
Abstract
Abstract
Aim:
To study the outcomes after endoscopic treatment of chronic foreign bodies (FBs) in the airway.
Materials and Methods:
A retrospective study (2008–2013) of 20 cases with chronic airway FBs (>2 weeks) was done with emphasis on endoscopic management. All cases were initially evaluated by the pediatric pulmonologist. Flexible and rigid bronchoscopy was done for diagnosis and retrieval, respectively. The techniques of FB retrieval, problems encountered, and their solutions were analyzed. Follow-up flexible bronchoscopy was done in symptomatic cases. Outcomes were assessed in terms of successful removal of the FB, clinical recovery, lung expansion, and need for further procedures.
Results:
Twenty cases (16 boys, 4 girls) with a mean age of 7 years had a chronic airway FB diagnosed on chest X-ray (n=6) and flexible bronchoscopy (n=14). Six cases had computed tomography evaluation. On rigid bronchoscopy, the FB was successfully retrieved in 16 cases. Two cases required open surgery for FB-induced tracheoesophageal fistula. One case required pneumonectomy because of a battery eroding into the lung parenchyma. One patient died. Of the 16 who had successful retrieval, 11 recovered with full lung expansion. Four recovered after additional bronchoscopic procedures (cauterization of granulation [n=2] and balloon dilatation of bronchial stenoses [n=2]). One case required pneumonectomy for persistent collapse despite multiple dilatations.
Conclusions:
An airway FB producing chronic respiratory symptoms may be missed because of lack of definite history of an inhaled FB. Clinical suspicion and flexible bronchoscopy are instrumental in diagnosis. Treatment is challenging because of chronicity-related complications and requires innovative ideas to make best use of the available urologic and bronchoscopic equipment. Addition of tracheotomy provides safety in difficult cases. Bronchoscopic removal leads to clinical and radiological recovery in most cases.
Introduction
P
This article presents the 6-year experience of chronic FBs in the airway from a developing country. We highlight the role of flexible bronchoscopy for diagnosis and of rigid bronchoscopy for retrieval. Innovative ideas and improvisations in instrumentation are stressed. Use of tracheotomy to make the procedure safe is illustrated. Long-standing FBs may cause life-threatening complications such as tracheoesophageal fistula and complete lung loss. Their management approach is also presented.
Materials and Methods
Records of cases that were treated for a chronic airway FB over a 6-year period (2008–2013) at a tertiary-care center were retrospectively reviewed. Data were collected regarding demographics, duration of symptoms, history of inhalation of FB, examination findings, results of radiological studies (chest X-ray and computed tomography [CT]), findings on flexible bronchoscopy, and surgical management.
Cases presenting with chronic respiratory symptoms (more than 2 weeks) with or without history of FB aspiration were initially evaluated by a pediatric pulmonologist (G.R.S.). After a thorough history and physical examination, flexible bronchoscopy using a 2.5-mm/3.5-mm videoscope (Karl Storz, Tuttlingen, Germany) was done.
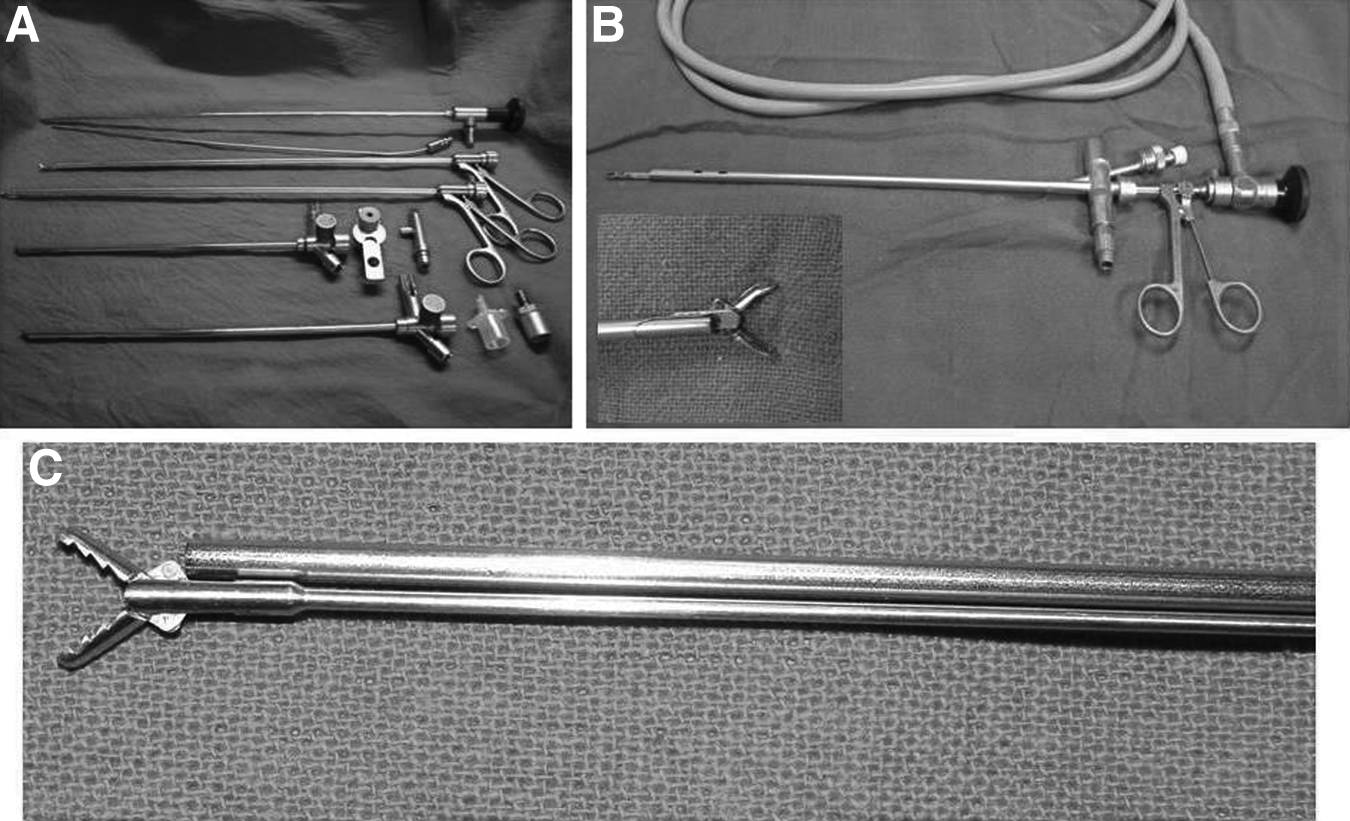
If an FB was diagnosed, the case was referred to a pediatric surgeon (S.K.A.) for rigid bronchoscopy and further management. CT scan of the chest (Fig. 1) was obtained in selected cases with chronic collapse or clinical suspicion of bronchiectasis. Rigid bronchoscopy (Karl Storz) was performed by the senior pediatric surgeon (S.K.A.) with the patient under general anesthesia—with conventional or jet ventilation as per the anesthetist's preference. An age-appropriate sheath and telescopes with videoscopic camera were used (Fig. 2). A record was made regarding nature and location of FB, condition of the airway (granulation, inflammation, erosion, ulceration, bleeding, etc.), impaction of FB, the technique of retrieval, problems encountered, and their solutions. If possible, the FB was retrieved using different maneuvers. If impacted, it was disimpacted first before maneuvering. Tracheotomy was used to retrieve large FBs with chronic collapse of the ipsilateral lung—as a safeguard to prevent slippage and impaction in the contralateral good side. When it was not considered safe, the procedure was terminated, and open retrieval of FB was carried out. Pneumonectomy was reserved for select cases.

Computed tomography scan showing bronchiectasis. The bronchiectasis resolved after 3 months of removal of the foreign body.
Follow-up was aimed at confirming clinical resolution and radiological expansion of lung. Persistent problems in lung expansion, granulation, and bronchial stenosis led to further procedures—both open and endoscopic. The management algorithm is shown in Figure 3.
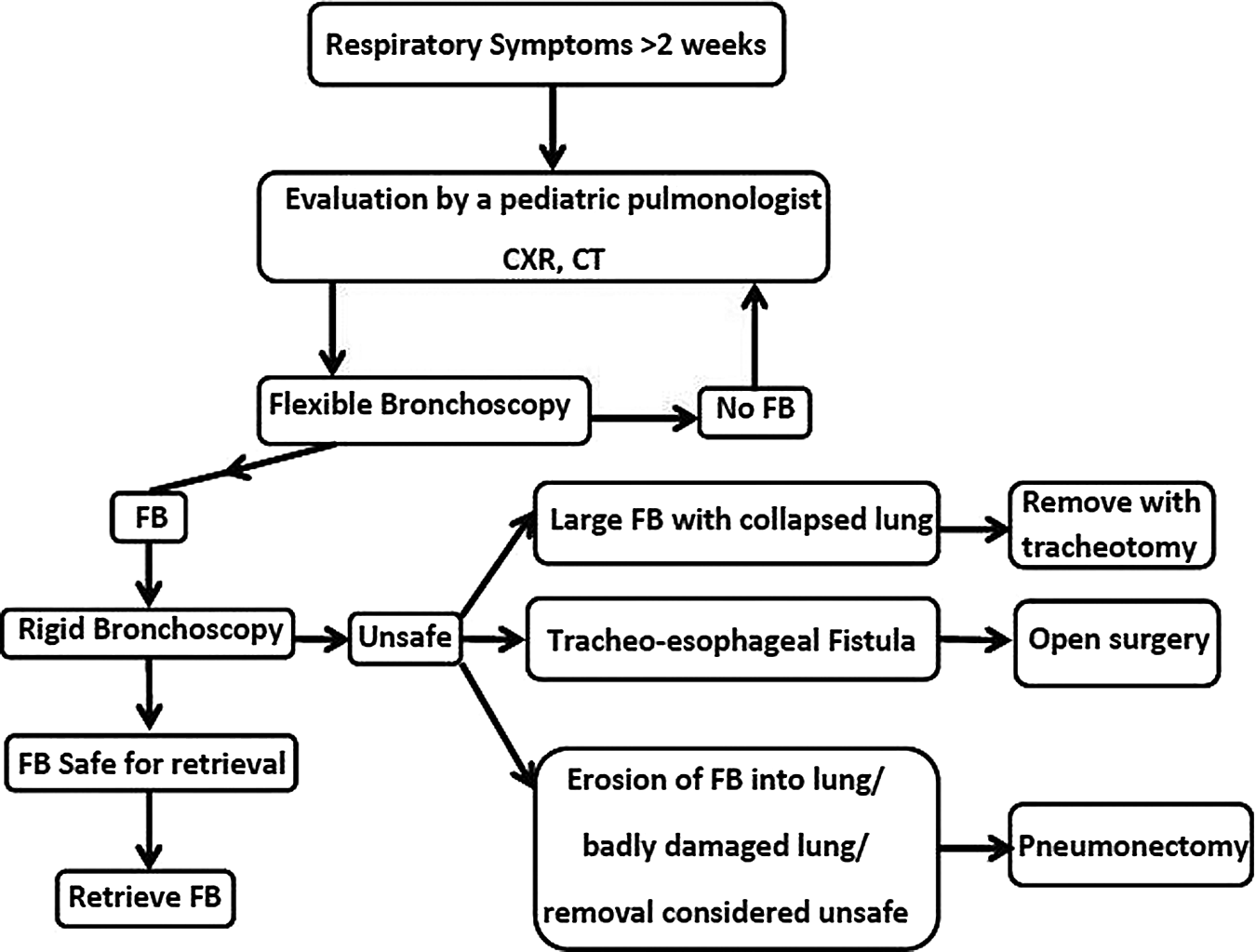
Management algorithm. CT, computed tomography; CXR, chest X-ray; FB, foreign body.
Outcomes were assessed in terms of successful removal of FB, expansion of lung, need for further treatment, and resolution of symptoms.
Results
In total, 20 cases were selected. There were 16 boys and 4 girls in the age range of 10 months–12 years (mean, 7 years). The median duration of symptoms was 11 months with a range from 2 weeks to 2 years. History of an aspiration event being witnessed by a responsible adult was not forthcoming at all in 11, whereas in 9 it was doubtful. Cough was the predominant symptom, followed by tachypnea, noisy breathing, fever, and episodes of violent cough with cyanosis. All of them had received antibiotics, bronchodilators, and over-the-counter cough syrups. Seven patients had previously been hospitalized elsewhere for treatment of “pneumonia.” Eight cases had received full or partial antitubercular treatment. Fifteen had received steroids. Prominent examination findings were decreased air entry (n=15), respiratory distress (n=4), fixed respiratory cycle sound (n=7), loss of volume on ipsilateral chest (n=3), crepitation (n=4), and features of bronchiectasis (n=3).
Chest X-ray showed a radio-opaque FB in 6 cases and hypertrophied lung in 5 cases with contralateral complete or partial collapse. Six cases had partial collapse of a lobe on the ipsilateral side. In 9 cases chest X-ray was normal. CT of the chest was done in 6 cases; all showed varying degrees of collapse, with bronchiectasis in 4. The 6 cases in which the FB was seen on chest X-ray were referred for rigid bronchoscopy straightaway without flexible bronchoscopy. In the remaining 14 cases, diagnostic flexible bronchoscopy was carried out by a pediatric pulmonologist (G.R.S.).
The nature of FB was vegetable matter (seeds, peanut, almond, coconut, beetle nut, tamarind seed, etc.) in 10 cases, plastic material in 4 cases, and metallic in 6 cases (seen on chest X-ray). The FB was located in the right main bronchus in 7 cases, left main bronchus in 7 cases, basilar left bronchus in 2 cases, and basilar right in 2 cases. A tracheoesophageal fistula was found in 2 cases on flexible bronchoscopy: they had a FB partly in the esophagus and partly in the trachea.
Rigid bronchoscopy
Rigid bronchoscopy was performed by the senior pediatric surgeon (S.K.A.) in all 20 cases in the operating room. Initial inspection was done to assess the airway, the presence or absence of secretions, pus, granulations, and impaction, and the condition of the contralateral side. For sharp objects like drawing pins, nails, etc., a plan was made to safely remove them without damaging the airway. To remove the FB, an optical forceps (Karl Storz) with soft peanut cups was used for free-lying vegetable FBs. For impacted FBs an improvised optical forceps (Fig. 2C and 4) was used: the telescope was passed by the side of a nonoptical sturdy forceps to maneuver the FB under vision. The widest possible sheath was used in these cases to allow simultaneous entry of the telescope and the forceps. Bronchial lavage was intermittently done to improve visibility and clear the blood and secretions. Retrieval at the level of vocal cords was watched under vision very carefully. If the FB was big or slippery and the ipsilateral lung was nearly completely collapsed, retrieval through the glottis was not considered safe. In this scenario the FB was held firmly with the forceps, withdrawn to the mid-trachea, and retrieved through a swift tracheotomy. The site of tracheotomy was guided by the light of the telescope, and it was done exactly opposite to where the FB was held in the trachea by the telescopic forceps. The procedure was coordinated well between the tracheotomy team and the bronchoscopy team for smooth execution with minimum hypoxia. Tracheotomy was primarily closed in 1 case, but a tracheostomy tube was left in the other. Decannulation was done a week later.
Improvised forceps being used to disimpact and remove a pen cap from the bronchus.
Outcomes
The outcomes were as follows: successful retrieval of FB without tracheotomy, n=14; successful retrieval of FB with tracheotomy, n=2; tracheoesophageal fistula treated by open operation, n=2; and battery in the left bronchus with erosion into lung parenchyma followed by pneumonectomy, n=1. One child died during bronchoscopy because of dislodgement of the FB into the opposite normal bronchus leading to respiratory arrest.
Follow-up and follow-up procedures
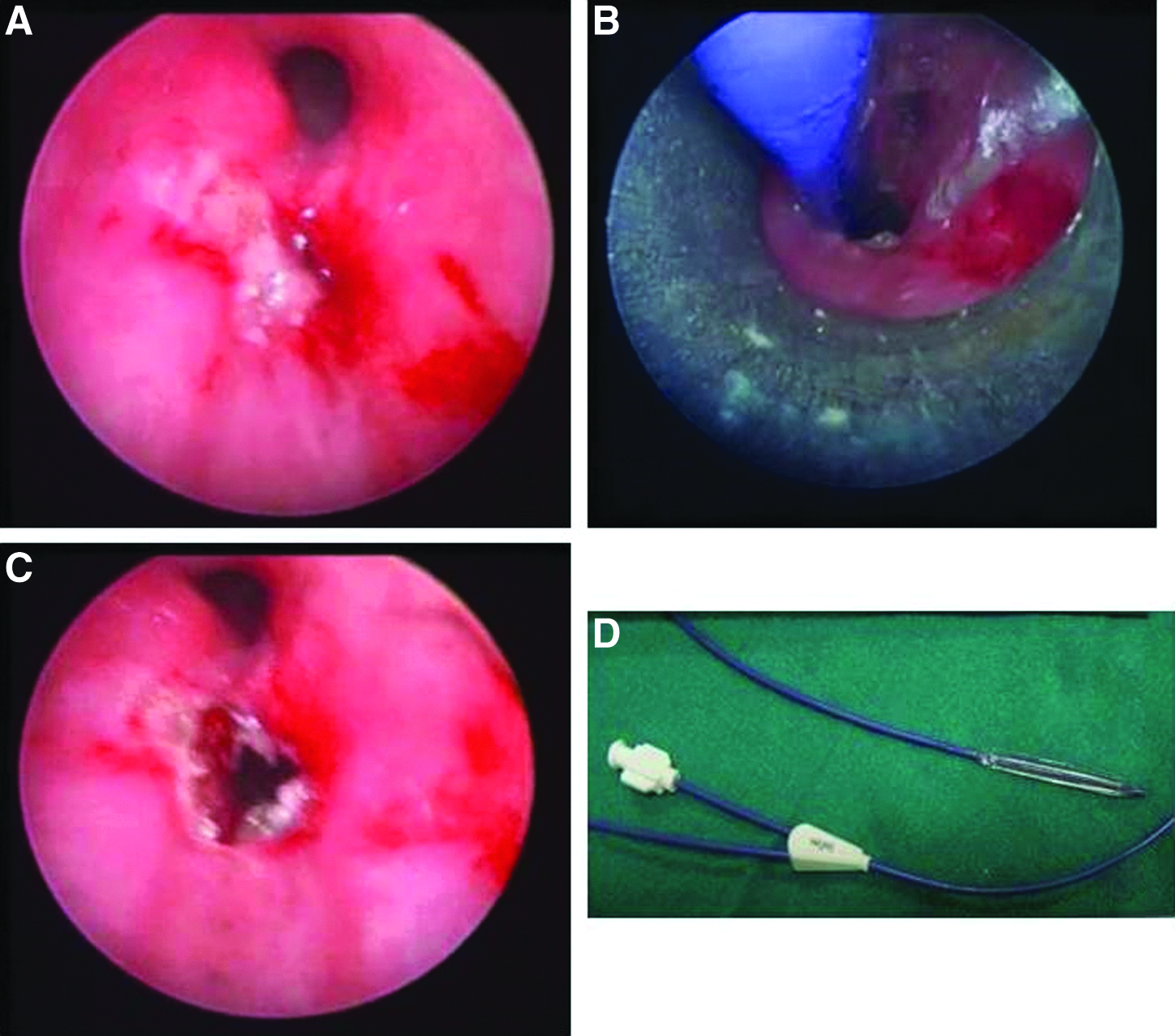
The follow-up was 1–6 years (average, 3.5 years). Of the 16 who had successful retrieval, 11 recovered completely with full lung expansion after a mean duration of 3 months. Four had persistent collapse due to residual granulation and/or bronchial stenosis as diagnosed on flexible bronchoscopy; they underwent rigid bronchoscopy again, and the granulations were cauterized and stenoses dilated using balloon dilators using ureteric dilators (Bard Force®; C.R. Bard, Inc., Covington, GA) (Fig. 5). All of them recovered on follow-up with full lung expansion. One patient required a pneumonectomy because of persistent collapse despite removal of the FB and multiple dilatations.
Discussion
Long-standing FB in respiratory tract can lead to significant morbidity and even mortality. An eyewitness to the aspiration episode is not commonly present in these cases. In none of our cases was the history of eyewitness account present with certainty. In these patients the diagnosis of foreign body was delayed with concomitant delay in treatment.5,6 Symptoms such as cough, acute dyspnea, pneumonia, and findings on physical examination (unilateral or bilateral decreased air entry, flow, rhonchi, wheeze, or stridor) are thought to be of low sensitivity and specificity as they overlap with various pathological conditions. Most of these cases were managed initially by antibiotics and bronchodilators and were referred because of persistent or recurrent symptoms. An initial investigation that is ordered universally is a chest X-ray. Finding a radio-opaque FB is diagnostic and was found in 6 of our cases. The other features on chest X-ray are nonspecific. A normal chest X-ray does not rule out aspiration of FB. 7
Flexible bronchoscopy under sedation is the most specific and sensitive investigation and should be offered to all children with persistent and recurrent symptoms. 8 Advances in optical technology have led to development of miniature fiber optic flexible bronchoscopes. However, proper training and experience are crucial to optimize the outcome and minimize the risk of complications by a flexible bronchoscope. 9 Flexible bronchoscopy has been used and advocated for diagnosis of long-standing FB in clinical scenarios composed of non-resolving pneumonia, recurrent hemoptysis, lung fibrosis, obstructive emphysema, and bronchiectasis. 10 Although retrieval of the FB may be possible through flexible bronchoscopy, we do not advocate it because of risk of complications. 11 Although bronchoscopes with an outer diameter of 2.5–3.5 mm with 1.2-mm working channels may be suitable for retrieval of recently inhaled FBs in select cases, for chronic and impacted FBs we consider it unsafe and impractical. In such cases, rigid bronchoscopy with the patient under general anesthesia is probably the safest procedure. It allows better vision, larger working field, and ability to do suction and lavage and provides control over the FB through a good grip of a sturdy forceps. Furthermore, it provides a good control over ventilation. 12
Jet ventilation versus conventional ventilation
Jet ventilation provides an opportunity for uninterrupted time to the surgeon for the procedure. 13 However, the sudden jet of pressure could push the FB further and cause mist over the telescope. Also, if complete occlusion of the lumen of the endoscope occurs by telescope and forceps, it can increase airway pressures. With conventional ventilation the surgeon may have to stop the procedure intermittently to allow the anesthetist to improve oxygenation and allow CO2 washout. Pulse oximetry and capnography are essential monitoring devices during the procedure. A good coordination between the anesthetist and the surgeon is essential.
Tracheotomy
Very early in this experience there was a death. This child had a large plastic FB (piece of a toy) in the left main bronchus impacted for more than 18 months. His left lung had been completely collapsed. During bronchoscopy it was possible to disimpact the FB. While it was being maneuvering with the help of optical forceps across the glottis, it slipped and lodged in the right main bronchus, causing a sudden fall in saturation, and the anesthetist was unable to ventilate. The child died. From this case we learned a lesson that large FBs with chronic collapse of lung should be dealt with great caution. We now use an improvised assembly of a sturdy forceps with a good grip along with the telescope to hold these FBs. In addition, we do not attempt to maneuver them across the vocal cords. Instead, they are retrieved through a tracheotomy after maneuvering them to the mid-trachea. Although highly useful, use of tracheotomy is not emphasized much in the literature.14,15
Problems in a developing country
India is a developing country, and resource crunch may be a problem even at tertiary-care centers. In an ideal world, retrieval of FBs from the airways should not be attempted if adequate instrumentation is not available. At our center most equipment, including optical forceps, is available. Yet, the variety of cases and chronicity of them make it extremely difficult to manage them. Metallic FBs impacted beyond 1 or 2 years are very difficult to maneuver with delicate optical forceps. Our experience has resulted in tailor-made improvisation in the instrumentation. The use of a sturdy forceps passed alongside the telescope provides the benefit of both ease of grip and maneuvering under telescopic vision. Furthermore, the innovative use of urologic equipment such as a metallic ureteric catheter as an endoscopic cautery electrode and ureteric dilators as bronchial dilators provides other examples of improvisations.
Tracheoesophageal fistula and FB (2 cases)
These two cases deserve special mention because of their rarity. In 1 case, the fistula was caused by a gradual erosion of the esophagus and posterior wall of the trachea by a battery in the esophagus. Respiratory symptoms were aggravated when the fistulation occurred. It was diagnosed on bronchoscopy, but an open thoracotomy was done to retrieve the FB. A long segment of the esophagus was destroyed, requiring a gastric pull-up later. The trachea had a 1-cm hole in the posterior wall that required closure with a muscle flap from strap muscles through a neck incision. The patient recovered completely and is symptom free after a 2-year follow-up.
The other case was a neglected case of esophageal FB (a plastic ring) that eroded through the esophagus and trachea causing tracheoesophageal fistula. This patient required neck exploration, retrieval of FB through a posterior pharyngotomy, and closure of the esophagus and tracheal defects with interposition of soft tissue (Fig. 6). He recovered completely and is well after a 5-year follow-up.
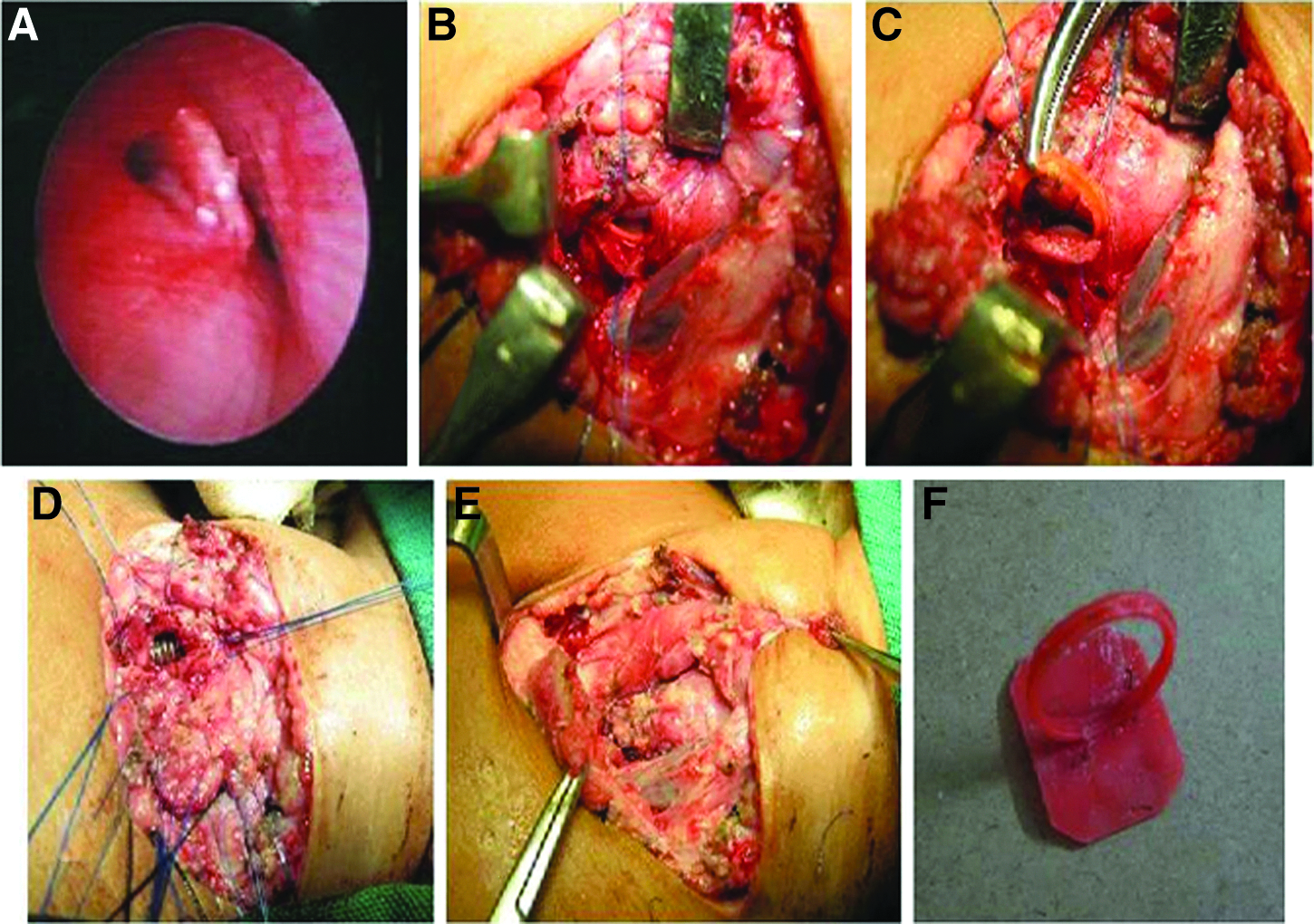
Open neck exploration for a chronic foreign body eroding through the esophagus.
Follow-up of FB removal
Of the 16 cases in which FBs were removed, 11 had complete expansion of lung within 3 months, whereas 4 had persistent collapse, and 1 needed pneumonectomy as the lung parenchyma was damaged and the patient had recurrent respiratory symptoms. In a large series, pneumonia followed by bronchiectasis was reported to be most common complication of long-term FB. 16 The exact duration required for the development of bronchiectasis after obstruction in humans is not known. It is also not known which of these will reverse. There are reports in the literature suggesting the resolution of bronchiectasis, scar changes, or atelectasis secondary to FB aspiration after the extracting of a long-standing retained FB.2,17 It is important to follow-up these patients by clinical examinations and chest X-ray. We advocate flexible bronchoscopy to check the status of granulation tissue in cases where the lung had not expanded, and depending upon the finding, dilatation, cauterization, etc., can be tried. This was successful in all of our cases.
Conclusions
Long-standing FB in the airway should be suspected if there are chronic respiratory symptoms even if there is no definite history, and flexible bronchoscopy should be offered for diagnosis. Bronchoscopic removal leads to reversal of lung changes in most cases. Follow-up bronchoscopy is essential to pick up complications like granulations and bronchial stenoses, which can be managed endoscopically.
Footnotes
Disclosure Statement
No competing financial interests exist.