
Abstract
Abstract
Purpose:
It is important to minimize surgical invasiveness in the therapy of patients with hepatocellular carcinoma (HCC), and consequently laparoscopic hepatic resection is widely performed. However, most anatomical resections, except left lateral sectionectomy, remain difficult technically, and laparoscopy-assisted procedures have been introduced as an alternative approach because of the safety and curative success of the operation. We reported previously pure laparoscopic subsegmentectomy of the liver using puncture of the portal branch under percutaneous ultrasound (US) with artificial ascites. Herein, we describe pure anatomical laparoscopic segmentectomy using the puncture method with indocyanine green (ICG) injection under laparoscopic US.
Patients and Methods:
Pure laparoscopic segmentectomy was planned for 2 patients with HCC of the liver. Identification of the segment was performed by ICG injection for optical imaging using near-infrared fluorescence under laparoscopic US guidance.
Results:
The procedures were completed successfully, and the postoperative courses were uneventful.
Conclusions:
Pure laparoscopic segmentectomy for HCC with a conventional puncture technique by ICG injection under laparoscopic US is considered to be a useful procedure featuring both low invasiveness and curative success.
Introduction
I
Laparoscopic hepatic resection is widely performed for HCC, and not only partial resection and left lateral sectionectomy, but also laparoscopy-assisted anatomical resection, such as a right or left hepatectomy, sectionectomy, and segmentectomy, may be performed.6,7 However, in the case of laparoscopic segmentectomy and subsegmentectomy, it is technically difficult to determine the portal vein territory by staining under intraoperative US. As an alternative approach, we made three-dimensional (3D) images preoperatively, based on multidetector computed tomography scanning, and performed segmentation or subsegmentation using workstation software. Then, we performed laparoscopy-assisted anatomical resection referring to the 3D images as simulated surgery. 8 Furthermore, we reported pure laparoscopic subsegmentectomy using puncture of the portal branch under percutaneous US with artificial ascites. 9
In this report, we devised a novel method for identification of a portal vein territory feeding the domain by indocyanine green (ICG) injection for optical imaging using near-infrared (NIR) fluorescence under laparoscopic US guidance, aiming at pure laparoscopic anatomical resection.
Patients and Methods
Case 1
A 78-year-old man was suffering from chronic hepatitis C and chronic renal failure. A physical examination was normal, but his liver function was somewhat poor (Child–Pugh Grade B), with total bilirubin of 0.3 mg/dL, albumin of 2.5 g/dL, prothrombin time of 97%, no ascites, and no hepatic encephalopathy. Abdominal plain computed tomography and magnetic resonance imaging showed a 3.5-cm HCC in segment 5 (S5) of the liver (Fig. 1). Considering the patient's age, comorbidity, liver function, and the location of the tumor, we planned laparoscopic segmentectomy of S5.
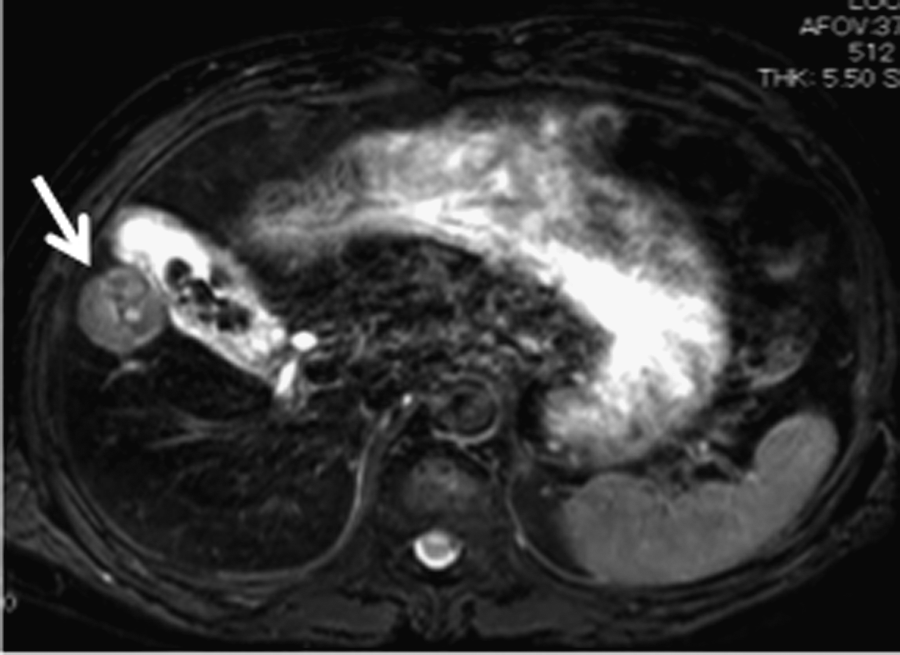
Abdominal magnetic resonance imaging showing a 3.5-cm-diameter hepatocellular carcinoma (arrow) in segment 5 of the liver.
Operative procedures of Case 1
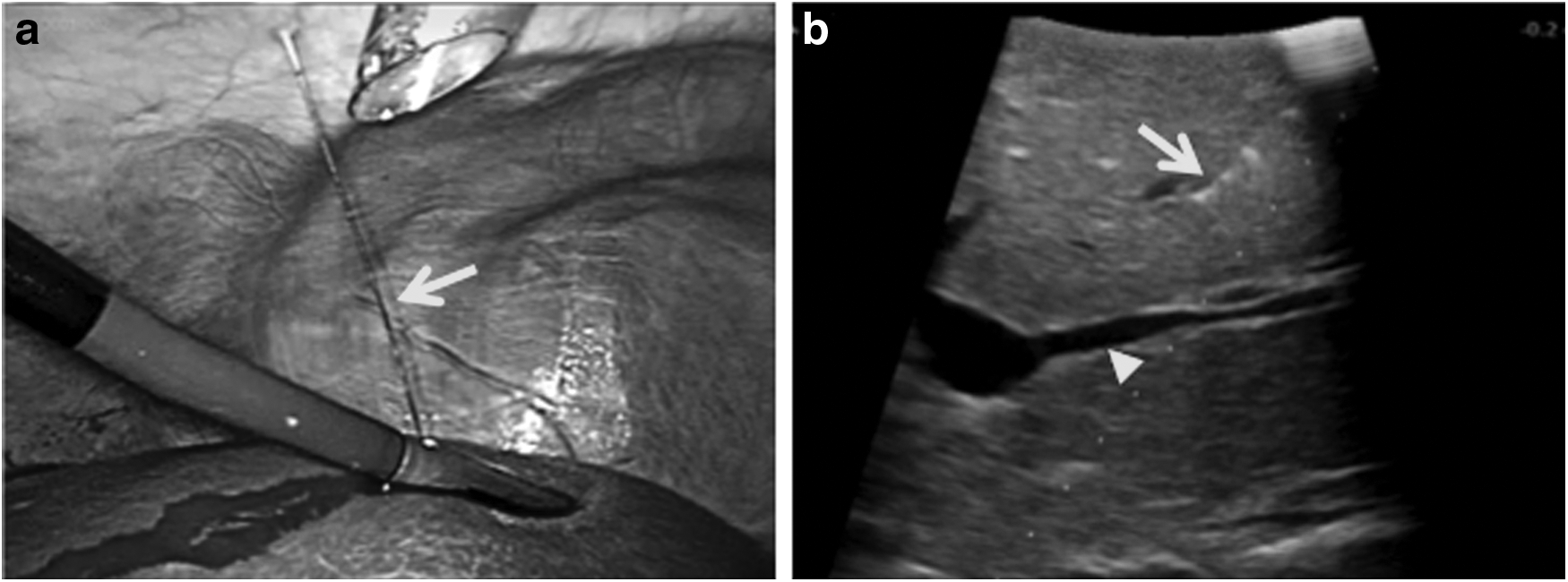
The patient's position was left half-lateral, and five ports were placed. Pneumoperitoneum was achieved with CO2, and the abdominal pressure was monitored and maintained at less than 12 mm Hg. Laparoscopic cholecystectomy was performed first, followed by laparoscopic US (Pro Focus Ultra View 2202; BK Medical, Herlev, Denmark) to identify and mark the tumor. The segmental portal branch of S5 was punctured with a 22-gauge needle (Create Medic Co., Ltd., Yokohama, Japan), which was introduced through the abdominal wall and a guide hole on the flexible laparoscopic US probe (laparoscopic transducer model 8666; BK Medical) (Fig. 2). One milliliter of ICG (DaiichiA Sankyo Co., Ltd., Tokyo, Japan) (5 mg/mL) was injected for optical imaging using NIR fluorescence without clamping the hepatic artery. One minute after injection, the area stained by ICG fluorescence was easily identified using a laparoscopic NIR ray camera system (IRI; Olympus, Tokyo) (Fig. 3a) and marked using electrocautery as a transection line (Fig. 3b).

One minute after injection of indocyanine green, the area of indocyanine green fluorescence was
Next, precoagulation was performed along the transection line using microwave energy, and the surface of the hepatic parenchyma was transected using laparoscopic coagulation shears (Harmonic Scalpel™; Ethicon Endo-Surgery, Cincinnati, OH). For deeper parenchymal transection, we used an ultrasonic dissector (CUSA Excel™; Integra Lifesciences Corp., Plainsboro, NJ) to identify intrahepatic structures such as hepatic veins and Glisson's pedicle. The exposed structures of 2 mm or less were dissected using EnSeal™ (Ethicon Endo-Surgery), and all sizable vessels were ligated with vessel clips. The specimen was extracted through an additional 2-cm umbilicalis incision using a plastic bag.
Case 2
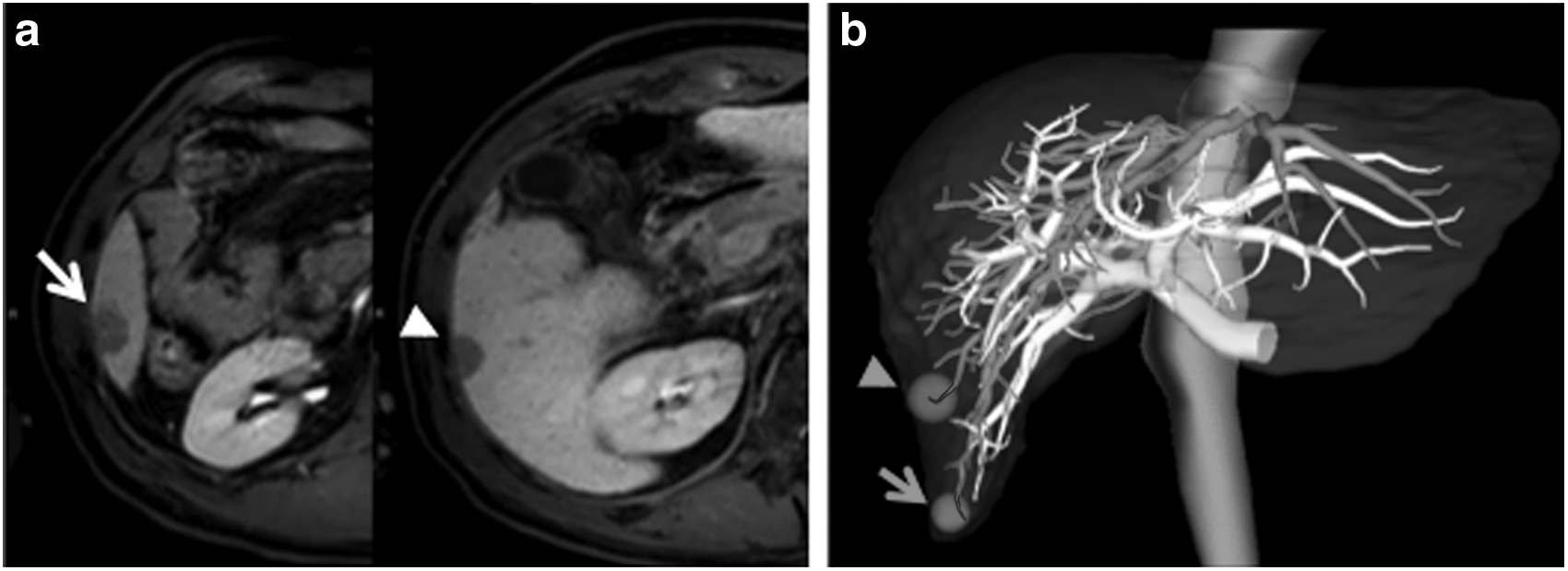
A 72-year-old man was suffering from chronic hepatitis C. A physical examination was normal, and the functional reserve of the liver was maintained comparatively (Child–Pugh Grade A), with total bilirubin of 0.8 mg/dL, albumin of 3.7 g/dL, prothrombin time of 96%, no ascites, and no hepatic encephalopathy. However, the platelet count (7.3×104/μL) was low, and activities of aminotransferase (aspartate aminotransferase, 47 IU/L; alanine aminotransferase, 65 IU/L) were elevated by chronic hepatitis. Abdominal computed tomography and magnetic resonance imaging showed 2-cm HCCs in S5 and segment 6 (S6) of the liver, respectively (Fig. 4a). The 3D images of the liver and two tumors were displayed using workstation software (Synapse Vincent; Fujifilm Corp., Tokyo), as shown in Figure 4b. One was located within S5, and another existed in the boundary of S5 and S6. Considering the patient's age, liver function, and tumor location, we planned laparoscopic segmentectomy of S5 and S6.
Operative procedures of Case 2
Five ports were placed with the patient in a left half-lateral position. The method of pneumoperitoneum was the same as for Case 1. Laparoscopic cholecystectomy was carried out, and then the right triangular ligament and the hepatorenal ligament were dissected. Laparoscopic US was performed in order to identify and mark the tumor. The segmental portal branches of S5 and S6 were injected with 2 mL of ICG (2.5 mg/mL) for optical imaging using NIR fluorescence under laparoscopic US guidance. One minute after injection of the ICG, the area of S5 (Fig. 5a) and S6 (Fig. 5b) was easily identified using a laparoscopic NIR ray camera system and marked using electrocautery as the transection line. The stained area was referred to the 3D image, and the anatomical relationship with the HCC also was verified (Fig. 6).
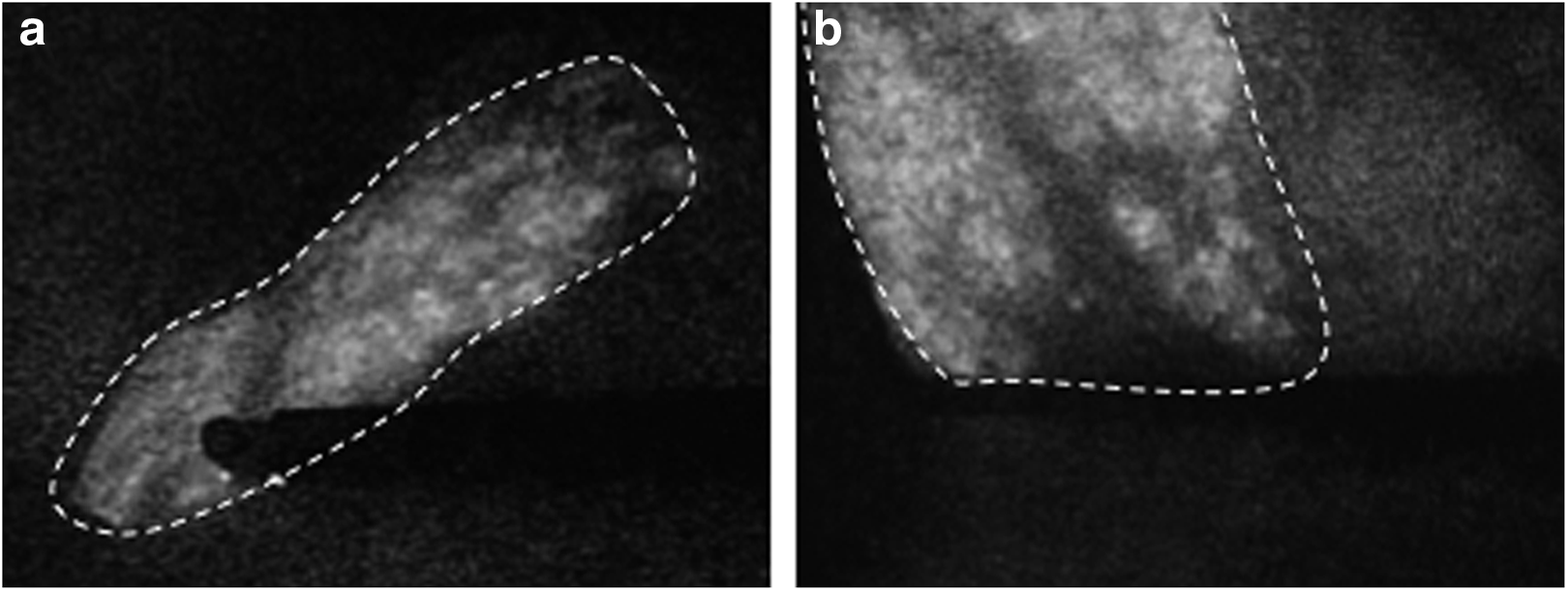
One minute after injection of indocyanine green, the area (white dotted line) of

The punctured (arrow and arrowhead) and stained areas of the portal branches were referred to the three-dimensional image, and the anatomical relationship with the HCCs also was verified (arrow, segmental portal branch of segment 5 [S5]; arrowhead, segmental portal branch of segment 6 [S6]).
Next, precoagulation was performed along the transection line using microwave energy. Hepatic parenchymal transection was performed using the same device and method as for Case 1. In Case 2, the Pringle maneuver (hepatic inflow occlusion time of 15 minutes and reperfusion time of 5 minutes) was performed during parenchymal transection. The specimen was extracted through an additional 2-cm umbilicalis incision using a plastic bag.
Results
The procedures of both cases were completed successfully. The operation time and intraoperative blood loss of Cases 1 and 2 were 320 minutes and 390 mL and 420 minutes and 620 mL, respectively. The postoperative course of Case 1 was uneventful, and the patient was discharged on postoperative Day 9. Although postoperative ileus was found in Case 2, the complication improved with conservative management, and the patient was discharged on postoperative Day 14.
Discussion
The beneficial effects of anatomical resection of HCC have been shown in terms of postoperative survival and disease-free survival,1–3 and our study also revealed that anatomical resection of a single HCC <3 cm in diameter was superior to nonanatomical resection or ablation therapies, in association with the overall and disease-free survival. 10 Therefore, even if such tumors are resected by laparoscopic surgery, anatomical resection should be considered for improving the surgical outcome. We also reported the value of laparoscopy-assisted anatomical resection in the case of a small HCC located in the right lobe border or the left lateral section. 8 In such cases, mobilization of the right liver was performed under pneumoperitoneum, and the segment was identified by staining with blue dye under intraoperative US through an additional small incision in the subcostal or intercostal region, as for conventional laparotomy.
When considering pure laparoscopic segmentectomy or subsegmentectomy, it seems that two issues may become problematic: the identification of the segment or subsegment and securing the parenchymal transection line. In parenchymal transection of the liver, a safe laparoscopic procedure can be developed using new instruments and devices.11,12
On the other hand, although there is a procedure for closing the Glisson's pedicle in order to determine the transection line, 13 this is technically difficult in a purely laparoscopic operation. Accordingly, we identified the segment with a nodule for pure anatomical laparoscopic segmentectomy using an artificial ascites technique for percutaneous US without an additional small incision. 9 However, percutaneous US is inferior to intraoperative US from the liver surface with respect to spatial resolution and the existence of a blind area.14,15 Therefore, we devised a method for the identification of a portal vein territory under laparoscopic US guidance, aiming at pure laparoscopic anatomical resection. Although it seems that the puncture of the portal vein under laparoscopic US guidance is difficult, development of laparoscope-related instruments is remarkable these days. The US probe used in this report has a hole to guide the puncture, so that puncture under laparoscopic US guidance is easily achieved. This method of puncture under laparoscopic US guidance is expected to have great value in laparoscopic hepatectomy, and additional devices may be required for the puncture of various other parts of the liver.
The ICG fluorescence imaging system was first used to perform sentinel lymph node biopsies in breast and colorectal cancer.16,17 Since then, it has received wide acceptance in various fields of surgical oncology and has become a valid diagnostic tool for guiding cancer treatment. 18 In the field of hepatic surgery, the ICG method was used for intraoperative detection of HCC or metastasis of colorectal carcinoma.19–21 Moreover, some authors have reported that ICG fluorescence imaging was useful for identification of the hepatic segment and subsegment during a laparotomic hepatectomy.22–24 The only reported experience regarding the use of ICG fluorescence imaging to identify hepatic segments during laparoscopic hepatectomy is a multimedia article published by Ishizawa et al. 25 Therein, the authors described injection of ICG into the portal branch of segment 4 or intravenously after clamping the segmental portal pedicle. In addition, puncture of the portal branch of S5 and S6 under laparoscopic US guidance was also possible in our experience. To our knowledge, this is the first report describing a novel technique for mapping a segment in the right liver using fluorescence imaging in laparoscopic liver surgery. Since the development of the laparoscopic US probe with a puncture guide and the laparoscopic NIR camera system, the method described in this report is possible and may be expected to be useful for pure laparoscopic anatomical hepatic resection, aiming at curability and low invasiveness.
For the precise puncture of the target portal vein, it is important to establish the anatomical relationship between the HCC and the surrounding structures preoperatively. Preoperative simulation using 3D images based on multidetector computed tomography is useful for identifying the anatomical relationship between the tumor and the portal branch and comparing the intraoperative staining area with the planned resection area. It seems that 3D simulation is essential for safe and accurate operation.
In conclusion, pure laparoscopic segmentectomy for small HCC using puncture of the portal branch with ICG injection, under laparoscopic US guidance, is considered to be a useful procedure to yield both low invasiveness and curative success.
Footnotes
Disclosure Statement
No competing financial interests exist.