
Abstract
Abstract
Background:
To report the preliminary experience of laparoscopic radical nephrectomy (LRN) in children with Wilms' tumor (WT) and renal cancer.
Patients and Methods:
From January 2010 to October 2013, the medical records of 7 cases of WT or renal cancer in children treated by LRN at two medical centers in China were reviewed.
Results:
All the patients were treated by LRN, and 3 of them underwent preoperative chemotherapy before surgery. The biggest tumor size was 10 cm without crossing the lateral edge of the vertebra at the time of operation. The median hospital stay was 8.5 days (range, 6–11 days). The pathologic investigation showed 5 cases of WT, 1 case of rhabdoid tumor, and 1 case of renal cell carcinoma. With a median follow-up of 1.9±1.5 years (range, 0.3–2.9 years), six children were in complete remission, and the remaining one was lost to follow-up. None of these patients presented evidence of oncological complications (tumoral recurrences, port-site implantation, or secondary lung metastases), and no small bowel obstruction occurred.
Conclusions:
LRN for WT and renal cancer may be considered as an option in selected children. Preoperative chemotherapy is to decrease tumor size and to facilitate the dissection, avoiding tumor rupture. For trained laparoscopic surgeons, the eventual indication of LRN is the tumor not crossing the midline. A long follow-up and more cases are necessary to evaluate the results of the laparoscopic approach.
Introduction
T
The purpose of this work is to review the preliminary experience of LRN for renal malignant tumors in children from two children's medical centers in China, to describe the laparoscopic technique, the results, and the postoperative evolution, and to evaluate the feasibility of this minimally invasive approach.
Patients and Methods
Patient selection for laparoscopic surgery
From January 2010 to September 2013, seven children (five boys and two girls) with a unilateral renal neoplasm underwent the LRN procedure at the Shanghai Children's Hospital of Shanghai Jiao Tong University and the Children's Hospital of Fudan University (Shanghai, China). The patients had a mean age of 4.3 years (range, 1.5–10 years) and a mean weight of 17.5 kg (range, 9.5–31 kg). Four patients had a tumor in the right kidney, and 3 had a tumor on the left side. The medical records about clinical findings, renal function, abdominal ultrasonography, and chest and abdomen computed tomography scans (Fig. 1), the laparoscopic techniques, operative time, hospitalization, complications, pathology, cosmetic results, and follow-up were retrospectively collected. The criteria for selection in our study for LRN were the tumor size at the time of surgery without crossing the midline, as well as absence of renal or cava thrombus.3,6 The initial symptoms were abdominal pain (n=5), hematuria (n=2), and abdominal mass (n=3).
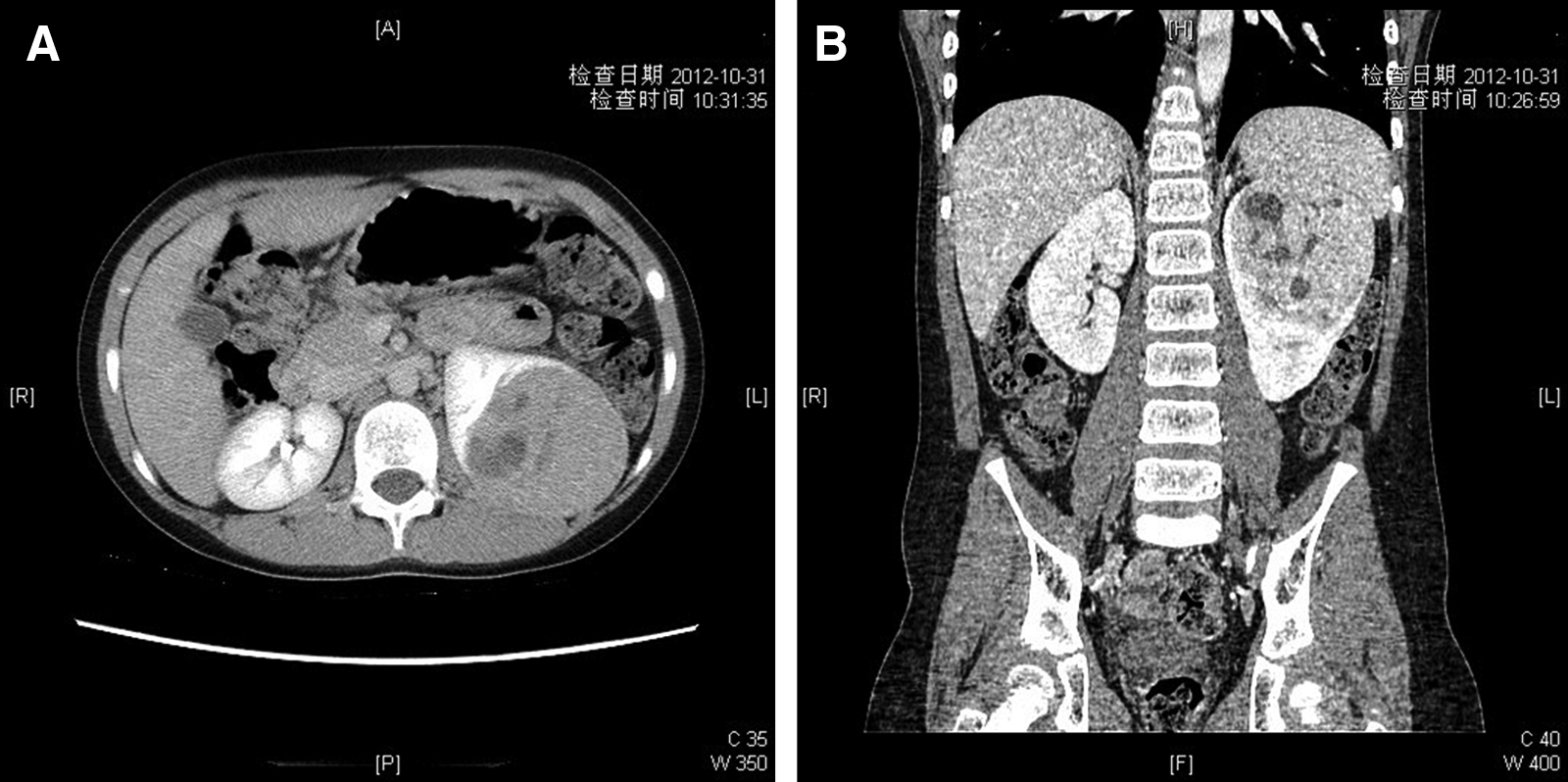
Preoperative computed tomography scan in a patient.
LRN was performed initially in 4 patients without preoperative chemotherapy or biopsy. When they were admitted to the hospital, 3 patients were advanced cases and presented with a tumor size crossing the lateral edge of the vertebra, and 1 patient had suspected lung metastases. Based on the histological confirmation by percutaneous fine-needle biopsy, 7 these patients underwent 4–8 weeks of chemotherapy consisting of vincristine, actinomycin D, and doxorubicin. Then the patients were reevaluated with abdominal and thoracic computed tomography to assess the reduction in tumor size and disappearance of focus in the lung. Subsequently these 3 cases underwent LRN.
The biggest tumor size at the time of surgery, with or without neoadjuvant chemotherapy, was 6.8±2.5 cm (range, 4.5–10 cm) in diameter without crossing the midline. Renal tumors were located as follows: two in the upper pole, four in the lower pole, and one in the medial part of kidney. All the children had normal hepatic and renal function when laparoscopy was performed.
Surgical technique
All patients underwent a transperitoneal approach under general anesthesia, and an orogastric tube and urinary catheter were inserted. The patient was positioned in 45° lateral decubitus with the side of interest up. The operating surgeon, assistant, and scrub nurse were positioned on the contralateral side of the tumor.
A 12-mm port for the scope was placed at the umbilicus with an open technique. Two other 5-mm working ports were placed subcostally in the anterior axillary's line and in the iliac fossa. The abdominal insufflation pressure with CO2 was 10–12 mm Hg.
The surgery was started by complete inspection of the abdominal cavity, especially on the vena cava and retroperitoneal lymph node.5,6,8 LRN was initiated by opening the peritoneum on the outside of the colon to the level of the hepatic or splenic flexure and carried around to the transverse colon to expose the retroperitoneal structures. The colon was released down. A silk stay suture or a fourth port was needed to retract the spleen or right lobe of the liver if the space was not enough for exposure. The ureter was isolated along the psoas muscle up to the level of the renal hilum using hook electrocautery. Then the ureter could be retracted by the stay suture to expose the renal hilum. The anterior surface of the vena cava and aorta was cleared of overlying lymphatic and soft tissue until up to the level of the renal vein, and then the renal artery was divided. The involved renal artery and vein were ligated with Hem-o-lok® clips (Weck® Closure Systems; Teleflex®, Research Triangle Park, NC) sequentially. The dissection of retroperitoneal lymph nodes was performed using a combination of Harmonic® scalpel (Ethicon Endo-Surgery, Cincinnati, OH) electrocautery. 9 The adrenal gland was removed at the same time in the case of an upper pole tumor if necessary. Finally, the stay suture was released, and the ureter was divided down to the level of the bladder and ligated using vascular clips (Fig. 2).
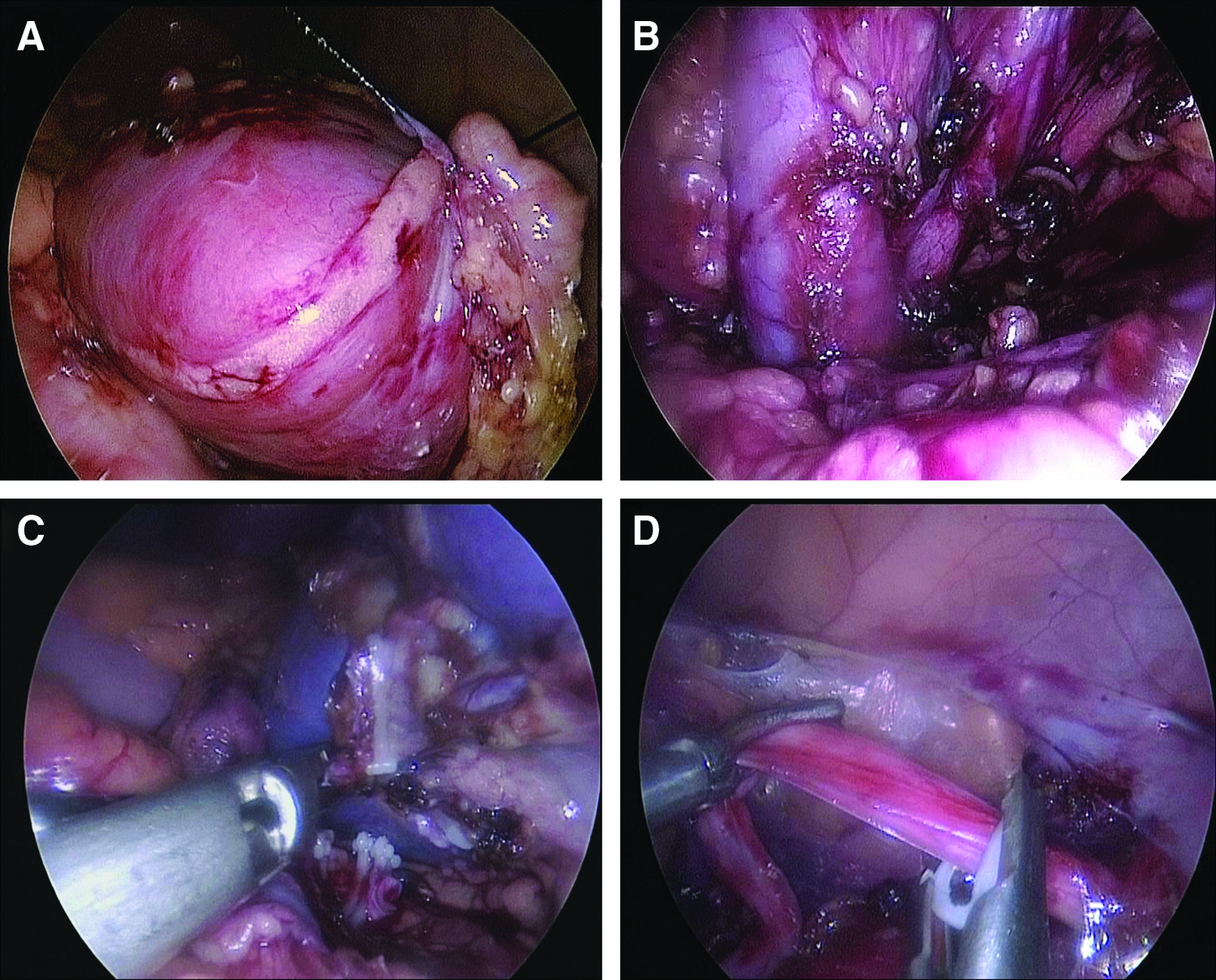
Intraoperative images and trocar position for laparoscopic radical nephrectomy.
A 10-mm EndoCatch II™ (US Surgical Corp., Norwalk, CT) specimen pouch was deployed intracorporeally. The resected tumor, the lymph node, and retroperitoneal tissue were completely entrapped in the bag. The transumbilical incision was lengthened 3 or 4 cm depending on the wall thickness of the patient's body until the contents in the bag could be visualized.10–12 In all cases morcellation was performed using scissors under direct vision, and the fragments of contents in the bag were removed piece by piece (Fig. 3). The umbilicus was irrigated with sterile water, and no drains were placed.
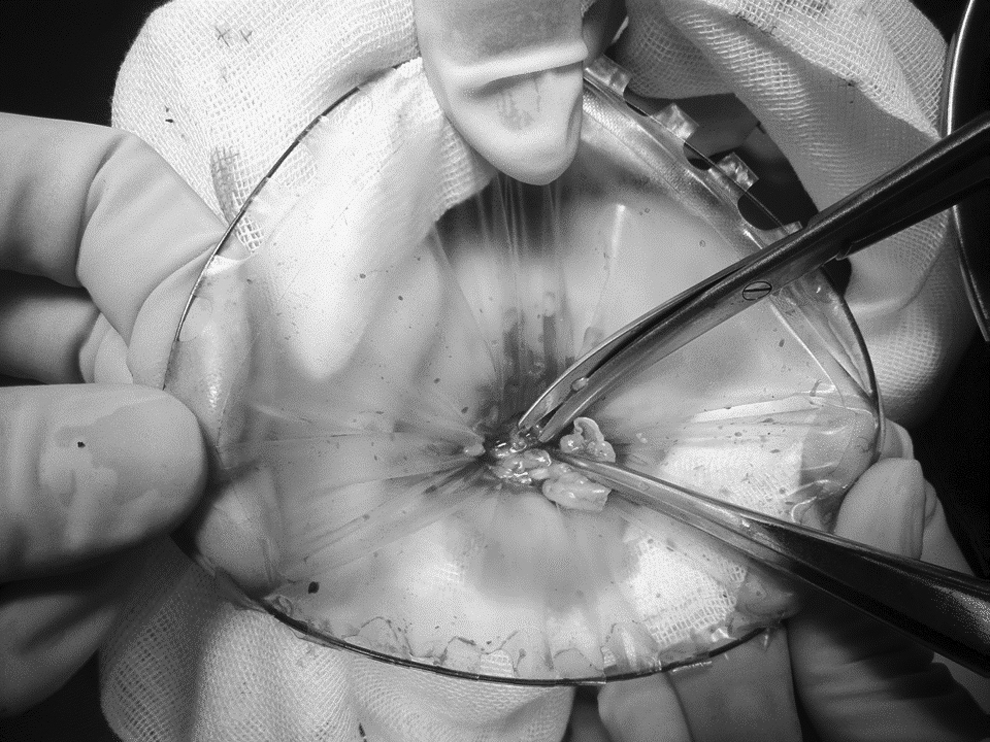
Morcellation of the specimen was performed through an enlarged umbilical incision under direct vision using scissors.
Results
Laparoscopy was performed successfully in 7 cases without conversion to the open procedure or incomplete resection.
The tumors and lymph node samples were removed completely into the EndoCatch II bag through the enlarged umbilical incision. The enlarged lymph nodes were found in the retroperitonium close to the aorta or vena cava in two children, but all the cases were negative for malignancy.
The mean operative time was 97 minutes (range, 75–15 minutes). The average blood loss was 13.5 mL (range, 5–30 mL), so no blood transfusion was administered in any case. Oral intake was restarted 24 hours after the orogastric tube was removed, and the mean time to full enteral feeds was 2.5 days (range, 2–4 days). The number of days until the initiation of postoperative chemotherapy was 6.5 days (range, 4–9 days). The median length of hospital stay was 8.5 days (range, 6–11 days [including the first cycle of postoperative chemotherapy]).
Histopathologic analysis revealed favorable WT in 5 cases (stage I, 4 cases; stage IV, 1 case), rhabdoid tumor in 1 case (stage III), and renal cell carcinoma in 1 case (stage I). Among the WTs, four were low-risk tumors, and one was a high-risk tumor, according to Children's Oncology Group risk staging. Six patients were treated completed by the chemotherapy and radiotherapy as recommended by the National Wilms Tumor Study-5. 7 The patient with renal cell carcinoma was followed up without chemotherapy or interferon-2α therapy. No viable tumor cells were found in the ureter.
With a median follow-up of 1.9±1.5 years (range, 0.3–2.9 years), 6 of the 7 patients were in complete remission without evidence of disease; 1 patient was lost to follow-up. The cosmetic result in the 6 cases with follow-up was satisfactory by parental reports (Fig. 4). None of the patients presented evidence of oncological complications (tumor recurrences in LRN, port-site implantation, or secondary lung metastases), and no small bowel obstruction occurred.

Cosmetic results at 3 months postoperatively.
Discussion
After the first description in 1991, 13 LRN has become the standard surgical procedure for stage T1/T2 renal cancer in adults. Some reports, which include over 100 cases in studies from multiple institutions, have proved the efficacy and safety of LRN in adult patients with renal cancer. 1 Also, LRN has been well recognized as successful even for aggressive malignant renal tumors in the early stage.2,14 Classically, open radical nephrectomy performed through either a chevron or a transverse abdominal incision and regional lymph node sampling is still considered as the standard treatment for malignant renal tumors in most children's hospitals, which requires long and deep incisions with a long recovery period. In recent years, selected case reports and small cases series have demonstrated the safety and feasibility of LRN for WT or other renal cancer in children; however, data regarding LRN for children in the English literature are still scarce, and prospective multicenter studies with a long period of follow-up have rarely been seen in the children's literature.3–6
The role of LRN in the treatment of renal tumor should be based on oncologic surgical principles, which are the same as that of open radical nephrectomy1,6,7: complete inspection of the abdominal cavity, lymph node sampling, and complete tumor resection without neoplastic cell spillage. In the experience with adults, contraindications include vena cava thrombosis, adhesions to other organs, initial tumor rupture, and surgical history.5,6 But in 2013, Xu et al. 15 reported a case of WT with renal vein tumor thrombus was successfully treated laparoscopically with only a three-port procedure. Javid et al. 4 also noted complete removal of WT with peritoneal implants by LRN in children, especially those deep in the pelvis.
The performance of LRN in children has been following the trail of adult surgery. In the beginning, the tumor size has been considered an important aspect for LRN. Some authors confirmed that the LRN was only efficacious for tumors up to 5 cm in the past 10 years. But recently, a summary of a multicenter study of 222 adult patients has provided findings that tumors>7 cm in size can be safely and efficaciously removed by LRN for renal cell carcinoma. 16 In our preliminary experience, all the LRNs in children could be completed successfully when the tumor did not cross the midline on the computed tomography scan, even for 1 case whose tumor size was 10 cm in diameter at the time of surgery. Nowadays, most laparoscopic surgeons have concluded that performing LRN on a patient with a tumor that extends across the lateral edge of the vertebra is an unsafe procedure because the tumor could not be removed easily for this case, with a higher probability of open conversion and also with a higher risk of tumor rupture, even it may have been possible to add a fourth or fifth trocar to facilitate the procedure.6,17 If tumor spillage or rupture happened in LRN, the tumor stage and the risk of seeding could increase, obviously associated with an adverse outcome.
For those cases with tumor size that crosses the midline, several cycles of preoperative chemotherapy were necessary to shrink the tumor. In cases of WT, preoperative chemotherapy based on the International Society of Pediatric Oncology protocols has been recommended always by some laparoscopic surgeons because it is able to induce remarkable tumor shrinkage and decrease the incidence of tumor rupture. 18 Laparoscopic tumor rupture is feared by many surgeons; it has been shown to occur during open radical nephrectomy in 2.8% of cases in the International Society of Pediatric Oncology-93 protocol after preoperative chemotherapy and in 11% of cases in the National Wilms Tumor Study-4 protocol 19 without preoperative chemotherapy. Likewise, in our preliminary experience, there was no temporal rupture or spillage in all 7 cases, in which 3 patients underwent preoperative chemotherapy, and the tumor size shrank sharply.
We should indicate that it was possible that the advanced tumors in the 3 patients could be resected by initial conventional opening nephroureterectomy according to the Children's Oncology Group protocols. But, the patients received preoperative chemotherapy from the Children's Oncology Group regimen based on the histological confirmation by fine-needle biopsy only for the LRN procedure. Such a procedure has also been adopted by some surgeons following Children's Oncology Group protocols in the literature. 4 Thus the complete resection without microscopic residue or any spillage could be achieved in LRN if the surgeon has appropriate training in both endosurgery and surgical oncology.3–6
LRN for a renal malignant tumor can be performed via transperitoneal or retroperitoneal approaches.1–6 Each approach has its own advantages and limitations. A systematic review and meta-analysis of the available information published 20 in the adult literature compared the outcomes of the two approaches, and the definitive conclusions were that there were no differences on the efficacy and safety of these two methods. In our own series, all the cases were performed by the transperitoneal approach, the same as other pediatric laparoscopic surgeons.
There are also two methods of specimen removal in LRN. One is adding a low suprapubic incision, through which the tumor is placed in a bag and extracted without morcellation. This method minimizes the risk of tumor rupture and allows adequate visualization of the total tumor margin and an accurate histological definition of the tumor, but the added suprapubic incision is used only for removal of tumor and increases the postoperative pain.5,6 Another method is performed through an extension of one of the port sites, usually through the umbilicus, after the tumor is introduced into an endoscopic bag. This procedure is accomplished via minimally invasive techniques, but the morcellation may cause breakage of the endoscopic bag and lead to further dissemination of the tumor within the abdominal cavity.10,11 In our preliminary experience, the morcellation was performed using scissors under direct vision, and the fragments of the contents were removed piece by piece from the endoscopic bag without any breakage of the bag or tumor plantation via an enlarged umbilical incision. The umbilical incision should be enlarged enough to retract out the contents in the bag, such as the morcellated tumor, the ureter, and the lymph node, sequentially. 12
The sampling of lymph nodes in the peritoneum is a very important indicator for accurate staging of WT in children. 7 But, there still has been controversy on the survival rates of patients and the number of lymph nodes examined in WT. Zhuge et al. 21 reported that the relationship between the lymph node data and the 5-year survival rate from 1340 patients with WT was as follows: with no lymph nodes sampled, 87%; 1–5 lymph nodes sampled, 91%; 6–10 lymph nodes, 93%; and more than 10 lymph nodes, 95%. From this study, the more lymph nodes were sampled, the better the prognosis of the patients. In contrast, Kieran et al. 9 recently found that the number of lymph nodes in the peritoneum did not predict the 5-year event-free survival variations among 3409 patients; the significance of lymph node positivity was greater only for patients with anaplastic WT. They concluded that extensive lymph node dissection seems unnecessary in the patient with negative hilar lymph nodes.
In the adult literature, the incidence of total complications of LRN was 8%–37% from multicenter studies but was as high as 24%–55% in the opening procedure in T1/T2 renal cell carcinoma.1,8 The results also promote the application of LRN in pediatric oncology. For instance, adhesive small bowel obstruction is one of the most common postoperative complications after radical nephrectomy for WT in open surgery: the incidence was 5.4% reported in the National Wilms Tumor Study-3, 22 and postoperative intussusceptions occurred in 1.1% of patients in the International Society of Pediatric Oncology study. 23 Until now, no adhesive small bowel obstructions or intussusceptions have been described after LRN of renal tumors in the pediatric literature, even though the number of cases is small, and the period of follow-up is limited, so that definitive conclusion cannot be drawn. It is the main benefit for numerous patients who have received laparoscopy. The other benefits of LRN for patients were a more comfortable postoperative course, a better cosmetic result on the abdominal wall, and quick discharge, at Day 2 or 3, in the pediatric literature.5,6 In our study, the average time of hospitalization was 8.5 days, during which the preoperative examinations and the first cycle of postoperative chemotherapy were involved. So LRN results in more rapid recovery of patients than the conventional open procedure.
In conclusion, LRN in children with WT or other renal cancers may be considered as an option in selected patients and can be safely performed by laparoscopic surgeons. For trained laparoscopic surgeons, the indication of LRN is the tumors do not cross the midline at the time of surgery. Preoperative chemotherapy is essential to decrease tumor size and to facilitate the dissection, avoiding tumor rupture. However, multicenter prospective studies with long follow-up and more cases are necessary to evaluate the results of minimally invasive surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.