
Abstract
Abstract
Background:
Reports on laparoscopic liver resection for intrahepatic cholangiocarcinoma are still scarce. With increased experience in laparoscopic liver resection, its application to intrahepatic cholangiocarcinoma can now be considered. Our aim is to determine the feasibility and safety of laparoscopic liver resection for intrahepatic cholangiocarcinoma and to analyze its clinical and oncologic outcomes.
Patients and Methods:
Among the 84 patients with intrahepatic cholangiocarcinoma operated on from March 2004 to April 2012, 37 patients with a T-stage of 2b or less were included in the study. Eleven patients underwent laparoscopic liver resection, and 26 underwent open liver resection. Treatment and survival outcomes were analyzed.
Results:
Intraoperative blood loss was significantly greater in the open group (P=.024), but with no difference in the blood transfusion requirement between groups (P=.074), and no operative mortality occurred. The median operative time, postoperative resection margin, and length of hospital stay were comparable between groups (P=.111, P=.125, and P=.077, respectively). Four (36.4%) patients in the laparoscopic group developed recurrence compared with 12 (46.2%) patients in the open group (P=.583). After a median follow-up of 17 months, the 3- and 5-year overall survival rates were 77.9% and 77.9%, respectively, in the laparoscopic group compared with 66.2% and 66.2%, respectively, in the open group (P=.7). There was also no significant difference in the 3- and 5-year disease-free survival rates for the laparoscopic group at 56.2% and 56.2%, respectively, versus the open group at 39.4% and 39.4%, respectively (P=.688).
Conclusions:
Laparoscopic liver resection for intrahepatic cholangiocarcinoma is technically safe with survival outcome comparable to that of open liver resection in selected cases.
Introduction
I
Laparoscopic liver resection (LLR) has gained increasing acceptance in recent years as an attractive procedure for the treatment of HCC.3,4 Compared with laparoscopic peripheral tumorectomy in early stages, advances in surgical techniques and improved equipment now allow the successful performance of major liver resection for HCC. In contrast, LLR for ICC is not commonly performed because of the scarcity of reports on its application for this indication and concern for inadequate resection margin and laparoscopic lymph node dissection. An inadequate resection margin may result from the satellite nodules and occurs occasionally in ICC. Unlike HCC, ICC may have metastatic lymph nodes, and some surgeons therefore advocate the necessity of lymph node dissection.
A few studies on LLR for ICC have recently been published, although they are primarily case reports.5–9 With increasing experience in laparoscopic liver surgery, the prospect of a laparoscopic approach for the management of ICC can no longer be considered as an extreme or rare procedure. The aim of our study was to determine the feasibility and safety of LLR for ICC and to analyze its clinical and oncologic outcome compared with conventional open liver resection.
Subjects and Methods
Study population and definitions used
Between March 2004 and April 2012, 84 (61 open, 23 laparoscopic) patients underwent liver resection for ICC at Seoul National University Bundang Hospital. Patients pathologically diagnosed as having ICC with a T-stage of 2b or less were included in our study. The exclusion criteria were as follows: (1) palliative resection, (2) concurrent other malignancy, (3) mixed HCC and cholangiocarcinoma, and (4) the periductal infiltrative type of cholangiocarcinoma. Laparoscopic surgery was performed with the pure laparoscopic approach as defined in the 2008 International Louisville Consensus, 10 wherein the entire operation is performed through laparoscopic ports, and only a small incision is made to extract the specimen afterward.
Thirty-seven patients met the inclusion criteria for the study. The patients' demographic data, preoperative laboratory values, tumor location, operative procedure, perioperative outcome, pathology report, and postoperative follow-up data were collected from the hospital database. The patients were divided into two groups according to the type of operation: LLR or conventional open liver resection. The operations done in the two groups were further classified into major or minor liver resections, according to the extent of resection. Major hepatic resections were defined as resection involving more than two segments. Minor liver resections were for resections involving two segments or less. 3 Right anterior and posterior sectionectomies were classified as major resections as these procedures require advanced technique and longer operation time. 11 Tumor staging was based on the pathologic Tumor Node Metastasis (TNM) classification of the American Joint Committee on Cancer, 7th edition.12,13 Lymph node dissection was selectively performed in both groups. Lymph node dissection was not performed in cases preoperatively diagnosed as having the intraductal papillary growth type of ICC. 14 The laparoscopic lymph node dissection technique was described in a previous study. 15 The extent of lymph node dissection included the hepatoduodenal ligament (no. 12) and the common hepatic artery (no. 8). 16
Follow-up and outcome measurement
A routine follow-up protocol was performed, including a physical examination and laboratory tests such as carcinoembryonic antigen, cancer antigen 19-9, liver function tests, and other routine blood tests. The laboratory tests were performed every 3 months for the first 2 years and then every 6 months for 5 years. Follow-up contrast-enhanced computed tomography and/or magnetic resonance imaging was performed to detect recurrence.
Statistical analysis
Continuous variables were reported as the median and range. The Mann–Whitney U test was used to identify significant differences for continuous variables, whereas the chi-squared test was used to determine the difference in the distribution of categorical variables between groups.
Overall and disease-free survival rates were analyzed using the Kaplan–Meier method, and the log-rank test was used to assess differences between groups. All analyses were performed using SPSS for Windows version 16 software (SPSS, Inc., Chicago, IL). A value of P<.05 was considered significant throughout the study.
Results
Baseline characteristics
The demographic data of enrolled patients are summarized in Table 1. Eleven patients underwent LLR, whereas 26 patients had conventional open liver resection for ICC. The patient age, gender, liver status, and preoperative American Society of Anesthesiologists score were not significantly different between the two groups (P>.05).
ASA, American Society of Anesthesiologists; CLD, chronic liver disease; F, female; LC, liver cirrhosis; M, male; N, normal liver.
Pathology data
Tumor size was comparable between the laparoscopic and the open groups (P=.702). No significant differences in tumor location (P=.660) or T-stage (P=.695) were found. No statistically significant difference in the postoperative analysis of the specimen resection margin was noted (P=.125) (Table 2).
Perioperative outcomes
The intraoperative and postoperative results are listed in Table 3. No significant differences were noted in the extent of resection (P=.051) and operative time (P=.111). Among the 11 patients in the laparoscopic group, 6 patients were preoperatively diagnosed as having HCC (n=4), angiomyosarcoma (n=1), and colorectal metastasis (n=1); therefore, lymph node dissection was not performed. In the remaining 5 patients who were preoperatively diagnosed as having ICC, only 1 patient had lymph node dissection performed. However, the pathology report was negative for lymph node metastasis. Nineteen patients in the open liver resection group underwent lymph node dissection, and 5 patients were positive for lymph node metastasis. The open liver resection group had more blood loss intraoperatively (P=.024) than the laparoscopic surgery group. The open group had a tendency to require a larger blood transfusion compared with the laparoscopic group, but this did not reach statistical significance (P=.074). The laparoscopic group also tended to have a shorter operation time and length of hospital stay, but this was not statistically significant (P=.111 and P=.077, respectively). No operative or perioperative mortality was observed in either group.
Continuous variable: presented as “median (range).”
Significant difference.
The postoperative complications were not significantly different between the two groups (P>.05). The laparoscopic surgery group included 1 patient who developed significant ascites due to severe liver cirrhosis postoperatively but was successfully managed conservatively and later recovered. Two patients in the open surgery group had symptomatic abdominal fluid collection, 2 developed wound problems, 2 had pneumonia, and only 1 patient experienced ileus postoperatively.
Recurrence and survival
The follow-up data for recurrence and survival are listed in Table 4. Four patients (36.4%) in the laparoscopic group developed recurrence compared with 12 (46.2%) of the patients in the open liver resection group. No statistically significant difference was noted in the percentage of patient recurrence between the two groups.
After a median follow-up period of 17 months (range, 0–94 months), overall patient survival and disease-free survival were calculated for both groups. The 3- and 5-year overall survival rates were 77.9% and 77.9%, respectively, in the laparoscopic group compared with 66.2% and 66.2%, respectively, in the open surgery group (P=.7) (Fig. 1). There was also no significant difference in the 3- and 5-year disease-free survival rate for the laparoscopic group at 56.2% and 56.2%, respectively, versus the open surgery group at 39.4% and 39.4%, respectively (P=.688) (Fig. 2).

Overall survival (P=.7). mos, months.
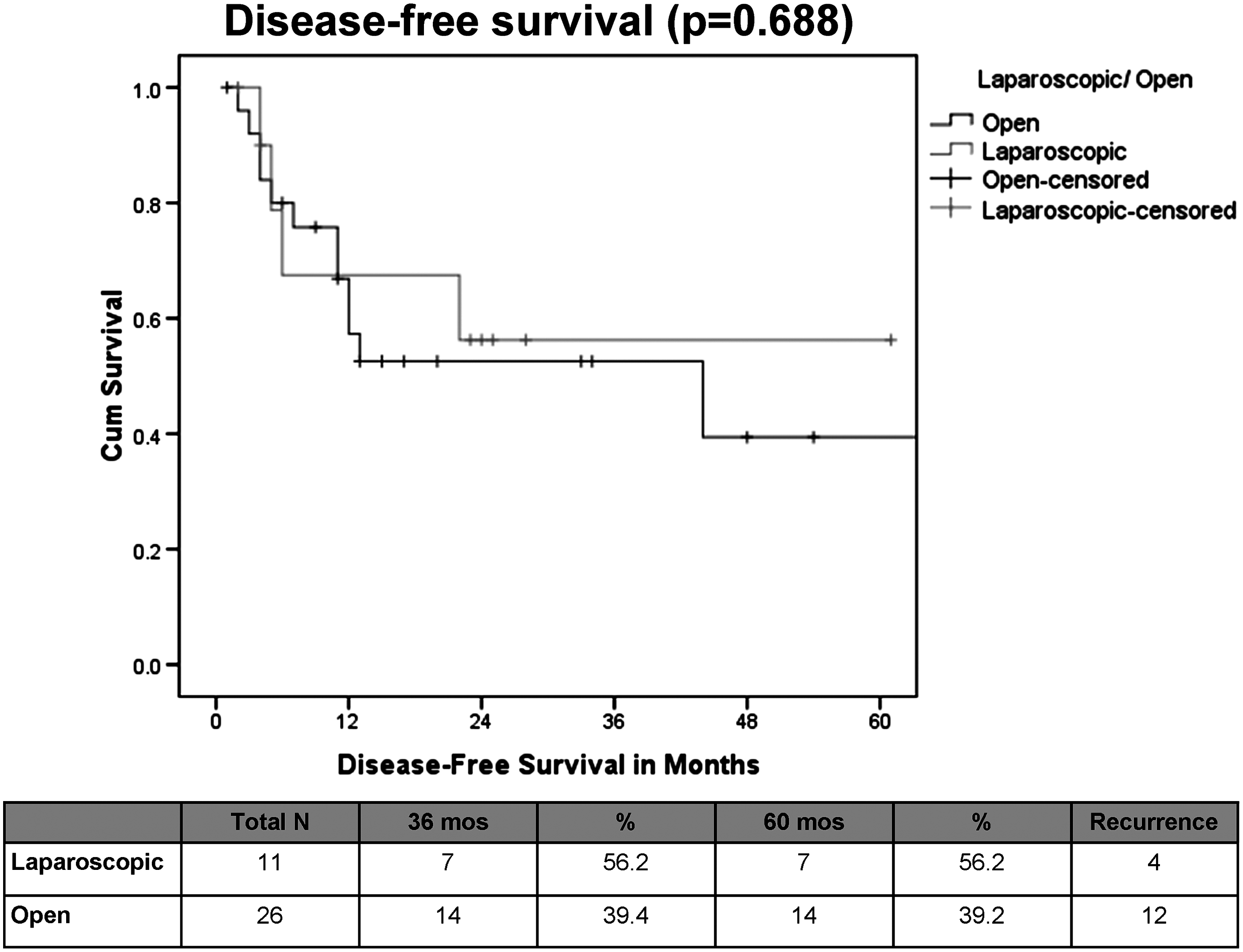
Disease-free survival (P=.688). mos, months.
Discussion
There are still only a few reports on LLR for ICC. Abu Hilal et al. 6 reported that laparoscopic left hemihepatectomy and caudate lobe resection for patients with ICC is feasible and safe. This was the first description of 2 cases of LLR for ICC. Another study on LLR for ICC was a report of a minimally invasive approach to extrapancreatic cholangiocarcinoma by Gumbs et al. 9 Their study concluded that minimally invasive surgery on gallbladder cancer and hilar cholangiocarcinoma and ICC was feasible and safe. However, neither study reported the oncological outcome or recurrence pattern.
We collected the data of all patients who underwent LLR and open liver resection for ICC. Cases were carefully selected to include only those with pure cholangiocarcinoma and with a T-stage of 2b or less. The selection criteria were based on studies of T-stage in ICC. In 2009, Nathan et al. 17 reported that the T-stage was an independent predictor of survival after liver resection for ICC. In the American Joint Committee on Cancer 7th edition, 13 the T3 stage involves tumor perforation of the visceral peritoneum or direct extension into adjacent extrahepatic structures. Therefore, the combined resection of other involved organs may be necessary. Hence, we excluded T3 lesions from our study because combined resection would be a complicated laparoscopic procedure.
In the AJCC 7th edition, the periductal infiltrating type was classified as T4 because of its extensive infiltrative behavior and higher lymphatic spread.12,18 Some studies on the periductal infiltrative type of cholangiocarcinoma have shown an unfavorable prognosis.19,20 The periductal infiltrative type has a greater than 60% incidence of lymph node metastasis compared with 30%–50% in mass forming and even less for the intraductal growth type. The differences in the pattern of lymphatic spread of the different histologic types and the more infiltrative nature of the periductal type of ICC resulted in its exclusion from our study.
Laparoscopic lymph node dissection has recently become popular in laparoscopic surgery, particularly in gastric and colon cancer. We have previously reported on laparoscopic lymph node dissection in gallbladder cancer. 15 We performed selective lymph node dissection for the laparoscopic group. Most of the patients did not undergo lymph node dissection because the preoperative diagnoses were HCC or the intraductal papillary growth type of ICC. Only 1 patient in the laparoscopic group underwent a laparoscopic lymph node dissection, but the pathology result was negative for metastasis. The follow-up outcomes in our study also showed no extrahepatic lymph node recurrence, even without lymph node dissection in the laparoscopic group.
Whether lymph node dissection should be performed for ICC remains unclear. Some argue against extensive lymph node dissection because of its potential morbidity given the high recurrence rate of ICC even in R0 resection.21–23 In a recent study, Morine et al. 14 concluded that routine lymph node dissection is not recommended for peripheral ICC. Surgery alone, including lymph node dissection, cannot control this type of tumor 24 because lymph node metastasis is seldom limited to the regional lymph nodes and because most tumor recurrence occurs in the remnant liver. There were no differences in survival in patients who had lymph node dissection and those who did not. Therefore, lymph node dissection might be unnecessary for peripheral-type ICC, 14 particularly the mass-forming type. 25 As the intraductal papillary growth type has a low lymph node metastasis rate, lymph node dissection may also be unnecessary.14,18,24
Typically, laparoscopic liver surgery for ICC presents advantages in the duration of hospital stay and complication rates, but these were not significantly different from those of the conventional group in our study because of the small sample size. The 3- and 5-year overall survival rates of the LLR group were comparable to those of the open resection group. The 3- and 5-year disease-free survival rates were also not significantly different between the two groups. This suggests that LLR for ICC can be performed with the same level of oncologic safety in centers experienced with minimally invasive techniques with no difference in long-term outcome compared with those who undergo conventional open liver resection.
The results from our study demonstrated that the laparoscopic approach to the resection of ICC can be performed safely and without compromising adequate resection margins, operation time, or the complication rate. Laparoscopic surgery is reported to result in less blood loss, less pain, and faster patient recovery.10,26,27 In our study, less intraoperative blood loss occurred in the laparoscopic group. With the present advances in laparoscopic techniques, we believe that LLR for ICC can be adapted as an optional operative approach and even be applied to selected cases. Although our study is one of the few studies performed regarding LLR for ICC, its application was constrained by the retrospective analysis of a limited number of patients as well as the limited experience and literature available. We therefore recommend further studies for its future application.
Conclusions
LLR for ICC is technically safe and has a comparable survival outcome compared with open liver resection. It can be an alternative approach to the management of ICC but only for selected cases and in centers experienced in LLR.
Footnotes
Disclosure Statement
No competing financial interests exist.