
Abstract
Abstract
Background:
Although single-incision laparoscopic (SIL) ileal pouch-anal anastomosis (IPAA) has been shown to be feasible and safe, outcomes have not been compared with the standard laparoscopic-assisted (LA) procedures. The purpose of this study was to compare the two techniques in children with chronic ulcerative colitis (CUC) and familial adenomatous polyposis (FAP).
Subjects and Methods:
Children ≤18 years of age who underwent SIL and LA IPAA between 2000 and 2013 at our institution were identified. Patient information was obtained retrospectively from patients' medical records and compared between approaches. Results for operative time and postoperative length of stay were stratified by number of stages (one, two, or three), and postoperative complications were stratified by diagnosis (CUC or FAP).
Results:
Children who underwent SIL IPAA (n=19) and LA IPAA (n=62) were not significantly different in age, gender, diagnosis, anti-tumor necrosis factor-α antibody use, staged approach, and stapled versus mucosectomy with hand-sewn anastomosis. SIL and LA IPAA had equivalent operative times for two- and three-stage procedures, but operative time for one-stage procedures was shorter with SIL (308 versus 355 minutes; P<.001). Median length of stay was shorter following SIL for all patients (4 versus 7 days; P<.001) and, specifically, for two-stage patients (4 versus 6 days; P=.009). There were no significant differences in complications between SIL and LA.
Conclusions:
SIL IPAA is a safe alternative to LA IPAA for children with CUC or FAP and may reduce postoperative length of stay without affecting short-term postoperative morbidity. Additional studies are needed to determine if there are long-term benefits.
Introduction
T
Subjects and Methods
Following Institutional Review Board approval of this study, all children ≤18 years of age who underwent LA or SIL IPAA between 2000 and 2013 were identified from a prospectively maintained database of surgical procedures at our institution. Patients with Crohn's disease or those who underwent open IPAA were excluded; however, prior to 2010, it was the practice at our institution to use the LA approach in all patients when feasible. Following introduction of the SIL approach in 2010, surgeon preference rather than patient characteristics dictated choice of SIL versus LA IPAA. One surgeon preferentially used the SIL approach on all elective patients, whereas the others decided on a case-by-case basis.
Patient demographic, preoperative, operative, and postoperative information was collected retrospectively from medical records using a standard data collection form by one of the physician authors. Outcomes were operative time, postoperative length of stay, and postoperative complications. Complications studied were unplanned return to the operating room, unplanned re-admission, wound infection or dehiscence, pelvic abscess, anastomotic leak, revision of IPAA, ileostomy complications including obstruction, small bowel obstruction unrelated to ileostomy, and portal vein thrombosis. Unplanned return to the operating room and re-admission excluded planned or routine ileostomy closure, exam under anesthesia, and pouchoscopy.
Technique
Both SIL and LA IPAA were performed in one, two, or three stages, with three-stage procedures reserved for patients with fulminant colitis, transfusion-dependent bleeding, or recent high-dose corticosteroid or anti-tumor necrosis factor-α antibody exposure. One-stage IPAA was performed on patients not receiving immunosuppression; thus, these were mainly FAP patients. Our technique for SIL IPAA has been previously reported. 10 In brief, SIL access was in the right lower quadrant at the site of the future ileostomy. If no ileostomy was planned, the umbilicus was used for SIL access. Mobilization of the colon and division of mesentery and greater omentum proceeded in a right to left fashion. The pouch was constructed extracorporeally. The LA approach was performed by laparoscopic mobilization of the colon and division of the mesentery followed by proctectomy and stapled ileal pouch creation through a low transverse (Pfannenstiel) incision. Four to five ports were used: one in the umbilicus, one in the right lower quadrant at the future ileostomy site, one at either end of the future Pfannenstiel incision, and one in the hypogastric region. Ports were typically 5 mm, although 10- or 12-mm ports were sometimes used in the umbilicus or at the site of the future ileostomy. IPAA was completed by either stapled anastomosis or rectal mucosectomy with hand-sewn anastomosis. Mucosectomy was preferred in patients with FAP; otherwise, the anastomotic technique was by surgeon preference. In select patients, no Pfannenstiel incision was used, and the procedure was entirely laparoscopic. A 12-mm port was required in these patients for pouch construction and specimen removal.
Statistical methods
Patient demographic, preoperative, operative, and postoperative information was collected retrospectively from medical records and compared between SIL and LA IPAA using t tests for continuous variables and chi-squared tests for categorical variables. Fisher's exact tests were used when n≤5. Postoperative length of stay was reported as a median value and was compared between SIL and LA using the Wilcoxon rank sum test. Outcomes of operative time and length of stay were stratified by number of stages (one, two, or three), and complications were stratified by diagnosis (CUC or FAP). Operative time was reported in minutes as mean (standard deviation). Complications that were studied included unplanned return to the operating room, unplanned re-admission, anastomotic leak, pelvic abscess, revision of IPAA, wound infection or dehiscence, small bowel obstruction, ileostomy complications, portal venous thrombosis, pouchitis, and pouch failure. Pouchitis was defined as at least one episode of clinical symptoms including, but not limited to, increased stool frequency, urgency, or incontinence that were improved with antibiotics or histologic evidence of pouchitis on pouch biopsy. 11 Duration of follow-up was determined by date of IPAA and date of last clinician visit at our institution. All analysis was completed using JMP software (SAS Institute, Cary, NC). Statistical significance was acknowledged when P<.05.
Results
In total, 81 consecutive children underwent IPAA for CUC or FAP; 19 were SIL, and 62 were LA. Median (interquartile range) follow-up after SIL IPAA was 1.3 (0.8, 3.0) years, and that following LA IPAA was 4.2 (1.4, 7.5) years. There was no significant difference in age or gender based on approach, and the distribution of one-, two-, and three-stage procedures was similar (Table 1). A one-stage approach was used more frequently in patients with FAP than CUC (85% versus 10%), and a three-stage approach was used more frequently in patients with CUC (34% versus 0%; P<.001). An accessory 5-mm port placed in the umbilicus was used in 53% of SIL procedures. Use was concentrated in the earlier patients, and an accessory port was not used in the last 5 patients. A low transverse Pfannenstiel incision was used in 87% of LA procedures. Hand-sewn IPAA with mucosectomy was more frequent in both SIL and LA approaches (56% versus 58%; P=.91). CUC was the reason for IPAA in 73% of patients who underwent SIL IPAA and 79% of those who underwent LA IPAA (P=.77). Of patients with CUC, mean duration of disease (3.2 versus 2.8 years; P=.57) and preoperative exposure to biologics (33% versus 27%; P=.74) were similar between SIL and LA approaches; however, use of corticosteroids was more frequent prior to LA IPAA (67% versus 27%; P=.014). Two patients who underwent LA IPAA required conversion to open IPAA, but no SIL patients required conversion to LA or open approaches. All patients with an ileostomy proceeded to closure with a median time to ileostomy closure of 2 (1.5, 3.0) months.
IPAA, ileal pouch-anal anastosmosi; LA, laparoscopic-assisted; SD, standard deviation; SIL, single-incision laparoscopic; TNF-α, tumor necrosis factor-α; UC, (chronic) ulcerative colitis.
Operative time and length of stay
There was no significant difference in overall operative time (333±65 versus 365±91 minutes; P=.09) (Fig. 1). When stratified by number of stages, operative times for one-stage SIL IPAA were significantly shorter than for LA (308±14 versus 355±65 minutes; P=.013). Operative times were similar between approaches for two- (353±81 versus 386±81 minutes; P=.32) and three- (316±50 versus 339±134 minutes; P=.60) stage procedures. Postoperative length of stay was shorter following SIL than LA for all patients (4 versus 7 days; P<.001) and, specifically, for patients who underwent two-stage IPAA (4 versus 6 days; P=.009) (Fig. 2). Following one- (9 versus 9 days; P=.70) and three- (3 versus 3 days; P=.44) stage procedures, length of stay was similar between approaches.
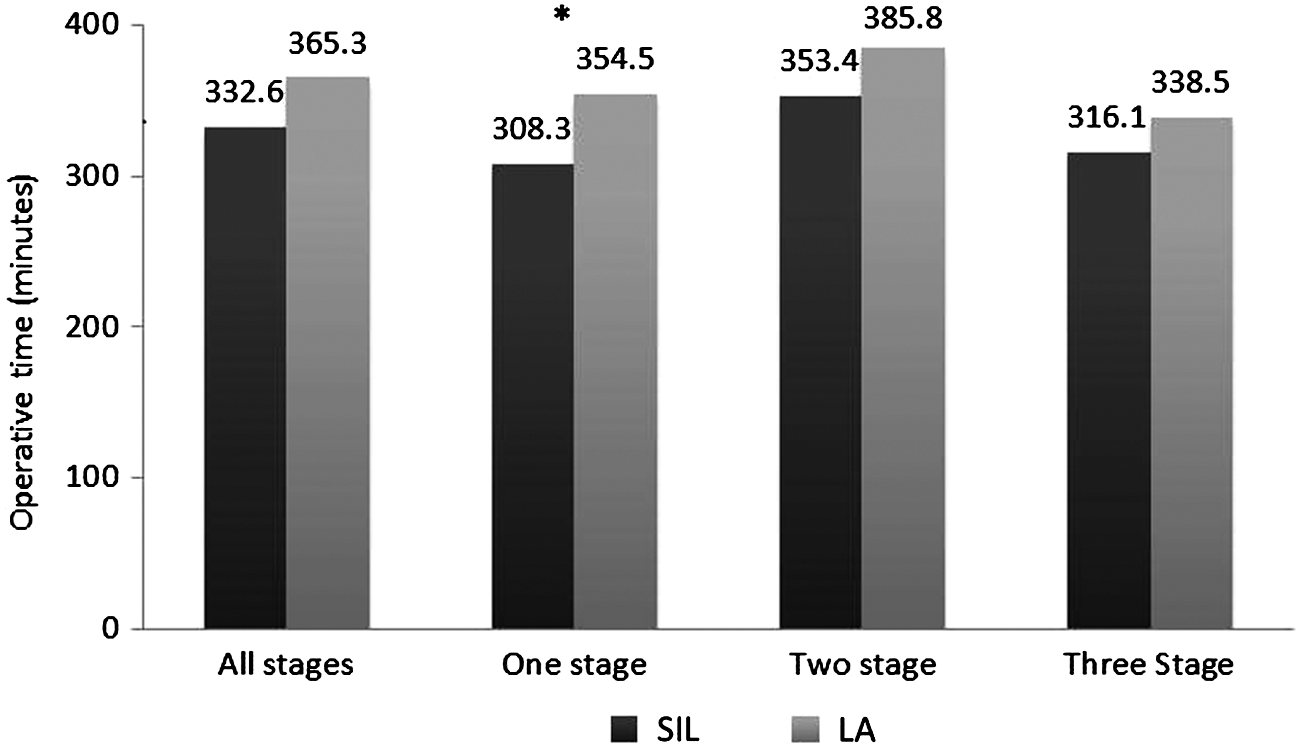
Operative time (minutes) is compared between single-incision laparoscopic (SIL) and laparoscopic-assisted (LA) approaches for one-, two-, and three-stage ileal pouch-anal anastomosis procedures. *Indicates statistically significant difference.
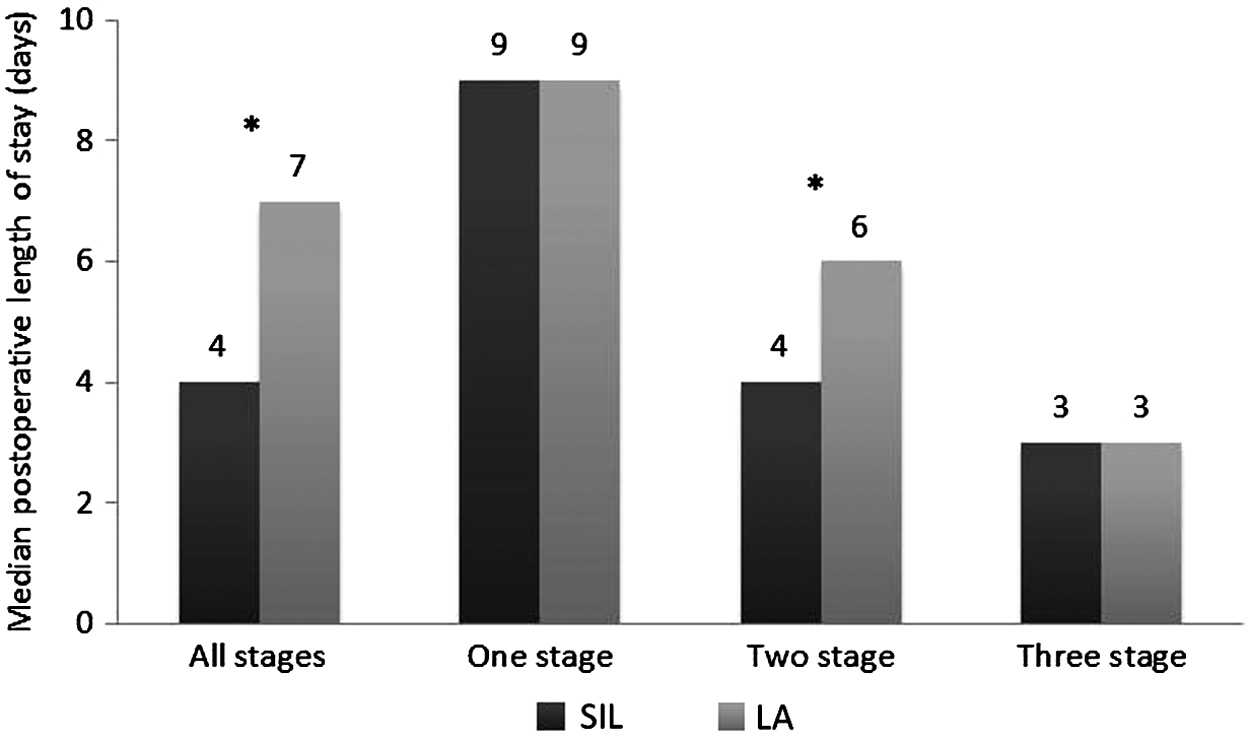
Postoperative length of stay (days) is compared between single-incision laparoscopic (SIL) and laparoscopic-assisted (LA) approaches for one-, two-, and three-stage ileal pouch-anal anastomosis procedures. *Indicates statistically significant difference.
Postoperative complications
Postoperative complications occurred in 44% of all children who underwent IPAA, and there was no significant difference between SIL and LA (28% versus 48%; P=.18). When stratified by diagnosis, there were no differences in the overall complication rate between SIL and LA IPAA for both CUC (29% versus 51%; P=.22) and FAP (25% versus 41%; P>.99). Rates of individual complications, including unplanned return to the operating room, bowel obstruction, pelvic abscess, anastomotic leak, or revision of IPAA, were similar between approaches; however, these results are limited by small sample size (Table 2). One patient who underwent a one-stage SIL procedure and 1 patient who underwent a one-stage LA procedure suffered anastomotic leaks, which were treated by revision of IPAA and diverting ileostomy, both of which were later closed.
FAP, familial adenomatous polyposis; IPAA, ileal pouch-anal anastomosis; LA, laparoscopic-assisted; SIL, single-incision laparoscopic; UC, (chronic) ulcerative colitis.
Pouchitis occurred in 60.0% of all patients and was similar between SIL and LA (50.0% versus 62.9%; P=.33). Pouchitis was more frequent in patients with CUC than FAP (76.3% versus 14.3%; P<.001) and in patients who underwent two- or three-stage IPAA versus one-stage IPAA (72.4% versus 70.0% versus 36.0%; P=.013). The risk of pouchitis was not influenced by duration of follow-up (P=.10). Pouch failure occurred in 5 (6.2%) patients with a mean (range) time to failure of 3.8 (1.2–5.6) years. All five failures occurred in patients with CUC who underwent LA IPAA in one (n=2) or two (n=3) stages. The risk of pouch failure was influenced by duration of follow-up (P=.034) and not surgical technique. Of note is that three of the five pouch failures occurred in patients who developed Crohn's disease in the postoperative period based on histologic findings of pouch biopsies or the presence of fistulae.
Discussion
As technology evolves, SIL pediatric surgery is being performed more often and for more procedures. In addition to demonstrating feasibility and safety of these novel techniques, they need to be compared with standard laparoscopic techniques to ensure that outcomes are not inferior and to identify potential benefits of single incision approaches. Proctocolectomy with IPAA is the surgical standard of care for pediatric FAP and CUC, and a SIL approach to this procedure has been shown to be safe and effective. 1 When compared with a standard LA approach to IPAA in this study, SIL IPAA was found to have similar outcomes and several potential benefits, including shorter operative time for one-stage procedures and shorter length of stay. Additionally, no patients in whom SIL IPAA was attempted required conversion to LA or open IPAA, and no intraoperative injuries occurred. This is the first report to compare SIL versus LA IPAA in the pediatric population.
It is important to consider operative time as an outcome of a novel surgical technique to ensure that increased technical complexity does not result in significantly longer procedures for children. Because LA IPAA was shown to have longer operative times than open IPAA in children and single-incision appendectomy has been associated with increased operative time when compared with standard laparoscopic techniques, this was particularly of concern.5,12,13 We found that operative times were similar between SIL and LA IPAA and that, in one-stage procedures, SIL was associated with shorter operative times. Decreased postoperative length of stay is also a theoretical benefit of SIL procedures, as there are fewer incisions. The results of this study support this benefit in part, as overall length of stay was shorter following SIL IPAA. When stratified by number of stages, the improvement in length of stay was limited to two-stage patients only. It is possible that improvement in other aspects of hospital care and increased emphasis on earlier discharge over time contributed to the shorter length of stay in SIL patients. Thus, our study demonstrates that SIL IPAA is not inferior to LA in terms of operative time and postoperative length of stay and may be superior in select patients.
Proctocolectomy with IPAA in children has a high complication rate, reported to be from 30% to 60% in the literature.14–16 Although we were unable to study long-term morbidity following SIL IPAA, we found that short-term postoperative morbidity was equivalent to that of LA IPAA overall and when stratified by diagnosis. The results of this study demonstrate that the postoperative leak and pelvic abscess rates are not higher following SIL IPAA. Wound complications were equivalent between approaches despite fewer incisions in SIL patients. These findings are consistent with existing literature comparing SIL and LA appendectomy, which also reports no difference in complications between approaches.12,17,18 The risk of small bowel obstruction and pouch failure also was not different between approaches in this study; however, longer follow-up of SIL patients is needed to make definitive conclusions. Pouchitis was equivalent between approaches, with rates in both SIL and LA patients consistent with what is reported in the literature.16,19 The sample size and relatively short follow-up period for SIL patients precluded conclusions regarding the risk of pouch failure following SIL versus LA IPAA in this study, as the risk of pouch failure was associated with duration of follow-up. Although all five pouch failures occurred in LA patients, this was not significant, and longer follow-up of SIL patients is needed to determine the risk of failure. Nonetheless, it is reassuring that no pouch failures occurred following this novel technique thus far.
There is always concern, when comparing outcomes of two surgical techniques, that patients were preferentially chosen for one technique or the other based on perceived suitability by the surgeon. In this study, patients who underwent SIL versus LA IPAA were similar in terms of age, gender, diagnosis, utilization of staged procedures, and utilization of a stapled IPAA. Additionally, patients with CUC were similar in terms of recent exposure to biologic therapy and duration of disease. Therefore, we feel that selection bias, while inherent to retrospective studies, contributed minimally to the results of this study.
The results of this study should be interpreted with its limitations in mind. Although patients were identified from a prospectively maintained data source, clinical information was obtained retrospectively. Because a laparoscopic approach (SIL or LA) to IPAA was the preferred approach at our institution since the start of the study period, unless there were special circumstances, patients who underwent open IPAA were not included. Furthermore, selection bias may have been introduced, as the choice of approach and number of stages was surgeon-dependent. The relatively recent introduction of SIL approaches precluded comparison of long-term morbidity, including chronic pouchitis and pouch failure, between approaches in this study. Similarly, the rate of bowel obstruction was likely underestimated because of the short duration of follow-up. This study did not evaluate differences in cosmetic results and patient satisfaction, which is a theoretical benefit of SIL procedures and proven benefit of single-incision appendectomy in children. 20 Lastly, the small sample size after stratification by number of stages and diagnosis precluded multivariable analysis of the impact of the SIL versus LA approach on outcomes.
To conclude, this study reports the largest series of SIL IPAA procedures in children and is the first to compare outcomes with standard LA IPAA. The results found SIL IPAA to be a safe alternative to LA IPAA in children with CUC or FAP, as outcomes were not inferior. In select patient groups, SIL was associated with shorter operative time and length of stay. Future directions for the study of SIL IPAA in children include evaluation of cosmetic results and long-term risk of bowel obstruction and pouch failure.
Footnotes
Disclosure Statement
No competing financial interests exist.