
Abstract
Abstract
Aims:
To compare surgical outcomes for a simple purse string method of laparoscopic hernia (LH) repair with a traditional open inguinal hernia (OH) repair in children in a single center.
Materials and Methods:
Following ethical approval, a retrospective review of all children undergoing LH repair from January 2010 to December 2013 versus a historic cohort of all OH repairs between January 2010 and December 2011 was conducted. LH repair was performed by a simple purse string technique using nonabsorbable braided suture. Groups were compared using the independent t test or the Mann–Whitney test as appropriate.
Results:
One hundred three patients (23 females, 80 males) underwent LH repair over the 4-year period compared with 151 (25 females, 126 males) OH procedures in the first 2 years. Median age in the LH group was 0.56 years (range, 0.04–14.7 years) compared with 0.52 years (range, 0.04–13.47 years) in the OH group (P = .81). In the LH group the intended operation was bilateral in 18 (17.4%); 85 were clinically unilateral, but at operation a contralateral patent processus vaginalis was repaired in 26 (30.5%). Median operative time was 50.5 minutes (range, 20–95 minutes) in the LH group and 20 minutes (range, 10–90 minutes) in the OH cohort (P < .0001). Recurrence rate was 2.9% in the LH group and 3.9% in the OH group, and overall complication rates were 7.8% and 9.9%, respectively.
Conclusions:
LH repair yields similar results to OH repair; however, the operation time is significantly longer. All complication rates were statistically similar on balance. Almost one-third of LH procedures resulted in concurrent detection and repair of a contralateral patent processus vaginalis at laparoscopy.
Introduction
T
Materials and Methods
Following institutional ethical approval, a retrospective review of all children undergoing laparoscopic hernia (LH) repair from January 2010 to December 2013 versus a historic cohort of all open hernia (OH) repairs between January 2010 and December 2011 was conducted. The type of operation selected was purely by individual surgeons' preference, with the senior author performing all elective hernia repairs by LH repair and other members of the department reserving the technique for incarcerated or recurrent hernias. There was no patient and/or family preference; all patients presenting underwent the “randomly allocated” surgeon's preferred approach. Our service's age range includes preterm infants up to children 16 years of age, with no age limits on either approach. Only 2 patients were excluded from the study (both unstable premature neonates who had an open repair under spinal anesthesia). Hydroceles were considered a separate diagnostic entity and were not performed laparoscopically and therefore were not part of this study.
LH repair was performed by a simple purse string technique. In brief, an infraumbilical incision was made, a 5-mm port was inserted via a direct cut-down, and pneumoperitoneum was established to 5–10 mm Hg CO2 insufflation. Two further stab incisions were used for direct insertion of 3-mm or 5-mm instruments. Inspection of the contralateral ring was performed to decide on the need for contralateral closure. We defined a significant open contralateral ring as one through which the camera could be passed into the groin or one through which viscera could go through, or there was already obvious herniation. A purse string closure at the internal ring (avoiding the vas and vessels by picking up the peritoneum on either side of these structures and between them) was performed using 3/0 polyethylene terephthalate (Ethibond®; Ethicon, Somerville, NJ) suture (Fig. 1).
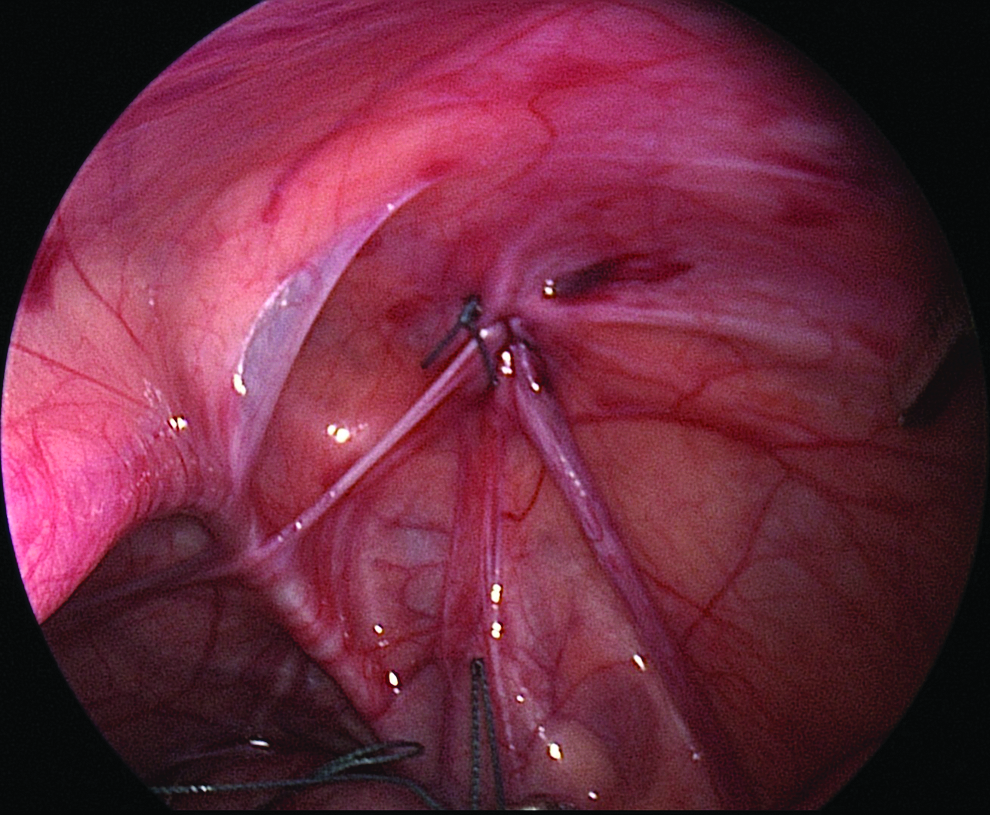
Laparoscopic view of the simple purse string repair.
Standard OH repair was performed via a groin crease incision through an external oblique window. The sac was dissected free of the vas and vessels up to the internal ring, transfixed with 3/0 polyglactin 910 (Vicryl®; Ethicon), and then divided.
Routine outpatient review was offered to patients after laparoscopic surgery at 3 months and then 1 year as it was initially a change in practice. Routine outpatient review was not offered after open surgery except in cases with intraoperative difficulty or in the preterm infants. Due to the regional service we provide, all patients with complications were seen back in outpatients, and these complications were captured on review.
Patient demographics were collected, and outcomes were compared, including operation time, length of stay, and complication rate. Groups were compared using the independent t test or the Mann–Whitney test as appropriate with a P value of < .05 deemed significant. The 95% confidence intervals are given.
Results
One hundred three patients (23 females, 80 males) underwent LH repair over the 4-year period compared with 151 (25 females, 126 males) OH repairs in the first 2 years. Median age in the LH group was 0.56 years (range, 0.04–14.7 years) compared with 0.52 years (range, 0.04–13.47 years) in the OH group (P = .81). The median weight in the LH group was 7.8 kg (range, 2–58.2 kg) compared with 7.6 kg (range, 2.06–48.4 years) in the OH group (P = .84). The median gestation in both groups was 35 weeks (range, 24–42 weeks). In the OH group there were 8 bilateral hernias and 143 unilateral, of which 3 had contralateral explorations. In the LH group the intended operation was bilateral in 18 (17.4%), and 85 were clinically unilateral, but at operation a contralateral patent processus vaginalis (PPV) was repaired in 26 (i.e., 30.5%). The median operative time was 50.5 minutes (range, 20–95 minutes) in the LH group and 20 minutes (range, 10–90 minutes) in the OH cohort (P < .0001). In unilateral cases the operative time in the open group was 25 minutes (range, 10–90 minutes) compared with 45 minutes (range, 20–95 minutes) in the laparoscopic group (P < .001). For bilateral repair the median operative time in the open group was 35 minutes (range, 20–70 minutes) compared with 64 (range, 27–90 minutes) in the laparoscopic group (P < .001). The number of trainee-led operations in the LH group was 42% compared with 80.1% in the OH group. No intraoperative complications were encountered during LH repair, and the procedure was well tolerated. Same-day discharge was possible in 56% who had LH repair and in 33% who had OH repair (P = .0002).
The median outpatient follow-up was 3 months in both groups but with a range up to 31.9 months in the LH group and 1 year in the OH group. In the LH group 16 patients had incomplete follow-up data as they were seen in peripheral outreach centers, and these clinic letters were not able to be reviewed; 5 patients were lost to follow-up as they failed to attend. The median follow-up period since the date of surgery until the current review was 3.86 years for both groups, and this is probably more representative as a follow-up time period given the catchment area and referral demographics (i.e., we have a relatively stable and nonmigratory population, and as such all complications and recurrences would come back to our single center). The comparative postoperative complications are shown in Table 1. The recurrences in the LH group occurred at 1 day and 5 months after repair. In the OH group they occurred at a mean of 197 days (range, 1–448 days) after repair. All laparoscopic repairs were redone laparoscopically. The findings at redo surgery were an open ring with the suture embedded in the tissues (presumed knot failure) in 2 cases and no visible suture in 1 patient in whom Vicryl was inadvertently used for closure. All except 2 cases of recurrent open hernia were managed by redo open surgery. The other 2 cases were redone laparoscopically. Overall there was no significant difference in postoperative outcome in terms of complications between the two groups.
CI, confidence interval; NA, not applicable.
Discussion
A recent randomized controlled trial published by the Helsinki group 12 aimed to answer the main controversies surrounding the debate of whether LH repair in children is a suitable alternative to traditional groin exploration and herniotomy. The trial concluded that the two procedures were similar in terms of surgical and cosmetic result but that laparoscopic repair involved longer operative time and an increased incidence of postoperative pain. The results of our series support the longer operative time, and in fact our median time of 50.5 minutes (range, 20–95 minutes) is longer than that reported by others—33 minutes by Koivusalo et al. 12 and 23 minutes by Chan et al. 13 —but this is most likely a reflection that a considerable number of LH procedures are performed by trainees learning the technique (40.7%).
Also, the exact operative time quoted in different articles varies; our operative time includes anesthetic time and is not “knife to skin” time and is therefore not accurate. There was no prospective aim to document operative times in either group, and therefore operative times are not accurate. In a retrospective review of the anesthetic charts only approximate overall operative time could be discerned.
It is also important to highlight that one-third of the patients explored for clinically unilateral hernias had a contralateral PPV repaired, and so allowing for this large number of bilateral operations, in fact the median operative time is similar to that in the literature.
In addition, despite longer operating times the majority of patients are discharged as day cases. This suggests that we do not have the same experience of increased postoperative pain, although we have not analyzed that specifically in our series. It would also be prudent to state that not all patients are treated with the intention of same-day discharge. Many patients with prematurity or associated morbidities are routinely kept overnight; therefore the individual patient demographics more often may determine the hospital stay. As this study is not randomized these confounding factors do no equate between groups.
It has long been debated among pediatric surgeons as to whether to perform contralateral groin exploration when faced with a clinical unilateral hernia. 14 LH repair allows the surgeon to clearly visualize the contralateral internal ring and to assess its patency laparoscopically. Hall et al. 15 tried to quantify this statistically and concluded that the probability of a contralateral PPV in an 8 month old was 50% (number needed to explore = 2), and it fell to 33% in a 4 year old (number needed to explore = 3) and to 25% (number needed to explore = 4) by 6 years of age. In our series one-third of the children were found to have an open contralateral internal ring; all were repaired with the same purse string method as for the clinically detected hernia. The reasoning for repairing these was based on the balance of risk and cost of developing a contralateral hernia and complications thereof against the risk of damage to cord structures during contralateral closure. The excellent visualization of the vas and vessels afforded by laparoscopy, along with the no touch technique of closure, minimizes the risk of cord damage. This is somewhat reinforced by our findings of no instances of testicular ascent and testicular atrophy in LH patients.
The debate still continues as to how many of these PPV cases would go on to develop a clinical hernia and how this varies with the age of the child. In the OH group there was an incidence of metachronous hernia of 4.3%. Interestingly, we found 1 patient in the LH group who developed a metachronous hernia. This was a 45-day-old term baby who had a right-sided hernia repaired and was thought to have a closed ring at the original laparoscopy. The rates of recurrence with LH vary in the literature from 1.13% to 3.1%.12–15 Our recurrence rate of 2.9% is in keeping with that found in the literature. The recurrence rate was higher (3.9%) in the cohort that had an open repair. This difference was not significant. Ein et al. 16 reported a recurrence rate of 1.2% incidence in 6361 infants and children; however, this reflects a personal series of repairs by a senior consultant. Conversely our series (both open and laparoscopic) included operations performed by trainees of all grades and could therefore be more representative of the overall outcome in the usual setting where operations performed under training and service provision.
There are different techniques reported in the literature to perform LH repair in children. These vary from combined percutaneous and endoscopic approaches such as the subcutaneous endoscopically assisted ligation or SEAL technique, 17 incising the hernia sac, 18 or purposeful traumatization of the internal ring to techniques to dissect the PPV from the underlying tissues with an injection technique. 19
Here we have shown that a simple purse string technique with a nonabsorbable braided suture is associated with a low risk of recurrence and injury. One patient had a recurrence after the use of Vicryl suture, and of note is that a recent animal study has shown a higher risk of recurrence in a rabbit model of pediatric inguinal hernia when absorbable nonbraided sutures are used. 20 Our experience would therefore reiterate the use of nonabsorbable suture in laparoscopic cases, as this combination of laparoscopic approach and nonabsorbable suture gives the same outcome as open repair. Due to the different surgical approach of a simple purse string closure without herniotomy (as is the case with the open procedure), the use of a nonabsorbable suture may allow for closure and success without the concomitant herniotomy in this situation. The occurrence of port-site hernia was an unexpected occurrence in 3 patients early in the series. This was despite direct closure of the sites. There has been none in the latter part of the series.
There are possible flaws with the findings of this study, including selection bias. However, we do not feel selection bias is a significant issue as patient allocation to surgeon is random, and as such so is the allocation to the method of repair. Furthermore, it is also assumed that all complications would be captured by this retrospective review, as by the nature of our service most complications would return to us as we provide the only pediatric service in locoregionally. The laparoscopic patients were offered routine follow-up to 1 year as this was a relatively new practice, and we were aiming to accurately determine postoperative complications in this group of patients. Therefore the complications in this group are a prospective collection of complications, and there were no obvious reasons why any complications should not have been collected. It is fair to assume that patients in the OH group will have presented with complications if they occurred.
In conclusion, there are various minimally invasive surgical approaches to pediatric inguinal hernia, and we suggest that LH repair performed as a simple purse string closure technique is one that can be effective and associated with a low complication rate and should be considered at least part of the pediatric surgeon's armamentarium. We have shown that the simple purse string method of LH repair yields similar results to OH repair in our series; however, the operation time maybe longer. All complication rates were statistically similar on balance.
Footnotes
Disclosure Statement
No competing financial interests exist.