
Abstract
Abstract
Background:
The aim of this study was to evaluate the clinical application and superiority of the da Vinci® Si Surgical System (Intuitive Surgical Inc., Sunnyvale, CA) in total parathyroidectomy for secondary hyperparathyroidism.
Materials and Methods:
Total parathyroidectomy was performed with the da Vinci Si Surgical System by the four-trocar axillo-bilateral-breast approach. The patients were placed in the supine position, and the operation procedure included creating the workspace, docking, and consoling stages. The camera arm is centered in the working space. Three working arms are then placed adjacent to the camera. The Harmonic® scalpel (Ethicon Endo-surgery, Inc., Cincinnati, OH) was used for hemostasis and gland resection, and dissected parathyroid was taken out by a specimen pouch.
Results:
Total parathyroidectomy with trace amounts of parathyroid tissue autotransplantation in 6 patients was successfully performed with the da Vinci Si Surgical System. There were no operation-related complications and no conversions to open or endoscopic surgery. Mean operation time was 156 minutes. Patients were discharged from the hospital 6 days after surgery. The postoperative cosmetic result was satisfactory, with minimal numbness and tingling on the anterior chest.
Conclusions:
This initial study shows that robotic total parathyroidectomy via the axillo-bilateral-breast approach is a safe and feasible alternative to selected patients, especially those with esthetic concerns.
Introduction
T
Materials and Methods
Patient eligibility and study design
One woman and five men with end-stage renal disease had secondary hyperparathyroidism. Mean age was 41 years old (range, 30–52 years). They underwent hemodialysis for a mean of 9.3 years (range, 5.5–13 years). One parathyroid gland had been removed in a 45-year-old male patient a year ago. The mean serum parathyroid hormone level was 1670 ng/L. Heights decreased an average of 6.5 cm in the 6 patients. Preoperative patient workups include a physical examination and imaging methods, such as high-resolution ultrasonography and 99mTc-sestamibi-single-photon emission computed tomography/computed tomography (99mTc-MIBI-SPECT/CT). Patients with any of the following were not offered a robotic approach: a history of significant thyroiditis, previous neck surgery or irradiation, severe Hashimoto's thyroiditis, obesity (body mass index, >27 kg/m2), enlarged thyroid gland detected on ultrasonography (>second-degree), and a suspicion of malignancy. All patients provided written informed consent for the study, and the study was approved by the Jinan Military General Hospital Research Ethics Board.
Surgical technique
Workspace creation
Patients, under general anesthesia with endotracheal intubation, were placed on the operating table in the supine position with the neck extended slightly. After draping, instrument arm trajectory lines and the working area were drawn onto the patient's chest and neck area for reference (Fig. 1). Bilateral skin incisions (8 mm) were made on the margin of the areola. A 12-mm incision on the right side of the sternum beside and the 8-mm incision on the right or left the axillary crease outside the lateral border of the pectoralis major muscle were then made. After incisions, blunt dissection was carefully performed with a vascular tunneler through the port incisions to develop space in the trajectory lines and working area, as well as laterally to the medial border of the sternocleidomastoid muscle. The camera port first was placed on the right of the sternum (the drawing of the eye), using a disposable 12-mm trocar. Ports 1, 2, and 3 for the instrument arms were placed in the superomedial edge of the breast areola and the fold of the axilla (Fig. 1).

The four-trocar axillo-bilateral-breast approach.
Patient cart positioning
The patient cart was rolled into position over the patient's head with the center column in line with the camera port, slightly angled to the operation table and the patient's head. The Mayo stand was placed toward the foot of the table for instrumentation, if desired.
Docking of the surgical robot system
Each of the four ports was docked with a robotic arm (Fig. 2). The da Vinci instrument ports were pointed toward the center of the cricoid cartilage using set-up joint release or port-clutch maneuvers.

The four-arm da Vinci Surgical System, docked.
Console stages
The general principle of operation proceeding for robotic total parathyroidectomy was in the same manner as conventional open parathyroidectomy. The working space was further cleared with a Harmonic® scalpel (Ethicon Endo-surgery, Inc., Cincinnati, OH) and maintained by CO2 insufflation at 6–7 mm Hg. The thyroid gland was then grasped by the grasp forceps and rotated medially. Next, the middle thyroid vein was dissected with the dissector and divided using the Harmonic scalpel. The recurrent laryngeal nerve was dissected in the tracheoesophageal groove, and the recurrent laryngeal nerve was located. The thyroid lobe was at that point rotated medially, and with cautious dissection the parathyroid was identified. Because of its visual perspective of surgical anatomy, the parathyroid was then circumferentially dissected and excised en bloc with the thyroid lobe. By the combination of preoperative ultrasonography, 99mTc-MIBI-SPECT/CT, and intraoperative exploration, each of the parathyroid glands was carefully discovered and removed (Fig. 3). The dissected parathyroid was taken out by a specimen pouch. The estimated weight of the autograft parathyroid tissue is 30 mg. 2 The intraoperative parathyroid hormone level should be 50–110 ng/L, which was monitored throughout the procedure to ensure a successful operation. 3
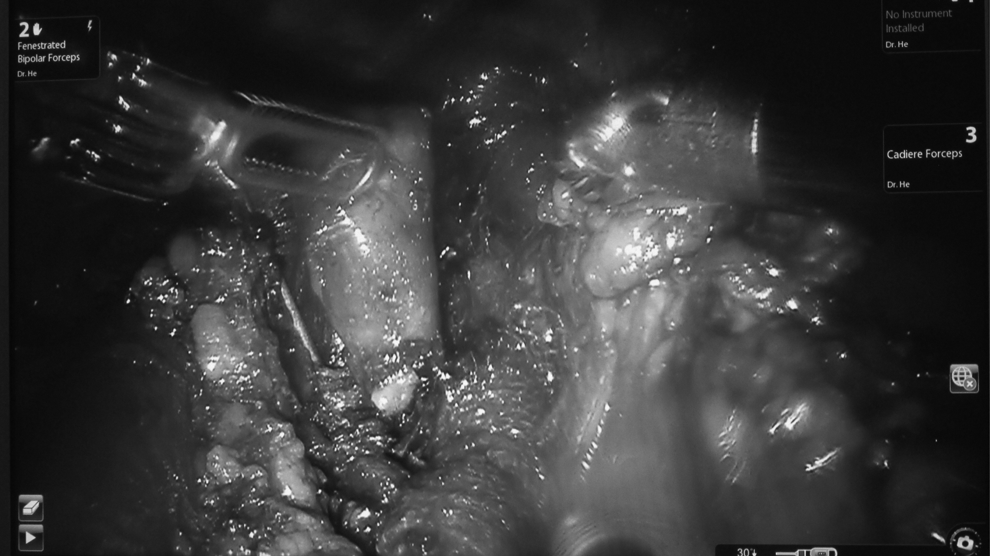
Identification and excision of the inferior parathyroid gland.
After discharge, the follow-up time was 7–10 months. Follow-up biochemical markers included serum phosphate, calcium, and parathyroid hormone. A scoring system was used by patients' self-assessment to grade the cosmetic outcome between 0 and 10.
Results
Robotic total parathyroidectomy with trace amounts of parathyroid tissue autotransplantation in 6 patients was completed successfully as planned. Five patients had four parathyroid glands removed each; 1 patient had only three. There were no conversions to open or endoscopic surgery. The mean time for creating the workspace was 40 minutes, the docking stage was 12 minutes, and the console stage was 104 minutes. Pathological diagnosis showed all patients had parathyroid hyperplasia.
There were no complications related to the robotic approach and no occurrences of any postoperative hemorrhage or voice changes. Graft-dependent recurrence was not observed. All patients' self-assessment (the postoperative cosmetic result) scores were satisfied (scores of 8) or very satisfied (scores of 9 or 10) (Fig. 4). The hypesthesia and paresthesia resolved after about 4 months.

Operative scar 3 days after robotic total parathyroidectomy.
Discussion
Robotic parathyroidectomy is a new and emerging technique with early outcomes that are at least comparable to those of conventional endoscopic parathyroidectomy. 4 Postoperative cosmetic status was excellent. Women are relatively suitable for the endoscopy operation, whereas male patients tend to have an uplifting clavicle and sternal handle with shorter cervical vertebrae. Also, 35.1% of inferior parathyroid glands were located in the thymus tongue lobe for all patients.2,5 Infraclavicular ectopic parathyroid glands are extremely difficult to resect because the clavicle interferes with insertion of the endoscopic forceps instrument into the deep and narrow workspace. However, the flexible robotic instruments allow the dissection of the transcervical thymus gland, which is difficult to reach with the conventional endoscope.
Certain facts should not be ignored: the benefits that the robot provides come with the risk of additional complications such as bleeding or numbness/tingling from the flap creation. The total time of robotic total parathyroidectomy is longer than that of the conventional parathyroidectomy owing to the complicated instruments and precise preoperative preparations.
Endoscopic total parathyroidectomy by the five-trocar anterior chest approach was successfully performed. 6 Moreover, to our knowledge, robotic total parathyroidectomy by the four-trocar axillo-bilateral-breast approach for secondary hyperparathyroidism has not been previously reported in the literature.
Conclusions
The axillo-bilateral-breast approach hence could be suggested as a novel alternative for robotic total parathyroidectomy for selected patients with cases of secondary hyperparathyroidism who wish to avoid neck scars.
Footnotes
Acknowledgments
This work was supported the President Funding of Jinan Military General Hospital of PLA (grants 2011 M 03 and 2013 ZD 05).
Disclosure Statement
No competing financial interests exist.