surgical experience with laparoscopic and hepatic surgery has widened the indications for laparoscopic liver resection, including the types of resection and the locations of the tumor.2,3,8,11–13
However, the expansion of indications to include tumors adjacent to the major hepatic vessels or located in the posterosuperior part of the liver is controversial owing to the inadequate operative view. 14 Also, tumors larger than 5 cm regardless of the tumor location have been considered contraindications for laparoscopic resection due to fear of rupture and difficulty in mobilization.3,5,8 Recently, however, tumors with characteristics that previously excluded them from being subject to laparoscopic resection have been successfully resected laparoscopically, including lesions in the posterosuperior segments of the liver.3,9
There are a few reports on the possibility of resecting large-sized hepatic tumors that are located on the anterolateral side (segments 2, 3, 5, 6, and the inferior part of segment 4 according to the classification of Couinaud) or pedunculated type tumors, which are suitable for tumorectomy or subsegmentectomy.4–7 The main difficulties of resecting large hepatic tumors are in obtaining the space for the operation, visualization of the operative field, and overcoming the possibility of rupture. The visualization problem has been overcome by adaptation of 30° or flexible laparoscopes, which provide a view from the superior side without interfering with the operative field. The delicacy of the resection was achieved by adopting the laparoscopic CUSA and other ultrasonic shear devices, providing a clear view throughout the operation with minimal bleeding, and fine dissection when performing parenchymal transection. 3
Besides these improvements in technology and equipment, the tailored method of port insertion, patient position, and appropriate selection of the resection type are important factors in performing laparoscopic liver resection for large hepatic tumors. For exophytic superficial tumors, tumorectomy and subsegmentectomy have been regarded as feasible irrespective of the tumor location.
In the Louisville statement on laparoscopic liver surgery, it was reported that the laparoscopic approach to left lateral sectionectomy should be considered as standard practice. 8 A large tumor located in the left lateral section has a higher possibility of tumor rupture and spillage during dissection of the left triangular ligament or retraction of the liver because of the limited space in the abdominal cavity under pneumoperitoneum. In contrast, right-sided lesions larger than 5 cm and that are deep seated are more amenable to laparoscopic resection than those located in the left side of the liver.3,10 However, it is possible to perform left lateral sectionectomy when adequate space between the falciform ligament and the mass can be provided. Adequate space for dissection and division of the Glisson is also necessary.
The possibility of rupture must be considered when performing resection for patients with a large HCC. Anatomic liver resection is the preferred technique for large HCCs as tumor margins are superior to those of tumorectomy. Moreover, the characteristic of the tumor is also important, although it is usually evaluated during the operation. When the tumor is friable and there is higher percentage of tumor spillage, conversion to open surgery should be performed. Preoperative imaging studies are also necessary before considering a laparoscopic approach, and when the imaging results suggest there may be a danger of rupture, open surgery is the preferred option.
The advantages of laparoscopic liver resection over open liver resection have been previously reported.6,8,14,15 However, tumor size has been regarded as one of the most important limitations to a laparoscopic approach. However, we did not find a difference in perioperative results due to increased tumor size. There was no significant intergroup difference in the rate of open conversion, mean operative time, mean blood loss, and postoperative hospital stay. Also, there was no significant difference in postoperative morbidity in both groups. Furthermore, there was no significant difference in disease-free survival, and our results suggest that laparoscopic liver resection for large tumors in selective patients can be safely and effectively performed.
Conclusions
In conclusion, laparoscopic liver resection for hepatic tumors larger than 5 cm is safe and feasible in selected patients. The surgical technique must be individualized according to the tumor location and relationship to the major hepatic vessels. Extra caution is warranted to avoid rupture when resecting exophytic masses.
Footnotes
Disclosure Statement
No competing financial interests exist.