
Abstract
Abstract
Aim:
We aimed to understand how changes in surgical techniques are transferred into surgical practice. We hypothesized that the integration of minimally invasive surgery (MIS) techniques into a pediatric surgical practice is dependent on the hiring of junior partners who can transfer their MIS knowledge to senior surgeons.
Materials and Methods:
We reviewed the operative approach to six different general pediatric surgical procedures from 2000 to 2012, including appendectomy, fundoplication, gastrostomy tube placement, pyloromyotomy, colectomy, and lobectomy (lung). The percentage of MIS cases was calculated for each procedure annually. Each year six to nine fellowship-trained pediatric surgeons operated at our institution. Three surgeons completed training in the era of MIS (hired in 2001, 2007, and 2009) and remained on staff for at least 3 years.
Results:
In 2000, 49% of procedures were performed with MIS. This increased to 98% in 2013 (P<.0001). Appendectomy, pyloromyotomy, and fundoplication demonstrated early adoption and uniform use of laparoscopy (>85%) by 2007. Gastrostomy tube placement reached 90% laparoscopy utilization in 2009. Lobectomy (lung) and colectomy also reached >80% MIS use in 2009 and 2010, respectively. The same trends were seen when looking only at senior surgeons who completed training prior to 2000.
Conclusions:
The hiring of junior surgeons with MIS training was associated with an increase in adoption of MIS techniques by the entire group. Procedures that were introduced early in the MIS era demonstrated a gradual rise toward uniform adoption of MIS techniques. More advanced and recently adopted MIS techniques demonstrated a rapid rise to uniform adoption.
Introduction
A
Materials and Methods
Following approval of the Colorado Multiple Institution Review Board, we performed a retrospective review of the operative techniques used to perform six different general pediatric surgical procedures at Children's Hospital Colorado from 2000 to 2012. Procedures evaluated included appendectomy, fundoplication, gastrostomy tube placement, pyloromyotomy, colectomy, and lobectomy (lung). We queried the operative database as well as the department's billing records for these six procedures during the study period. Data collected included operation performed, whether an open or MIS approach was used, date of operation, and the operating surgeon. During the study period, in total, 15 different board-certified pediatric surgeons operated at Children's Hospital Colorado with between six and nine surgeons operating in any given year. Ten of the 15 completed their pediatric surgery training prior to 2000 (senior surgeons), with the remaining 5 finishing training after 2000 (junior surgeons). During the study period, three surgeons were hired who remained on staff for more than 3 years. These surgeons entered practice in 2001, 2007, and 2009, respectively.
Trends in MIS utilization for each procedure were documented each year for both the group as a whole and among only the senior surgeons. Additionally, we documented the makeup of the group (distribution of junior and senior surgeons) each year of the study. Statistical comparisons were made between the first and final years of the study using Fisher's exact test. A P value of <.05 was considered statistically significant. Statistical analysis was performed in Prism version 6.0b software (GraphPad Software, Inc., La Jolla, CA).
Results
Over the 13-year study period, the average number of each procedure performed per year was as follows: appendectomy, 238; fundoplication, 129; gastrostomy tube placement, 102; pyloromyotomy, 56; colectomy, 8; and lobectomy (lung), 7. When looking at these six procedures as a group, 364 total procedures were performed in 2000, 177 of which (48.6%) were performed using MIS techniques. In 2012, 895 procedures were performed, 874 with MIS techniques (97.7%) (P<.0001). Table 1 documents the number and percentage of each of the separate procedures that were performed using MIS techniques each year. In 2000, less than half of the operations for each procedure were performed with MIS. This increased to over 80% for all procedures by 2012. Figure 1 demonstrates these trends as well as how the rate at which MIS techniques were adopted varied with each procedure. Appendectomy, pyloromyotomy, and fundoplication were the first procedures to reach relatively uniform adoption of MIS techniques. By 2007 more than 90% of each of these procedures were performed laparoscopically. Gastrostomy tube placement reached 90% adoption of MIS techniques by 2009. Colectomy and lobectomy (lung), the most complex and rare procedures evaluated, were the last to see uniform adoption of MIS techniques, not occurring until 2010 and 2011 respectively.
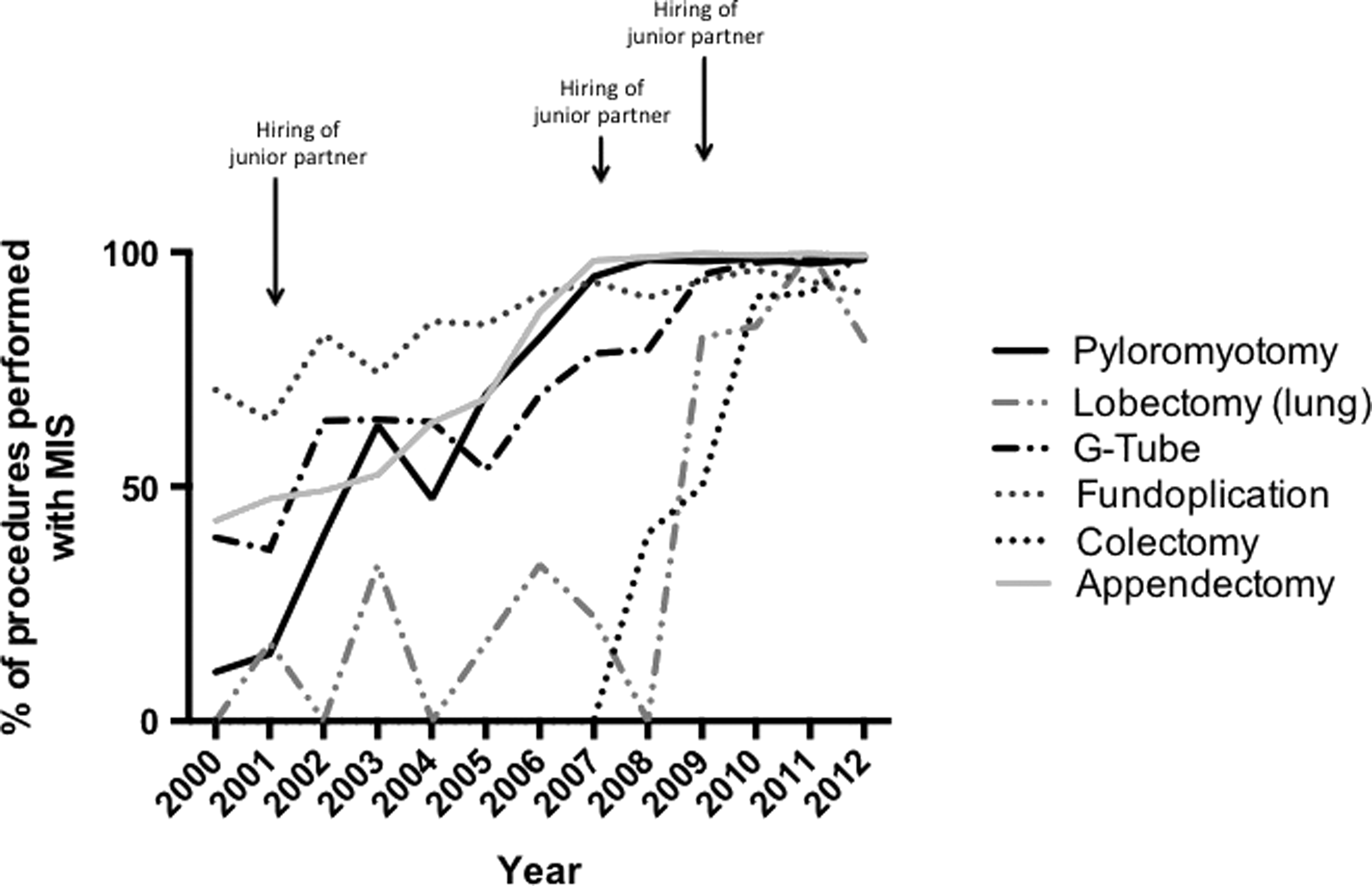
Trends in adoption of minimally invasive surgery (MIS) techniques for six pediatric general surgery procedures. The data demonstrate a rise in the proportion of procedures that were performed using MIS techniques for each of six different general surgical procedures. Pyloromyotomy, appendectomy, and fundoplication showed the earliest rise in MIS use and uniform adoption of MIS techniques by 2006. Gastrostomy tube (G-Tube) placement showed uniform adoption of MIS by 2008. Lobectomy (lung) and colectomy did not reach uniform adoption of MIS techniques until 2011.
Data are number (%).
Over the 13-year period, the percentage of staff surgeons who had completed training after 2000 increased, making up approximately 50% of the faculty from 2009 to 2012. Table 2 documents the percentage of MIS procedures that were performed by surgeons who completed training before 2000. The bottom row of Table 2 lists the percentage of all MIS procedures performed by senior surgeons. Figure 2 demonstrates the variation in percentage of MIS procedures performed by senior surgeons, compared with the percentage of the staff surgeons made up by senior surgeons. Figure 2 demonstrates that these rates vary in a comparable manner.
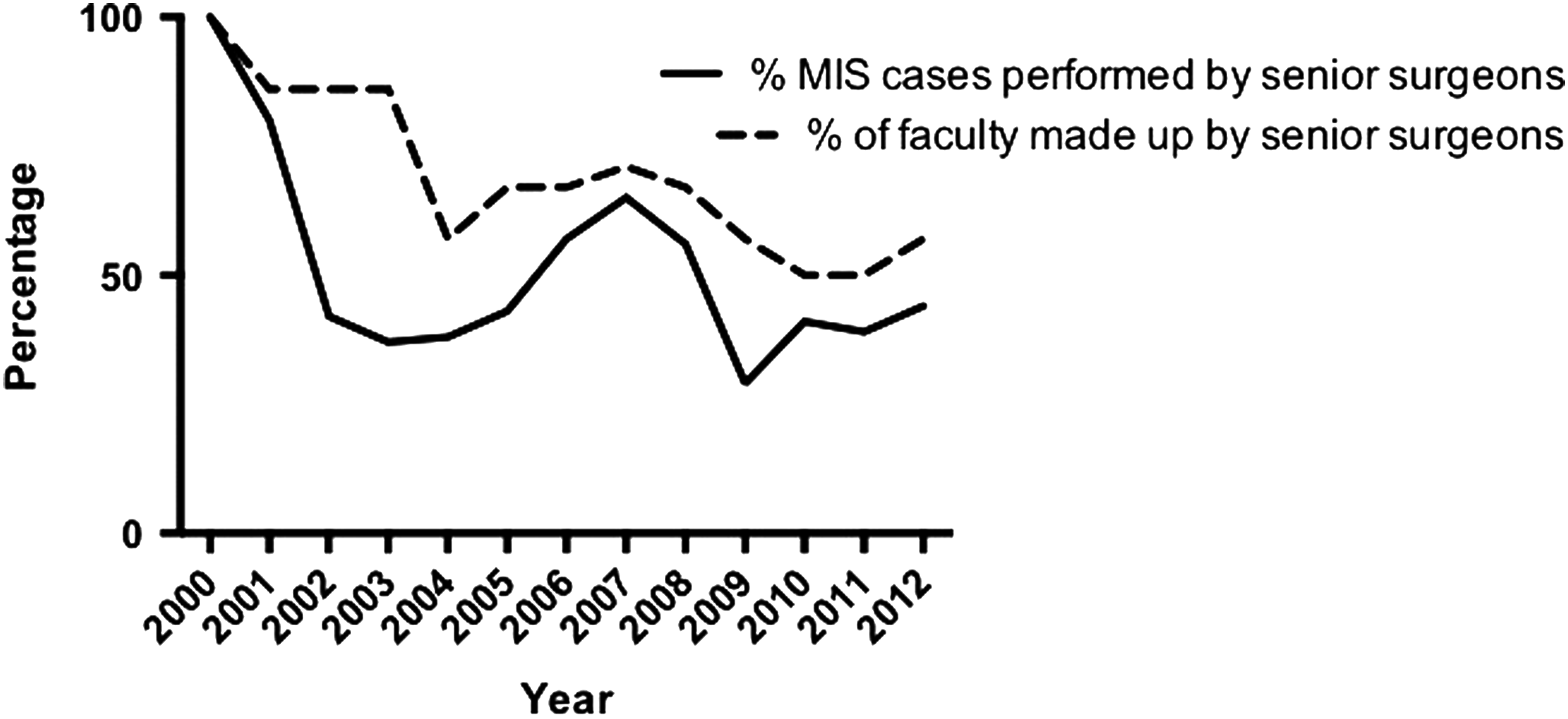
Trends in the percentage of faculty made up by senior surgeons and percentage of minimally invasive surgery (MIS) cases performed by these surgeons. The dashed line documents the percentage of faculty surgeons who completed training prior to 2000 each year. The solid line represents the percentage of MIS cases performed by this group of senior surgeons. The data demonstrate that senior surgeons performed a relatively constant percentage of MIS cases, relative to the distribution of faculty surgeons.
Data are number (%). A senior surgeon was one who had completed training prior to 2000.
When looking only at senior surgeons, we found that the same trends shown among the group as a whole were demonstrated. Our data demonstrated that the older surgeons also gradually moved to uniform use of MIS techniques to perform appendectomy (98%), fundoplication (92%), and pyloromyotomy (92%) by 2007 and gastrostomy tube placement (90%) by 2009. Senior surgeons performed a much smaller percentage of all lobectomies (lung) and colectomies. However, those senior surgeons who performed these more advanced procedures did move to an MIS approach by 2010 and 2011, as was seen when looking at the group as a whole. The rate of MIS approach among senior surgeons for all six of these procedures increased from 49% in 2000 to 98% in 2012 (P<.0001).
Discussion
Since the first laparoscopic cholecystectomy was performed in 1985, 2 the use of MIS techniques has increased rapidly among general and pediatric surgeons.4,5,7 The adoption of MIS in pediatric surgery was somewhat slower than it was in adult surgery because of underappreciation of postoperative pain among children, lack of appropriately sized instruments, and a relatively steep learning curve. 5 Despite this early delay, MIS approaches are now considered the standard of care in the treatment of a variety of pediatric surgical diseases, including the six procedures evaluated here: appendectomy, fundoplication, gastrostomy tube placement, pyloromyotomy, colectomy, and lobectomy (lung).8–14 In addition to their widespread use in pediatric general surgery, MIS techniques have also seen extensive utilization in the treatment of pediatric urologic pathologies, with pediatric urologists leading the way in the adoption of MIS techniques in children. Common MIS procedures performed by pediatric urologists include varicocelectomy, laparoscopic treatment of urolithiasis, and tissue anastomoses.15–17 The benefits of MIS in children include smaller scars, decreased postoperative pain, shorter hospital length of stay, and earlier return to regular activities. 5
Our data demonstrate that the adoption of MIS techniques did not occur at the same rate for all procedures. The procedures that were more common and performed most frequently in our institution demonstrated relatively early adoption to an MIS approach among all surgeons. In 2000, only 10% of pyloromyotomies were performed laparoscopically. This rate rose steadily over the following 7 years to reach uniform utilization (>95%) of laparoscopic pyloromyotomy among all surgeons in the group by 2007. A similar trend was seen with appendectomy: by 2007 almost all appendectomies (>95%) were performed laparoscopically. The increased use of MIS began in 2001 following the hiring of the first pediatric surgeon who had completed training in the era of MIS. It is interesting that similar trends were seen with the more complex laparoscopic procedures of lobectomy (lung) and colectomy. We initially hypothesized that it was only the pediatric surgeons who had completed training after 2000 who were performing the majority of the MIS operations. However, our data demonstrate that, over time, for each separate procedure, surgeons who had completed training prior to the MIS era adapted to perform MIS procedures without formal training. Our data also demonstrate that senior surgeons continue to perform the same procedures, including appendectomy, pyloromyotomy, fundoplication, and gastrostomy tube placement, at a constant rate, even as they move to an MIS approach. Senior surgeons in our group did perform a smaller percentage of the colectomies and lobectomies (lung), as these procedures more routinely were completed using MIS. However, those senior surgeons who continued to perform these advanced procedures adopted an MIS approach that their more junior partners were also using.
Previous work has focused on determining how many cases are required to attain competence for a given MIS procedure. It has been demonstrated in the literature that training required to reach proficiency is similar among both residents and attending surgeons, suggesting that adult learners acquire skills at the same rate, regardless of age. 18 Learning curves for common laparoscopic procedures, such as appendectomy, cholecystectomy, fundoplication, colectomy, herniorrhaphy, and splenectomy, have been reported to require 20–40 cases to reach proficiency.19–22 Pediatric surgery is somewhat limited by these numbers as many of these procedures are quite rare, even at high-volume tertiary referral centers such as Children's Hospital Colorado. At our institution, senior surgeons who trained in an era without MIS are now performing the majority of common operations using MIS techniques. Our data also support previous reports demonstrating that once a certain proficiency is reached in laparoscopic skills, these skills are then translatable to multiple surgical procedures. 23 This is likely true for our surgical group, with initial acquisition of basic MIS techniques occurring relatively slowly, whereas procedures that have only recently been performed using MIS demonstrating a quicker rise toward uniform use of MIS.
There are several limitations that should be considered when interpreting our data. This was a retrospective study using administrative databases. Our aim was to describe the trends in MIS use among a single surgical practice. We have not presented data regarding surgeon proficiency or time to operative proficiency for a given procedure. Our data instead aim to document a historical trend and provide a possible explanation for the trend. Despite these limitations, our data remain valuable as they document that the hiring of junior surgeons with MIS training was associated with an increase in adoption of MIS techniques by the entire surgical group.
Footnotes
Acknowledgments
We wish to thank Parish A. Burch BS, MSCIT, for his help in obtaining data from the operating room database.
Disclosure Statement
No competing financial interests exist.