
Abstract
Abstract
Introduction:
The published experience with minimally invasive techniques to treat injured children is currently small. In this multicenter case series, we aimed to characterize the contemporary role of minimally invasive surgery (MIS) in pediatric trauma.
Materials and Methods:
After obtaining Institutional Review Board approval at six pediatric regional trauma centers in the United States, a retrospective review was conducted on children who have undergone thoracoscopy or laparoscopy for the management of trauma over the past 13 years.
Results:
There were 200 patients with a mean age of 9.6±4.2 years, and 73% were male. Laparoscopy was performed for 187 (94%) and thoracoscopy for 8 (4%), whereas 5 (2%) patients had both, for a total of 205 MIS procedures. Conversion to open surgery occurred in 36% (n=73). Median operative time was 77 (range, 16–369) minutes. Of the 132 procedures completed without conversion, 81 (61%) were diagnostic, whereas the remaining were therapeutic, including the repair of bowel injuries (n=20), distal pancreatectomy (n=5), splenectomy (n=2), repair of traumatic abdominal wall hernias (n=2), evacuation of hemothorax (n=3), and other thoracoscopic or laparoscopic interventions (n=19). Procedures that required conversion were most commonly for bowel injury (n=56). Patients with peritonitis were most likely to require conversion to an open procedure (77.4%). Mean time to a regular diet was 4.2±8.6 days, and mean hospital stay was 6.3±6.5 days. Postoperative complications occurred in 19 patients, long-term sequelae in 10 patients, and permanent disability in 2 patients. There were no deaths or missed injuries.
Conclusions:
In the stable pediatric trauma patient, laparoscopy and thoracoscopy can be performed safely and effectively for both diagnostic and therapeutic purposes.
Introduction
M
Materials and Methods
After Institutional Review Board approval at each institution was obtained, data were collected, including patient demographics, mechanism of injury, indication for operative intervention, conversion to open procedure, complications, and postoperative course. Complications were defined as either postoperative events or morbidities requiring additional therapeutic intervention or operation or trauma-related re-admission. Descriptive analysis was performed. Means are expressed as ±standard deviation unless otherwise stated. MIS was defined as body cavity procedures to include laparoscopic procedures, laparoscopic-assisted procedures, and thoracoscopic procedures. Endoscopic and sigmoidoscopic/colonoscopic procedures were excluded.
Results
There were 200 patients with a mean age of 9.6±4.2 years, and 73% were male. Demographic data of the study cohort are shown in Table 1. Blunt trauma occurred in 60%, with the most common mechanism of injury being an all-terrain vehicle or motor vehicle crash (37%), with other mechanisms of injury listed in Table 2. Laparoscopy was performed for 187 patients (94%) and thoracoscopy for 8 patients (4%), whereas 5 (2%) patients had both, for a total of 205 MIS procedures. Conversion to open surgery occurred in 35% (n=72), although no additional procedure was necessary after conversion in 6 cases. Median operative time was 77 (range, 16–369) minutes.
CT, computed tomography.
Indications for the MIS approach as well as the percentage of cases converted to open surgery for each indication are outlined in Table 3. Patients with peritonitis and imaging suspicious for hollow viscus injury were most likely to require conversion to an open procedure (77.4% and 54.5%, respectively).
Includes completely laparoscopic and laparoscopic-assisted procedures.
Of the 132 procedures completed without conversion, 81 (61%) were diagnostic, whereas the remaining were therapeutic. An illustrative description of procedures performed in the study cohort is shown in Figure 1.
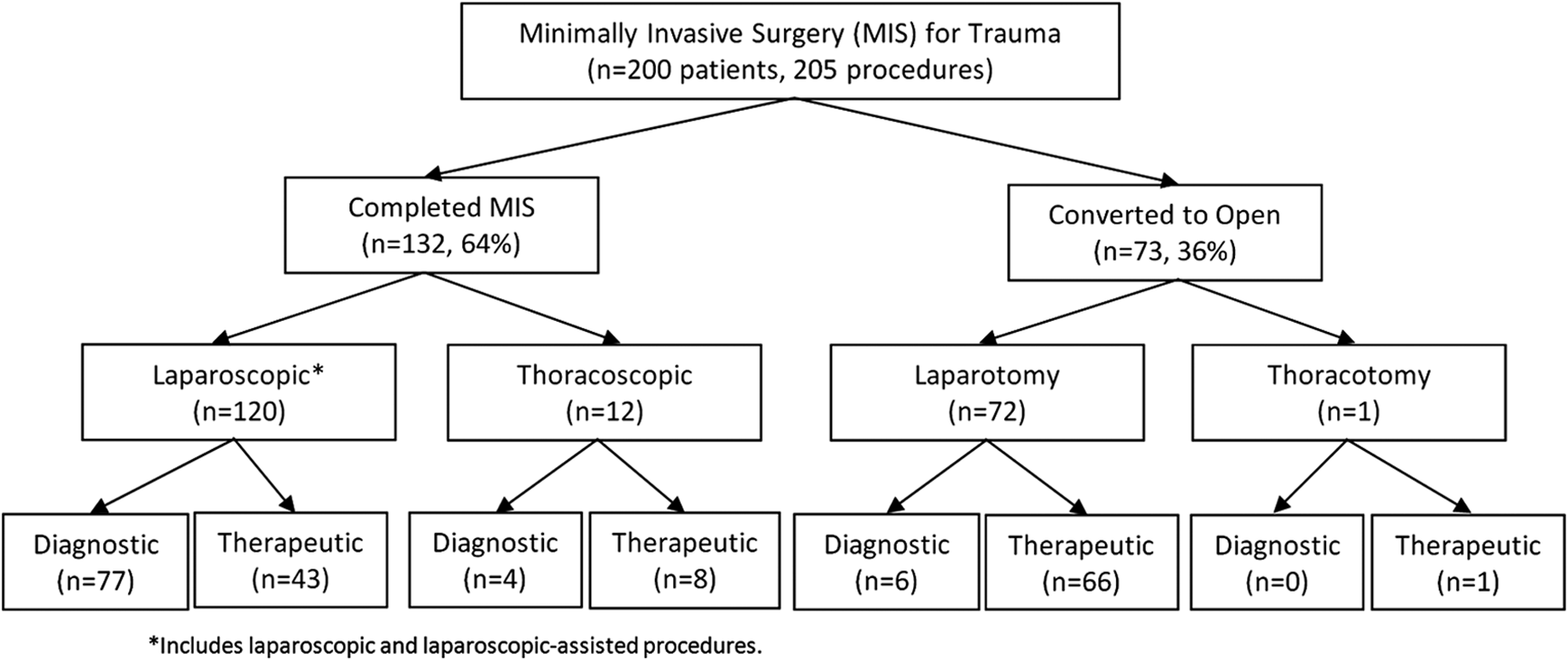
Breakdown of study group by procedure type.
Table 4 shows the spectrum of therapeutic MIS procedures. The MIS procedures listed as other include diverting colostomy, intraperitoneal drain placement after transanal rectal laceration repair, diaphragmatic rupture repair, removal of foreign bodies, repair of gastric injury, wedge resection of injured lung, etc. One patient had incomplete operative records indicating a laparoscopic procedure for pneumoperitoneum, but the details of the procedure were unclear. Procedures that required conversion were also most common for bowel injury (n=56); 74% of these required laparotomy. Various procedures that required conversion to open surgery listed as other in Table 4 include transthoracic repair of diaphragmatic defect not diagnosed preoperatively, repair of mesenteric tears, cholecystectomy and cholangiogram for gallbladder injury, repair of bladder injury, etc. Reasons for conversion included technical difficulty (n=69), hemorrhage (n=17), or hemodynamic instability (n=3), and some patients had more than one reason for conversion.
Includes completely laparoscopic and laparoscopic assisted procedures.
Mean time to a regular diet was 4.2±8.6 days, and mean hospital stay was 6.3±6.5 days. Median follow-up time was 1.2 months (range, 0.03–112 months), and 28% (n=55) patients were lost to follow-up. Complications occurred in 19 patients and are shown in Table 5. Long-term sequelae following their traumatic injuries occurred in 10 patients, and permanent disability was found in 2 patients. However, these were primarily related to their injuries and not the operative procedures. There were no deaths and no missed injuries.
Discussion
The traditional standard for trauma laparotomy is a midline incision from the subxiphoid to the suprapubic region. This approach continues to be the standard of care for unstable trauma patients. However, algorithms for the inclusion of MIS in penetrating and blunt abdominal trauma in children have been proposed.11,14 These algorithms can be extrapolated to include thoracic trauma as well. Despite these proposed treatment algorithms, the literature describing the use of MIS in children remains limited, being primarily based on case reports and small series.5–13
This study provides a contemporary representation of current MIS applications in pediatric trauma, with far more cases than previously reported. We found that MIS was used successfully as a diagnostic tool to exclude an injury in 61% of the 132 successfully performed procedures, corresponding to 40% of the study population. In this same cohort, MIS therapeutic interventions were successfully performed in 51 patients.
This study underscores the utility of MIS as a diagnostic tool in patients with equivocal findings on physical exam and imaging studies. Laparoscopy and thoracoscopy can be an extension of the physical exam. In patients with a penetrating injury, MIS has been shown to be an excellent adjunct to diagnose fascial violation. 16 The concern in patients with both blunt and penetrating abdominal trauma remains hollow viscus injury, which can be difficult to diagnose preoperatively11,17 and can have significant morbidity if the diagnosis is delayed or missed. 18 Direct peritoneal lavage is no longer used as laparoscopy typically provides complete assessment of the intraperitoneal cavity and offers therapeutic capabilities. Despite diverse mechanisms of injury, MIS was used successfully to exclude an injury requiring further intervention in 61% of procedures completed minimally invasively and 40% of all procedures attempted minimally invasively. Only in 6 of the 192 minimally invasive procedures (3%) was laparoscopy inadequate to exclude an injury, and a subsequent nontherapeutic laparotomy was performed. This corresponds to MIS preventing negative laparotomy or thoracotomy in 40% of the study population, a rate that is similar to two previous smaller studies in children.11,12
As a diagnostic tool, the rate of a missed injury with laparoscopy in the adult literature is reported at 1%–3%.16,19 The pediatric trauma literature reports a 0% missed injury rate,11,12 which is replicated in this series. Our study further substantiates the effectiveness and accuracy of MIS in the evaluation of pediatric trauma patients.
As a definitive interventional procedure, laparoscopy and thoracoscopy were used to accomplish the therapeutic goals of the procedure in 51 cases, which corresponds to 43% of the overall number of therapeutic procedures. These minimally invasive therapeutic procedures centered primarily on repair of bowel injuries, which has been well described in pediatric trauma patients, 10 but also included a wide variety of other procedures indicating the versatility of MIS for selected trauma patients.
Conversion to laparotomy or thoracotomy was performed in 35% of cases, primarily for technical reasons. Most of the repairs performed after conversion were related to bowel injury. Seventy-four percent of patients requiring bowel resection or repair of enterotomies or serosal tears were converted from laparoscopy to laparotomy. The size of the incision after laparoscopy, however, can be much smaller than that for a trauma laparotomy because other sites of injury have been explored and excluded so the incision can be tailored to the problem. Preoperative peritonitis, imaging suspicious for hollow viscus injury without clinical signs, and pneumoperitoneum were the most frequent predictors of the need to convert to an open operation. Overall, MIS was successful in excluding injury or diagnosing injury and in completing therapeutic intervention in 65% of cases.
A major limitation of this study is its retrospective nature and lack of a comparative primary open surgery cohort. Without a comparison group of open surgery patients, we are not able to analyze if patients undergoing MIS have improved pain scores, improved cosmesis, shorter hospital stays, lesser narcotic requirements, shorter operative times, or shorter return to school/activities. Presumably, the advantages of MIS that have been reported with pyloromyotomies, cholecystectomies, and numerous other operations would be similar for trauma patients.
The lack of data regarding pediatric trauma admissions from all centers over the study period prevents us from having a better view of which trauma patient should undergo MIS. Future studies need to further define the advantage of MIS in pediatric trauma patients as well as which patients benefit the most from an MIS approach.
This large multi-institutional series demonstrates that, in the stable pediatric trauma patient, laparoscopy and thoracoscopy can be performed safely and effectively for both diagnostic and therapeutic purposes.
Footnotes
Disclosure Statement
No competing financial interests exist.