
Abstract
Abstract
Aims:
Reinforcement of the staple line is one of the most debated technical aspects concerning laparoscopic sleeve gastrectomy (LSG). Different buttressing methods have been proposed and demonstrated to be effective in reducing the incidence of staple line bleeding, although data concerning their effort on staple line leakage are not consistent. The aim of this study was to ascertain the technical feasibility and to report the preliminary outcomes of laparoscopic use of platelet-rich plasma (PRP) to reinforce the staple line during sleeve gastrectomy.
Patients and Methods:
From March 2012 to May 2012, 20 patients were prospectively enrolled (10 females; mean age, 44.6±11 years; mean body mass index, 42.3±5.45 kg/m2). Type 2 diabetes mellitus was present in 4 patients, obstructive sleep apnea syndrome in 3, and hypertension in 6. LSG was performed using a 48-French bougie and gold cartridges; reinforcement of the staple lines with buttressed materials or oversewing the suture was performed excluding the last cranial cartridge. PRP was prepared by separating the platelets from autologous blood withdrawn on the same day of surgery, in order to obtain a membrane with cylindrical shape (2×5 cm) formed by fibrin and active platelets. The membrane is introduced through the 10-mm trocar and placed at the upper portion of the staple line. The overall cost for the preparation of PRP is about €15.
Results:
No intraoperative complications and conversions have been recorded during the surgical procedures. No deaths occurred. The mean operative time was 85±31 minutes, which was not significantly increased compared with the operative time of the surgeon's overall personal series (750 cases). At 12 months of follow-up the abdominal ultrasound was negative for collections, and upper contrast showed no images indicating gastric leaks. In no case did PRP induce symptoms of rejection, infection, or adverse events.
Conclusions:
The use of PRP during LSG is feasible, does not increase significantly the operative time, does not require any special devices, and is cost effective. A larger cohort of patients is needed to ascertain the potential effectiveness of PRP in the prevention of postoperative staple line complications.
Introduction
S
In recent years a growing trend has emerged in relation to the use of autologous blood products to facilitate the healing process in a variety of surgical applications. This remarkable advance is due to the better understanding of the wound healing process, in particular regarding platelets, which release many growth factors (GFs) involved in the tissue regeneration. Platelet-rich plasma (PRP) is by definition a portion of the plasma fraction of autologous blood, which also has a three- to sevenfold increased concentration of platelets and a 7–30-fold increased concentration of GFs, compared with whole blood. Thus, when applied topically, PRP releases a supraphysiological quantity of GFs, which allows a jump start to enhance the healing process.17–20
The aim of this article is to assess the feasibility and the safety of autologous PRP application during LSG as a reinforcement of the upper edge of the staple line in a preliminary experience with 20 patients.
Patients and Methods
From March 2012 to May 2012, at the Policlinico Umberto I, “Sapienza” University of Rome, Rome, (Italy), 20 patients were prospectively enrolled (10 females; mean age, 44.6±11 years; mean body mass index, 42.3±5.45 kg/m2). The study was approved by the local ethics committee. After complete metabolic and psychological study, the patients underwent LSG. In this group of patients the PRP was used to reinforce the upper part of the suture line. Patients with previous bariatric surgery were excluded from the study. Other exclusion criteria were anemia (hemoglobin, <10 g/dL) and thrombocytopenia (platelets, <120×103/μL). Comorbidities were distributed as follows: type 2 diabetes mellitus in 4 patients (20%), obstructive sleep apnea syndrome in 3 patients (15%), and hypertension in 6 patients (30%). In 6 patients a concomitant procedure was performed: cholecystectomy in 2 cases, hiatoplasty in 3, and excision of gastrointestinal stromal tumor placed at the gastroesophageal junction in 1 case. After the operation the patients were followed up for a minimum of 1 year. At 1, 6, and 12 months postoperatively, an abdominal ultrasound and X-ray swallow were performed to exclude late leaks and abdominal collections.
Surgical technique
The patient, with pneumatic compression boots, is positioned in the 30° anti-Trendelenburg position with legs abducted. Five trocars are used. The division of the vascular supply of the gastric greater curvature starts at 6 cm from the pylorus and proceeds upward to the angle of His and is performed with radiofrequency (Harmonic Scalpel™; Ethicon Endo-Surgery, a Johnson & Johnson Company, Cincinnati, OH) or with LigaSure™ vessel sealing (Valleylab™, Boulder, CO) devices. The complete mobilization of the gastric fundus, with meticulous dissection of the posterior gastric wall, is accomplished. The sleeve gastrectomy is created using a linear stapler (Echelon™ Endopath; Ethicon Endo-Surgery) with gold cartridges. The stapler is applied alongside a 48-French calibrating bougie. The resection line was performed avoiding the “critical area” by resecting the fundus 1.5 cm from the angle of His. A methylene blue dye test is routinely performed at the end of the procedure in all cases. A gastric remnant of 60–80 mL in volume is obtained. Reinforcement of the staple lines with buttressed materials or by oversewing the running suture is performed until the last cranial cartridge. In 3 patients hiatal hernia repair was performed with the LSG; crural repair was performed by means of two or three interrupted nonabsorbable polypropylene (Prolene®; Ethicon US, LLC, Somerville, NJ) stitches. 21 Drains are not routinely placed, and the nasogastric tube is removed at the end of the procedure. Upper gastrointestinal contrast (diatrizoate meglumine and diatrizoate sodium solution [Gastrografin®; Bracco Diagnostics, Monroe Township, NJ]) study was performed on the first postoperative day.
PRP preparation and application
In order to prepare PRP, whole blood (60–75 mL) was collected in a syringe preloaded with 2–7 mL of anticoagulant no more than 2 hours before surgery. After collection, the whole blood sample underwent differential centrifugation by a gradient cell separator machine. The first centrifugation spin (160 g for 6 minutes) separates low-platelet concentrated plasma from red blood cells and PRP. In the second spin (1500 g for 10 minutes), the PRP is separated from the platelet-poor plasma, and it is collected at the bottom of the test tube because of its high specific gravity. From the initial blood draw, there is approximately 15–20 mL of PRP available with a platelet count of 1×106/μL±20%. A cell control is carried out on PRP and on the platelet-poor plasma.
The PRP is placed in sterile tubes (about 8 mL per tube) with 2 mL of calcium gluconate (ratio 4:1) and 1 mL of 95% ethyl alcohol. The product is centrifuged at 1500 g for 35 minutes. The result is a membrane with cylindrical shape (2×5 cm) formed by fibrin and active platelets. The membranes have a solid and elastic consistency with suturable, cuttable, and malleable properties (Fig. 1). The overall time to complete the PRP-membrane preparation is about 1 hour, and the cost for the whole procedure is about €15.
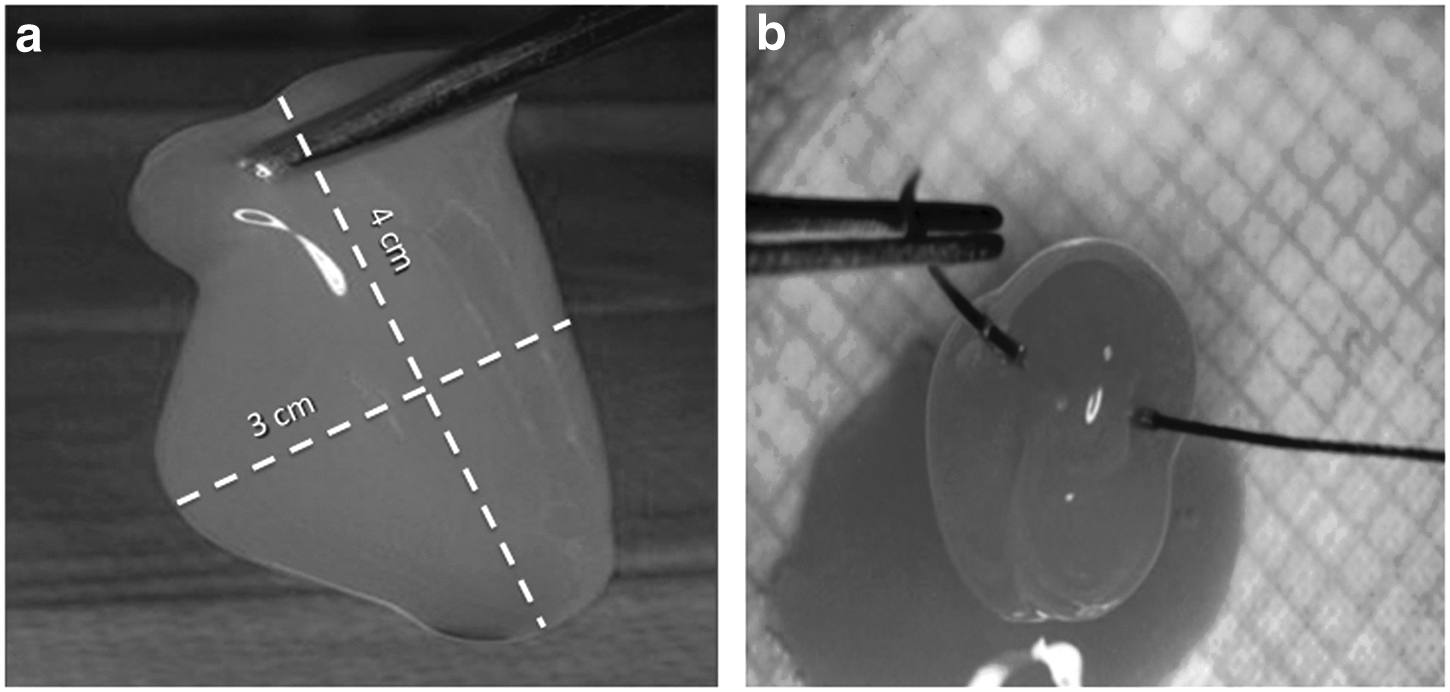
During the operation, the membrane is introduced through the 10-mm trocar wrapped in a layer of oxidized cellulose polymer (Surgicel®; Ethicon) used as support. The PRP is placed at the upper portion of the staple line, adjacent to the last firing, and fixed with two clips (Fig. 2).
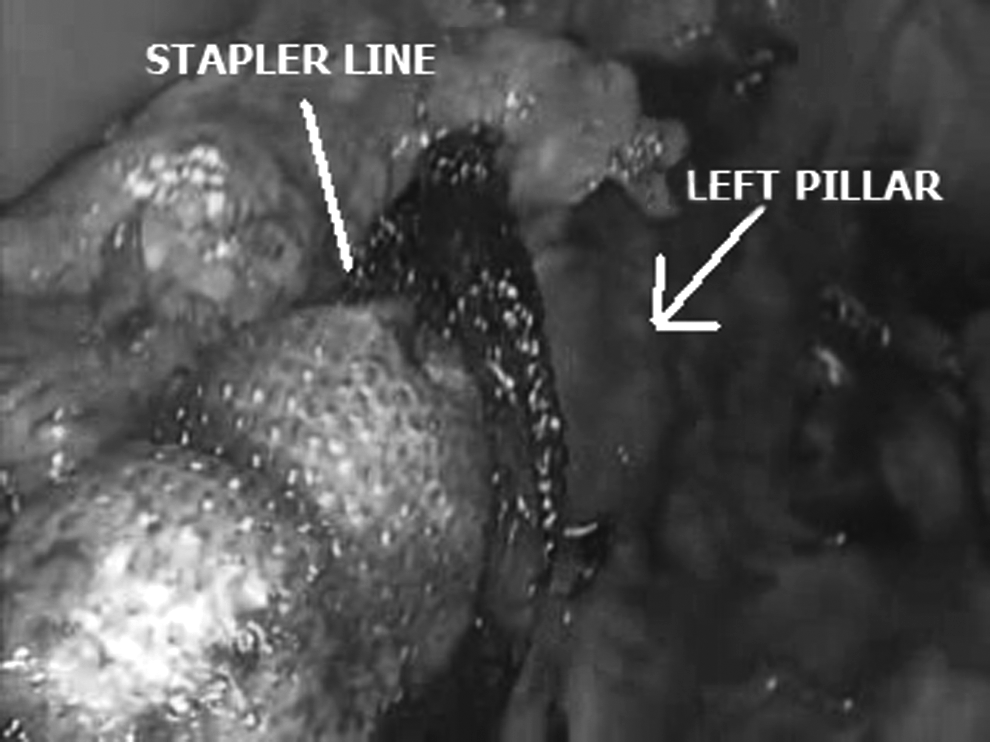
The platelet-rich plasma was placed at the upper portion of the staple line, in a layer of Surgicel used for support.
Results
Twenty patients were subjected to LSG. No intraoperative complications and conversions have been recorded during the surgical procedures. There were no deaths. The mean operative time was 85±31 minutes, which is not significantly increased compared with the operative time of the surgeon's overall personal series (750 cases). The application of the membrane/PRP was feasible and easy in all cases. The intraoperative methylene blue dye test and the early postoperative upper gastrointestinal series performed in all patients were negative for staple line leaks. Mean hospital stay was 5±2 days. At follow-up, the abdominal ultrasound was negative for collections, and upper contrast showed no images indicating gastric leaks. A temperature of <38°C was reported in 1 patient in the first 5 postoperative days without leukocytosis and any radiological sign of abdominal abscess or infection; the fever disappeared after 3 days of antibiotic therapy per os (ampicillin/sulbactam).
At 12 months of follow-up no cases of leak were observed. In no case did PRP induce symptoms of rejection, infection, or adverse events.
Discussion
Staple line–related complications can severely affect the postoperative course of patients operated on with LSG; their management is usually conservative, although a surgical approach can be sometimes required.11,22–24 As these complications often result in a prolonged hospital stay and significantly increased costs, in recent years several different techniques have been adopted to reinforce the staple line during LSG, trying to reduce the incidence of staple line bleeding and/or leak. 24 Actually, the main options consist of oversewing the staple line with a running or inverting absorbable suture, buttressing the staple line with different materials such as glycolidetrimethylene carbonate copolymer (Gore Seamguard®; W.L. Gore & Associates, Inc., Flagstaff, AZ), bovine pericardium strips (Peri-Strips Dry® and PSD Veritas®; Synovis Surgical Innovations, St. Paul, MN), or porcine small intestinal submucosa (Surgisis® Biodesign®; Cook Medical, Inc., Bloomington, IN), and, finally, covering the staple line with fibrin glue (Tisseel® fibrin sealant; Baxter, Deerfield, IL) or hemostatic agents (Floseal® hemostatic matrix; Baxter).
Although SLR is advocated by most authors, the debate concerning its role in reducing the incidence of staple line–related complications is still unsolved. Published data show that SLR reduces the incidence of staple line bleeding after LSG, whereas none of the different reinforcement methods has been demonstrated to play a main role in the prevention of staple line leak.13–16 During the International Sleeve Gastrectomy Expert Panel Consensus Statement, held in Florida in March 2012, with a collective experience of more than 12,000 LSG procedures performed, most surgeons considered it acceptable to reinforce the staple line with buttressing materials or oversewing the suture (95% and 77%, respectively) in order to prevent the development of staple line–related complications. However, although all the panelists agreed that SLR reduces the incidence of staple line bleeding, reinforcing the staple line to prevent the development of gastric leak was considered advisable but not mandatory, owing to the lack of large clinical trials assessing its effectiveness. 25
Aurora et al., 8 in a systematic analysis involving 4888 LSGs, recorded a 2.4% rate of leak, with an increased risk in patients with a body mass index of >50 kg/m2 than in those with a body mass index of <50 kg/m2 (2.9% versus 2.2%; difference not significant). In 92% of patients, the leak was located at the esophagogastric junction, and in most cases it developed after hospital discharge (>10 days after surgery). SLR did not affect the incidence of leak, although a significant decrease of gastric fistula occurred when LSG was tailored with a ≥40-French bougie. 8 These results were consistent with those reported in a systematic review and meta-analysis by Parikh et al., 10 including almost 10,000 patients subjected to LSG; the incidence of leak (2.2%) was not affected by SLR, whereas it was significantly reduced when a ≥40-French bougie was used. In 2009 Chen et al. 26 published a review of the literature involving 1539 LSGs; additionally, they described their experience with Peri-Strips and Seamguard in a series of 35 patients. Clinical outcome did not support statistically the use of buttressing materials, as the leak rate in patients who received SLR was 1.45 times that in patients without reinforcement (difference not significant). So the authors concluded that a larger cohort of patients was necessary to assess the effectiveness of SLR. 26 Choi et al., 14 in a meta-analysis including 1335 LSGs, evaluated the impact of SLR on the overall complication rate after LSG and, separately, on the incidence of gastric fistula and bleeding; analysis of the collected data showed that SLR did not significantly reduce the rate of leak and bleeding.
More recently, Dapri et al. 15 randomly compared patients subjected to LSG without SLR versus patients in whom the staple line was reinforced with Gore Seamguard or with suturing. A reduction of intraoperative blood loss was reported, although there were no significant differences in terms of postoperative leaks among the three techniques.
The use of hemostatic agents and sealants in different bariatric procedures has been successfully reported in large multicenter, randomized studies concerning the use of fibrin glue during laparoscopic gastric bypass, with a significant reduction of the incidence of complications in the fibrin glue group. Because of the great diffusion of LSG, the use of hemostatic agents to reinforce the staple line is under investigation; Gentileschi et al. 13 compared three different SLR techniques: covering the staple line with Floseal, buttressing with Gore Seamguard, and oversewing. The first technique has been demonstrated to be safe like the latter ones and cost-effective, with no significant differences concerning the incidence of staple-related complications.
In our personal experience of 750 LSGs, the overall incidence of staple line leak is 3%. As time has passed, the staple line has been reinforced by means of oversewing adsorbable suture (running or inverting) or buttressing materials (Gore Seamguard, Peri-Strips Dry, and PSD Veritas). We have observed a reduction of the incidence of staple line leak, although not statistically significant, when the latter have been used.
PRP is an autologous concentration of platelets in concentrated plasma, which has been extensively used for over three decades in order to promote soft and hard tissue healing and to significantly reduce wound healing time.19,20 The use of PRP is still validated in several surgical branches (periodontal and oral, maxillofacial, orthopedic, plastic, spinal, and cardiac) and in the management of diabetic wounds and burns.27–38 The significance behind its use refers to the abundance of GFs stored in platelets, which enhance the quality of wound healing and reduce healing times by expediting tissue regeneration. In particular, platelet-derived GF, transforming GF, vascular endothelial GF, insulin-like GF, platelet-derived angiogenic factor, and epithelial GF play key roles in the healing process.18,20 Current methods of PRP preparation allow us to obtain a platelet enrichment of 300%–700%; thus, when compared with whole blood, a 7-fold increase in transforming GF, a 30-fold increase in platelet-derived GF, and a 10-fold increase in epithelial GF have been reported in PRP. 20 In addition, platelet-derived chemokines and cytokines also play a main role in the healing process recruiting inflammatory cells (macrophages and natural killer cells), vascular endothelial cells, and stem cells at the trauma site. Thus PRP functions as a topical tissue sealant and drug delivery system, and its use presents a great similarity to the natural healing processes, with the simultaneous application of a high concentration of multiple GFs. In addition, GFs may be more effective when directly delivered through a “depot” platelet plug, allowing their slow release, than when administered in a bolus dose. 39
Several animal models have been proposed to assess the physiopathological effects of PRP.40–43 Bir et al. 44 investigated its angiogenic properties in a murine model of hind limb ischemia by means of laser Doppler perfusion imaging and the measurement of capillary and mature vessel density. They demonstrated that the injection of PRP in the ischemic site improved significantly all of these parameters when compared with the administration of saline solution (control group). Moreover, they reported a significant increase of the angiogenic effect when PRP was administered in a sustained form instead of solution form. In the former, in fact, GFs and cytokines are immobilized in a hydrogel vehicle; thus, after the injection, they are gradually released as a result of the hydrogel degradation.
Two interesting experimental studies concerning the effects of PRP on the healing process of intestinal anastomosis have been published by Yol et al. 45 and Yamaguchi et al. 46 In the former study, 30 rats were divided into three groups on the basis of operative technique: colonic anastomosis only, colonic anastomosis with topical PRP application, and colonic anastomosis with fibrin sealant application. 45 After 2 weeks the rats in the PRP group demonstrated a significant increase of the anastomosis bursting pressure as well as in the levels of the tissue hydroxyproline (index of collagen metabolism), compared with the other two groups. Furthermore, histopathological examination of the anastomotic site revealed a beneficial effect of PRP over fibrin sealant on fibroblast development, production of rich collagen, and reduction of inflammatory cell infiltration. The latter study confirmed these results, although the authors claimed the concentration of PRP as a key factor on its pathophysiological effect. 46 In fact, although the healing process of murine intestinal anastomosis was significantly improved after the administration of low-concentrated PRP, high-concentrated PRP administration resulted in an impaired anastomotic bursting pressure and a reduction of hydroxyproline tissue levels.
About 90% of gastric fistulas after LSG occur at the esophagogastric junction, and they can have an early (first postoperative days) or delayed (1 or more weeks after surgery) presentation. 8 Whereas the former is related to the failure of the mechanical stapler, in the latter the initial physiologic process of healing can be impaired. In particular, the dissection of gastric fundus, in order to perform an adequate “fundectomy,” could cause the ischemia of the gastric wall at the esophagogastric junction, where a “critical area” of vascularization may occur. The blood supply impairment, associated with the increased intraluminal pressure of the tubulized stomach, can lead to the development of staple line leaks. 9
The rationale for using autologous PRP as a SLR technique at the esophagogastric junction is to prevent the impairment of the healing process of the staple line and to enhance it through the topical delivery of a high concentration of GFs and other platelet-derived factors. Although for this specific field of application animal models are not described in the literature, Brady et al. 47 in 2006 reported the use of PRP during bariatric surgical procedures in 10 patients undergoing laparoscopic gastric bypass with reinforcement of gastrojejunostomy, jejunojejunostomy, and the stomach's staple line using platelet gel. None of the patients experienced staple line–related complications, namely, leaks or bleedings. Thus the authors concluded that PRP might replace the use of fibrin sealants because the former provides a larger number of GFs than the latter, and it is obtained from the patients' own blood by means of a cheap and rapid process.
Our initial experience shows that autologous PRP is feasible during the laparoscopic procedure and safe, with no adverse reactions recorded at a follow-up of 12 months, and cheaper than other SLR methods such as buttressing materials, with a cost of only €15 for each LSG. Initially, PRP placement may be time consuming, requiring about 15 minutes to be completed, but the learning curve can be easily overcome. Even if preliminary clinical outcome concerning the incidence of staple-related complications are encouraging, a larger cohort of patients is necessary to define whether autologous PRP could be part of the repertoire of the bariatric surgeon for the prevention of staple line bleeding and leak.
Footnotes
Acknowledgments
The authors would like to thank Dr. Roberta Maselli, Dr. Giorgio Di Rocco, Dr. Domenico Giannotti, Dr. Gregorio Patrizi, Dr. Francesca Frangella, and Dr. Maria Giulia Bernieri for their contribution to our work.
Disclosure Statement
No competing financial interests exist.